

Biomedical engineer Kevin Zhao has a sensor in his arm and his chest that monitors his oxygen level in those tissues in real time.
Last month, at a conference celebrating DARPA, the research arm of the Defense Department, FBI Special Agent Edward You declared, "The 21st century will be the revolution of the life sciences."
Biomedical engineer Kevin Zhao has a sensor in his arm and chest that monitors his oxygen level in real time.
Indeed, four years ago, the agency dedicated a new office solely to advancing biotechnology. Its primary goal is to combat bioterrorism, protect U.S. forces, and promote warfighter readiness. But its research could also carry over to improve health care for the general public.
With an annual budget of about $3 billion, DARPA's employees oversee about 250 research and development programs, working with contractors from corporations, universities, and government labs to bring new technologies to life.
Check out these three current programs:
1) IMPLANTABLE SENSORS TO MEASURE OXYGEN, LACTATE, AND GLUCOSE LEVELS IN REAL TIME
Biomedical engineer Kevin Zhao has a sensor in his arm and his chest that monitors his oxygen level in those tissues in real time. With funding from DARPA for the program "In Vivo Nanoplatforms," he developed soft, flexible hydrogels that are injected just beneath the skin to perform the monitoring and that sync to a smartphone app to give the user immediate health insights.
A first-in-man trial for the glucose sensor is now underway in Europe for monitoring diabetics, according to Zhao. Volunteers eat sugary food to spike their glucose levels and prompt the monitor to register the changes.
"If this pans out, with approval from FDA, then consumers could get the sensors implanted in their core to measure their levels of glucose, oxygen, and lactate," Zhao said.
Lactate, especially, interests DARPA because it's a first responder molecule to the onset of trauma, sepsis, and potentially infection.
"The sensor could potentially detect rise of these [body chemistry numbers] and alert the user to prevent onset of dangerous illness."
2) NEAR INSTANTANEOUS VACCINE PROTECTION DURING A PANDEMIC
Traditional vaccines can take months or years to develop, then weeks to become effective once you get it. But when an unknown virus emerges, there's no time to waste.
This program, called P3, envisions a much more ambitious approach to stop a pandemic in its tracks.
"We want to confer near instantaneous protection by doing it a different way – enlist the body as a bioreactor to produce therapeutics," said Col. Matthew Hepburn, the program manager.
So how would it work?
To fight a pandemic, we will need 20,000 doses of a vaccine in 60 days.
If you have antibodies against a certain infection, you'll be protected against that infection. This idea is to discover the genetic code for the antibody to a specific pathogen, manufacture those pieces of DNA and RNA, and then inject the code into a person's arm so the muscle cells will begin producing the required antibodies.
"The amazing thing is that it actually works, at least in animal models," said Hepburn. "The mouse muscles made enough protective antibodies so that the mice were protected."
The next step is to test the approach in humans, which the program will do over the next two years.
But the hard part is actually not discovering the genetic code for highly potent antibodies, according to Hepburn. In fact, researchers already have been able to do so in two to four weeks' time.
"The hard part is once I have an antibody, a large pharma company will say in 2 years, I can make 100-200 doses. Give us 4 years to get to 20,000 doses. That's not good enough," Hepburn said.
To fight a pandemic, we will need 20,000 doses of a vaccine in 60 days.
"We have to fundamentally change the idea that it takes a billion dollars and ten years to make a drug," he concluded. "We're going to do something radically different."
3) RAPID DIAGNOSING OF PATHOGEN EXPOSURE THROUGH EPIGENETICS
Imagine that you come down with a mysterious illness. It could be caused by a virus, bacteria, or in the most extreme catastrophe, a biological agent from a weapon of mass destruction.
What if a portable device existed that could identify--within 30 minutes—which pathogen you have been exposed to and when? It would be pretty remarkable for soldiers in the field, but also for civilians seeking medical treatment.
This is the lofty ambition of a DARPA program called Epigenetic Characterization and Observation, or ECHO.
Its success depends on a biological phenomenon known as the epigenome. While your DNA is relatively immutable, your environment can modify how your DNA is expressed, leaving marks of exposure that register within seconds to minutes; these marks can persist for decades. It's thanks to the epigenome that identical twins – who share identical DNA – can differ in health, temperament, and appearance.

These three mice are genetically identical. Epigenetic differences, however, result in vastly different observed characteristics.
Reading your epigenetic marks could theoretically reveal a time-stamped history of your body's environmental exposures.
Researchers in the ECHO program plan to create a database of signatures for exposure events, so that their envisioned device will be able to quickly scan someone's epigenome and refer to the database to sort out a diagnosis.
"One difficult part is to put a timestamp on this result, in addition to the sign of which exposure it was -- to tell us when this exposure happened," says Thomas Thomou, a contract scientist who is providing technical assistance to the ECHO program manager.
Other questions that remain up in the air for now: Do all humans have the same epigenetic response to the same exposure events? Is it possible to distinguish viral from bacterial exposures? Does dose and duration of exposure affect the signature of epigenome modification?
The program will kick off in January 2019 and is planned to last four years, as long as certain milestones of development are reached along the way. The desired prototype would be a simple device that any untrained person could operate by taking a swab or a fingerprick.
"In an outbreak," says Dr. Thomou, "it will help everyone on the ground immediately to have a rapidly deployable machine that will give you very quick answers to issues that could have far-reaching ramifications for public health safety."

Jamie Rettinger with his now fiance Amie Purnel-Davis, who helped him through the clinical trial.
Melanoma is the deadliest form of skin cancer. About 85,000 people are diagnosed with it each year in the U.S. and more than 8,000 die of the cancer when it spreads to other parts of the body, according to the Centers for Disease Control and Prevention (CDC).
There are two peaks in diagnosis of melanoma; one is in younger women ages 30-40 and often is tied to past use of tanning beds; the second is older men 60+ and is related to outdoor activity from farming to sports. Light-skinned people have a twenty-times greater risk of melanoma than do people with dark skin.
"When I graduated from medical school, in 2005, melanoma was a death sentence" --Diwakar Davar.
Jamie had a follow up PET scan about six months after his surgery. A suspicious spot on his lung led to a biopsy that came back positive for melanoma. The cancer had spread. Treatment with a monoclonal antibody (nivolumab/Opdivo®) didn't prove effective and he was referred to the UPMC Hillman Cancer Center in Pittsburgh, a four-hour drive from his home in western Ohio.
An alternative monoclonal antibody treatment brought on such bad side effects, diarrhea as often as 15 times a day, that it took more than a week of hospitalization to stabilize his condition. The only options left were experimental approaches in clinical trials.
Early research
"When I graduated from medical school, in 2005, melanoma was a death sentence" with a cure rate in the single digits, says Diwakar Davar, 39, an oncologist at UPMC Hillman Cancer Center who specializes in skin cancer. That began to change in 2010 with introduction of the first immunotherapies, monoclonal antibodies, to treat cancer. The antibodies attach to PD-1, a receptor on the surface of T cells of the immune system and on cancer cells. Antibody treatment boosted the melanoma cure rate to about 30 percent. The search was on to understand why some people responded to these drugs and others did not.
At the same time, there was a growing understanding of the role that bacteria in the gut, the gut microbiome, plays in helping to train and maintain the function of the body's various immune cells. Perhaps the bacteria also plays a role in shaping the immune response to cancer therapy.
One clue came from genetically identical mice. Animals ordered from different suppliers sometimes responded differently to the experiments being performed. That difference was traced to different compositions of their gut microbiome; transferring the microbiome from one animal to another in a process known as fecal transplant (FMT) could change their responses to disease or treatment.
When researchers looked at humans, they found that the patients who responded well to immunotherapies had a gut microbiome that looked like healthy normal folks, but patients who didn't respond had missing or reduced strains of bacteria.
Davar and his team knew that FMT had a very successful cure rate in treating the gut dysbiosis of Clostridioides difficile, a persistant intestinal infection, and they wondered if a fecal transplant from a patient who had responded well to cancer immunotherapy treatment might improve the cure rate of patients who did not originally respond to immunotherapies for melanoma.
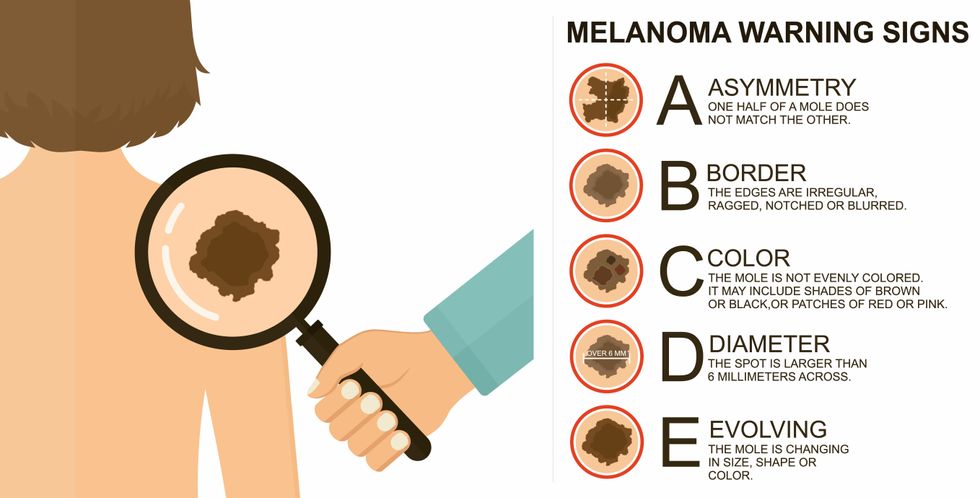
The ABCDE of melanoma detection
Adobe Stock
Clinical trial
"It was pretty weird, I was totally blasted away. Who had thought of this?" Jamie first thought when the hypothesis was explained to him. But Davar's explanation that the procedure might restore some of the beneficial bacterial his gut was lacking, convinced him to try. He quickly signed on in October 2018 to be the first person in the clinical trial.
Fecal donations go through the same safety procedures of screening for and inactivating diseases that are used in processing blood donations to make them safe for transfusion. The procedure itself uses a standard hollow colonoscope designed to screen for colon cancer and remove polyps. The transplant is inserted through the center of the flexible tube.
Most patients are sedated for procedures that use a colonoscope but Jamie doesn't respond to those drugs: "You can't knock me out. I was watching them on the TV going up my own butt. It was kind of unreal at that point," he says. "There were about twelve people in there watching because no one had seen this done before."
A test two weeks after the procedure showed that the FMT had engrafted and the once-missing bacteria were thriving in his gut. More importantly, his body was responding to another monoclonal antibody (pembrolizumab/Keytruda®) and signs of melanoma began to shrink. Every three months he made the four-hour drive from home to Pittsburgh for six rounds of treatment with the antibody drug.
"We were very, very lucky that the first patient had a great response," says Davar. "It allowed us to believe that even though we failed with the next six, we were on the right track. We just needed to tweak the [fecal] cocktail a little better" and enroll patients in the study who had less aggressive tumor growth and were likely to live long enough to complete the extensive rounds of therapy. Six of 15 patients responded positively in the pilot clinical trial that was published in the journal Science.
Davar believes they are beginning to understand the biological mechanisms of why some patients initially do not respond to immunotherapy but later can with a FMT. It is tied to the background level of inflammation produced by the interaction between the microbiome and the immune system. That paper is not yet published.
Surviving cancer
It has been almost a year since the last in his series of cancer treatments and Jamie has no measurable disease. He is cautiously optimistic that his cancer is not simply in remission but is gone for good. "I'm still scared every time I get my scans, because you don't know whether it is going to come back or not. And to realize that it is something that is totally out of my control."
"It was hard for me to regain trust" after being misdiagnosed and mistreated by several doctors he says. But his experience at Hillman helped to restore that trust "because they were interested in me, not just fixing the problem."
He is grateful for the support provided by family and friends over the last eight years. After a pause and a sigh, the ruggedly built 47-year-old says, "If everyone else was dead in my family, I probably wouldn't have been able to do it."
"I never hesitated to ask a question and I never hesitated to get a second opinion." But Jamie acknowledges the experience has made him more aware of the need for regular preventive medical care and a primary care physician. That person might have caught his melanoma at an earlier stage when it was easier to treat.
Davar continues to work on clinical studies to optimize this treatment approach. Perhaps down the road, screening the microbiome will be standard for melanoma and other cancers prior to using immunotherapies, and the FMT will be as simple as swallowing a handful of freeze-dried capsules off the shelf rather than through a colonoscopy. Earlier this year, the Food and Drug Administration approved the first oral fecal microbiota product for C. difficile, hopefully paving the way for more.
An older version of this hit article was first published on May 18, 2021
