
Abortions Before Fetal Viability Are Legal: Might Science and the Change on the Supreme Court Undermine That?

The United States Supreme Court Building in Washington, D.C.
This article is part of the magazine, "The Future of Science In America: The Election Issue," co-published by LeapsMag, the Aspen Institute Science & Society Program, and GOOD.
Viability—the potential for a fetus to survive outside the womb—is a core dividing line in American law. For almost 50 years, the Supreme Court of the United States has struck down laws that ban all or most abortions, ruling that women's constitutional rights include choosing to end pregnancies before the point of viability. Once viability is reached, however, states have a "compelling interest" in protecting fetal life. At that point, states can choose to ban or significantly restrict later-term abortions provided states allow an exception to preserve the life or health of the mother.
This distinction between a fetus that could survive outside its mother's body, albeit with significant medical intervention, and one that could not, is at the heart of the court's landmark 1973 decision in Roe v. Wade. The framework of viability remains central to the country's abortion law today, even as some states have passed laws in the name of protecting women's health that significantly undermine Roe. Over the last 30 years, the Supreme Court has upheld these laws, which have the effect of restricting pre-viability abortion access, imposing mandatory waiting periods, requiring parental consent for minors, and placing restrictions on abortion providers.
Viability has always been a slippery notion on which to pin legal rights.
Today, the Guttmacher Institute reports that more than half of American women live in states whose laws are considered hostile to abortion, largely as a result of these intrusions on pre-viability abortion access. Nevertheless, the viability framework stands: while states can pass pre-viability abortion restrictions that (ostensibly) protect the health of the woman or that strike some kind a balance between women's rights and fetal life, it is only after viability that they can completely favor fetal life over the rights of the woman (with limited exceptions when the woman's life is threatened). As a result, judges have struck down certain states' so-called heartbeat laws, which tried to prohibit abortions after detection of a fetal heartbeat (as early as six weeks of pregnancy). Bans on abortion after 12 or 15 weeks' gestation have also been reversed.
Now, with a new Supreme Court Justice expected to be hostile to abortion rights, advances in the care of preterm babies and ongoing research on artificial wombs suggest that the point of viability is already sooner than many assume and could soon be moved radically earlier in gestation, potentially providing a legal basis for earlier and earlier abortion bans.
Viability has always been a slippery notion on which to pin legal rights. It represents an inherently variable and medically shifting moment in the pregnancy timeline that the Roe majority opinion declined to firmly define, noting instead that "[v]iability is usually placed at about seven months (28 weeks) but may occur earlier, even at 24 weeks." Even in 1977, this definition was an optimistic generalization. Every baby is different, and while some 28-week infants born the year Roe was decided did indeed live into adulthood, most died at or shortly after birth. The prognosis for infants born at 24 weeks was much worse.
Today, a baby born at 28 weeks' gestation can be expected to do much better, largely due to the development of surfactant treatment in the early 1990s to help ease the air into babies' lungs. Now, the majority of 24-week-old babies can survive, and several very premature babies, born just shy of 22 weeks' gestation, have lived into childhood. All this variability raises the question: Should the law take a very optimistic, if largely unrealistic, approach to defining viability and place it at 22 weeks, even though the overall survival rate for those preemies remains less than 10% today? Or should the law recognize that keeping a premature infant alive requires specialist care, meaning that actual viability differs not just pregnancy-to-pregnancy but also by healthcare facility and from country to country? A 24-week premature infant born in a rural area or in a developing nation may not be viable as a practical matter, while one born in a major U.S. city with access to state-of-the-art care has a greater than 70% chance of survival. Just as some extremely premature newborns survive, some full-term babies die before, during, or soon after birth, regardless of whether they have access to advanced medical care.
To be accurate, viability should be understood as pregnancy-specific and should take into account the healthcare resources available to that woman. But state laws can't capture this degree of variability by including gestation limits in their abortion laws. Instead, many draw a somewhat arbitrary line at 22, 24, or 28 weeks' gestation, regardless of the particulars of the pregnancy or the medical resources available in that state.
As variable and resource-dependent as viability is today, science may soon move that point even earlier. Ectogenesis is a term coined in 1923 for the growth of an organism outside the body. Long considered science fiction, this technology has made several key advances in the past few years, with scientists announcing in 2017 that they had successfully gestated premature lamb fetuses in an artificial womb for four weeks. Currently in development for use in human fetuses between 22 and 23 weeks' gestation, this technology will almost certainly seek to push viability earlier in pregnancy.
Ectogenesis and other improvements in managing preterm birth deserve to be celebrated, offering new hope to the parents of very premature infants. But in the U.S., and in other nations whose abortion laws are fixed to viability, these same advances also pose a threat to abortion access. Abortion opponents have long sought to move the cutoff for legal abortions, and it is not hard to imagine a state prohibiting all abortions after 18 or 20 weeks by arguing that medical advances render this stage "the new viability," regardless of whether that level of advanced care is available to women in that state. If ectogenesis advances further, the limit could be moved to keep pace.
The Centers for Disease Control and Prevention reports that over 90% of abortions in America are performed at or before 13 weeks, meaning that in the short term, only a small number women would be affected by shifting viability standards. Yet these women are in difficult situations and deserve care and consideration. Research has shown that women seeking later terminations often did not recognize that they were pregnant or had their dates quite wrong, while others report that they had trouble accessing a termination earlier in pregnancy, were afraid to tell their partner or parents, or only recently received a diagnosis of health problems with the fetus.
Shifts in viability over the past few decades have already affected these women, many of whom report struggling to find a provider willing to perform a termination at 18 or 20 weeks out of concern that the woman may have her dates wrong. Ever-earlier gestational limits would continue this chilling effect, making doctors leery of terminating a pregnancy that might be within 2–4 weeks of each new ban. Some states' existing gestational limits on abortion are also inconsistent with prenatal care, which includes genetic testing between 12 and 20 weeks' gestation, as well as an anatomy scan to check the fetus's organ development performed at approximately 20 weeks. If viability moves earlier, prenatal care will be further undermined.
Perhaps most importantly, earlier and earlier abortion bans are inconsistent with the rights and freedoms on which abortion access is based, including recognition of each woman's individual right to bodily integrity and decision-making authority over her own medical care. Those rights and freedoms become meaningless if abortion bans encroach into the weeks that women need to recognize they are pregnant, assess their options, seek medical advice, and access appropriate care. Fetal viability, with its shifting goalposts, isn't the best framework for abortion protection in light of advancing medical science.
Ideally, whether to have an abortion would be a decision that women make in consultation with their doctors, free of state interference. The vast majority of women already make this decision early in pregnancy; the few who come to the decision later do so because something has gone seriously wrong in their lives or with their pregnancies. If states insist on drawing lines based on historical measures of viability, at 24 or 26 or 28 weeks, they should stick with those gestational limits and admit that they no longer represent actual viability but correspond instead to some form of common morality about when the fetus has a protected, if not absolute, right to life. Women need a reasonable amount of time to make careful and informed decisions about whether to continue their pregnancies precisely because these decisions have a lasting impact on their bodies and their lives. To preserve that time, legislators and the courts should decouple abortion rights from ectogenesis and other advances in the care of extremely premature infants that move the point of viability ever earlier.
[Editor's Note: This article was updated after publication to reflect Amy Coney Barrett's confirmation. To read other articles in this special magazine issue, visit the e-reader version.]
World’s First “Augmented Reality” Contact Lens Aims to Revolutionize Much More Than Medicine
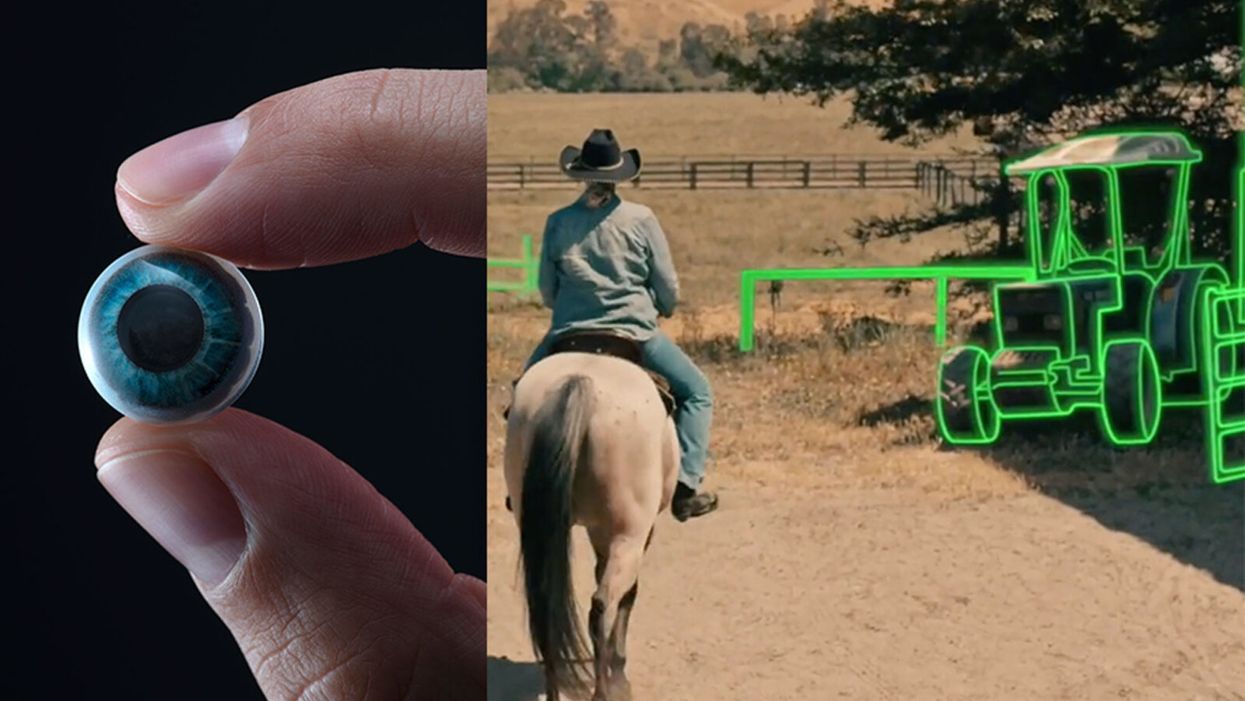
On the left, a picture of the Mojo lens smart contact; and a simulated image of a woman with low vision who is wearing the contact to highlight objects in her field of vision.
Imagine a world without screens. Instead of endlessly staring at your computer or craning your neck down to scroll through social media feeds and emails, information simply appears in front of your eyes when you need it and disappears when you don't.
"The vision is super clear...I was reading the poem with my eyes closed."
No more rude interruptions during dinner, no more bumping into people on the street while trying to follow GPS directions — just the information you want, when you need it, projected directly onto your visual field.
While this screenless future sounds like science fiction, it may soon be a reality thanks to the new Silicon Valley startup Mojo Vision, creator of the world's first smart contact lens. With a 14,000 pixel-per-inch display with eye-tracking, image stabilization, and a custom wireless radio, the Mojo smart lens bills itself the "smallest and densest dynamic display ever made." Unlike current augmented reality wearables such as Google Glass or ThirdEye, which project images onto a glass screen, the Mojo smart lens can project images directly onto the retina.
A current prototype displayed at the Consumer Electronics Show earlier this year in Las Vegas includes a tiny screen positioned right above the most sensitive area of the pupil. "[The Mojo lens] is a contact lens that essentially has wireless power and data transmission for a small micro LED projector that is placed over the center of the eye," explains David Hobbs, Director of Product Management at Mojo Vision. "[It] displays critical heads-up information when you need it and fades into the background when you're ready to continue on with your day."
Eventually, Mojo Visions' technology could replace our beloved smart devices but the first generation of the Mojo smart lens will be used to help the 2.2 billion people globally who suffer from vision impairment.
"If you think of the eye as a camera [for the visually impaired], the sensors are not working properly," explains Dr. Ashley Tuan, Vice President of Medical Devices at Mojo Vision and fellow of the American Academy of Optometry. "For this population, our lens can process the image so the contrast can be enhanced, we can make the image larger, magnify it so that low-vision people can see it or we can make it smaller so they can check their environment." In January of this year, the FDA granted Breakthrough Device Designation to Mojo, allowing them to have early and frequent discussions with the FDA about technical, safety and efficacy topics before clinical trials can be done and certification granted.
For now, Dr. Tuan is one of the few people who has actually worn the Mojo lens. "I put the contact lens on my eye. It was very comfortable like any contact lenses I've worn before," she describes. "The vision is super clear and then when I put on the accessories, suddenly I see Yoda in front of me and I see my vital signs. And then I have my colleague that prepared a beautiful poem that I loved when I was young [and] I was reading the poem with my eyes closed."
At the moment, there are several electronic glasses on the market like Acesight and Nueyes Pro that provide similar solutions for those suffering from visual impairment, but they are large, cumbersome, and highly visible. Mojo lens would be a discreet, more comfortable alternative that offers users more freedom of movement and independence.
"In the case of augmented-reality contact lenses, there could be an opportunity to improve the lives of people with low vision," says Dr. Thomas Steinemann, spokesperson for the American Academy of Ophthalmology and professor of ophthalmology at MetroHealth Medical Center in Cleveland. "There are existing tools for people currently living with low vision—such as digital apps, magnifiers, etc.— but something wearable could provide more flexibility and significantly more aid in day-to-day tasks."
As one of the first examples of "invisible computing," the potential applications of Mojo lens in the medical field are endless.
According to Dr. Tuan, the visually impaired often suffer from depression due to their lack of mobility and 70 percent of them are underemployed. "We hope that they can use this device to gain their mobility so they can get that social aspect back in their lives and then, eventually, employment," she explains. "That is our first and most important goal."
But helping those with low visual capabilities is only Mojo lens' first possible medical application; augmented reality is already being used in medicine and is poised to revolutionize the field in the coming decades. For example, Accuvein, a device that uses lasers to provide real-time images of veins, is widely used by nurses and doctors to help with the insertion of needles for IVs and blood tests.
According to the National Center for Biotechnology Information, augmentation of reality has been used in surgery for many years with surgeons using devices such as Google Glass to overlay critical information about their patients into their visual field. Using software like the Holographic Navigation Platform by Scopsis, surgeons can see a mixed-reality overlay that can "show you complicated tumor boundaries, assist with implant placements and guide you along anatomical pathways," its developers say.
However, according to Dr. Tuan, augmented reality headsets have drawbacks in the surgical setting. "The advantage of [Mojo lens] is you don't need to worry about sweating or that the headset or glasses will slide down to your nose," she explains "Also, our lens is designed so that it will understand your intent, so when you don't want the image overlay it will disappear, it will not block your visual field, and when you need it, it will come back at the right time."
As one of the first examples of "invisible computing," the potential applications of Mojo lens in the medical field are endless. Possibilities include live translation of sign language for deaf people; helping those with autism to read emotions; and improving doctors' bedside manner by allowing them to fully engage with patients without relying on a computer.
"[By] monitoring those blood vessels we can [track] chronic disease progression: high blood pressure, diabetes, and Alzheimer's."
Furthermore, the lens could be used to monitor health issues. "We have image sensors in the lens right now that point to the world but we can have a camera pointing inside of your eye to your retina," says Dr. Tuan, "[By] monitoring those blood vessels we can [track] chronic disease progression: high blood pressure, diabetes, and Alzheimer's."
For the moment, the future medical applications of the Mojo lens are still theoretical, but the team is confident they can eventually become a reality after going through the proper regulatory review. The company is still in the process of design, prototype and testing of the lens, so they don't know exactly when it will be available for use, but they anticipate shipping the first available products in the next couple of years. Once it does go to market, it will be available by prescription only for those with visual impairments, but the team's goal is to bring it to broader consumer markets pending regulatory clearance.
"We see that right now there's a unique opportunity here for Mojo lens and invisible computing to help to shape what the next decade of technology development looks like," explains David Hobbs. "We can use [the Mojo lens] to better serve us as opposed to us serving technology better."

Schmidt Ocean Institute co-founder Wendy Schmidt is backed by 32 screens in research vessel Falkor's control room where most of the science takes place on the ship, from mapping to live streaming of underwater robotic dives.
WENDY SCHMIDT is a philanthropist and investor who has spent more than a dozen years creating innovative non-profit organizations to solve pressing global environmental and human rights issues. Recognizing the human dependence on sustaining and protecting our planet and its people, Wendy has built organizations that work to educate and advance an understanding of the critical interconnectivity between the land and the sea. Through a combination of grants and investments, Wendy's philanthropic work supports research and science, community organizations, promising leaders, and the development of innovative technologies. Wendy is president of The Schmidt Family Foundation, which she co-founded with her husband Eric in 2006. They also co-founded Schmidt Ocean Institute and Schmidt Futures.
Editors: The pandemic has altered the course of human history and the nature of our daily lives in equal measure. How has it affected the focus of your philanthropy across your organizations? Have any aspects of the crisis in particular been especially galvanizing as you considered where to concentrate your efforts?
Wendy: The COVID-19 pandemic has made the work of our philanthropy more relevant than ever. If anything, the circumstances of this time have validated the focus we have had for nearly 15 years. We support the need for universal access to clean, renewable energy, healthy food systems, and the dignity of human labor and self-determination in a world of interconnected living systems on land and in the Ocean we are only beginning to understand.
When you consider the disproportionate impact of the COVID-19 virus on people who are poorly paid, poorly housed, with poor nutrition and health care, and exposed to unsafe conditions in the workplace—you see clearly how the systems that have been defining how we live, what we eat, who gets healthcare and what impacts the environment around us—need to change.
"This moment has propelled broad movements toward open publication and open sharing of data and samples—something that has always been a core belief in how we support and advance science."
If the pandemic teaches us anything, we learn what resilience looks like, and the essential role for local small businesses including restaurants, farms and ranches, dairies and fish markets in the long term vitality of communities. There is resonance, local economic benefit, and also accountability in these smaller systems, with shorter supply chains and less vertical integration.
The consolidation of vertically integrated business operations for the sake of global efficiency reveals its essential weakness when supply chains break down and the failure to encourage local economic centers leads to intense systemic disruption and the possibility of collapse.
Editors: For scientists, one significant challenge has been figuring out how to continue research, if at all, during this time of isolation and distancing. Yet, your research vessel Falkor, of the Schmidt Ocean Institute, is still on its expedition exploring the Coral Sea Marine Park in Australia—except now there are no scientists onboard. What was the vessel up to before the pandemic hit? Can you tell us more about how they are continuing to conduct research from afar now and how that's going?
Wendy: We have been extremely fortunate at Schmidt Ocean Institute. When the pandemic hit in March, our research vessel, Falkor, was already months into a year-long program to research unexplored deep sea canyons around Australia and at the Great Barrier Reef. We were at sea, with an Australian science group aboard, carrying on with our mission of exploration, discovery and communication, when we happened upon what we believe to be the world's longest animal—a siphonophore about 150 feet long, spiraling out at a depth of about 2100 feet at the end of a deeper dive in the Ningaloo Canyon off Western Australia. It was the kind of wondrous creature we find so often when we conduct ROV dives in the world's Ocean.
For more than two months this year, Falkor was reportedly the only research vessel in the world carrying on active research at sea. Once we were able to dock and return the science party to shore, we resumed our program at sea offering a scheduled set of now land-based scientists in lockdown in Australia the opportunity to conduct research remotely, taking advantage of the vessel's ship to shore communications, high resolution cameras and live streaming video. It's a whole new world, and quite wonderful in its own way.
Editors: Normally, 10–15 scientists would be aboard such a vessel. Is "remote research" via advanced video technology here to stay? Are there any upsides to this "new normal"?
Wendy: Like all things pandemic, remote research is an adaptation for what would normally occur. Since we are putting safety of the crew and guest scientists at the forefront, we're working to build strong remote connections between our crew, land based scientists and the many robotic tools on board Falkor. There's no substitute for in person work, but what we've developed during the current cruise is a pretty good and productive alternative in a crisis. And what's important is that this critical scientific research into the deep sea is able to continue, despite the pandemic on land.
Editors: Speaking of marine expeditions, you've sponsored two XPRIZE competitions focused on ocean health. Do you think challenge prizes could fill gaps of the global COVID-19 response, for example, to manufacture more testing kits, accelerate the delivery of PPE, or incentivize other areas of need?
Wendy: One challenge we are currently facing is that innovations don't have the funding pathway to scale, so promising ideas by entrepreneurs, researchers, and even major companies are being developed too slowly. Challenge prizes help raise awareness for problems we are trying to solve and attract new people to help solve those problems by giving them a pathway to contribute.
One idea might be for philanthropy to pair prizes and challenges with an "advanced market commitment" where the government commits to a purchase order for the innovation if it meets a certain test. That could be deeply impactful for areas like PPE and the production of testing kits.
Editors: COVID-19 testing, especially, has been sorely needed, here in the U.S. and in developing countries as well as low-income communities. That's why we're so intrigued by your Schmidt Science Fellows grantee Hal Holmes and his work to repurpose a new DNA technology to create a portable, mobile test for COVID-19. Can you tell us about that work and how you are supporting it?
Wendy: Our work with Conservation X Labs began years ago when our foundation was the first to support their efforts to develop a handheld DNA barcode sensor to help detect illegally imported and mislabeled seafood and timber products. The device was developed by Hal Holmes, who became one of our Schmidt Science Fellows and is the technical lead on the project, working closely with Conservation X Labs co-founders Alex Deghan and Paul Bunje. Now, with COVID-19, Hal and team have worked with another Schmidt Science Fellow, Fahim Farzardfard, to repurpose the technology—which requires no continuous power source, special training, or a lab—to serve as a mobile testing device for the virus.
The work is going very well, manufacturing is being organized, and distribution agreements with hospitals and government agencies are underway. You could see this device in use within a few months and have testing results within hours instead of days. It could be especially useful in low-income communities and developing countries where access to testing is challenging.
Editors: How is Schmidt Futures involved in the development of information platforms that will offer productive solutions?
Wendy: In addition to the work I've mentioned, we've also funded the development of tech-enabled tools that can help the medical community be better prepared for the ongoing spike of COVID cases. For example, we funded EdX and Learning Agency to develop an online training to help increase the number of medical professionals who can operate ventilators. The first course is being offered by Harvard University, and so far, over 220,000 medical professionals have enrolled. We have also invested in informational platforms that make it easier to contain the spread of the disease, such as our work with Recidiviz to model the impact of COVID-19 in prisons and outline policy steps states could take to limit the spread.
Information platforms can also play a big part pushing forward scientific research into the virus. For example, we've funded the UC Santa Cruz Virus Browser, which allows researchers to examine each piece of the virus and see the proteins it creates, the interactions in the host cell, and — most importantly — almost everything the recent scientific literature has to say about that stretch of the molecule.
Editors: The scale of research collaboration and the speed of innovation today seem unprecedented. The whole science world has turned its attention to combating the pandemic. What positive big-picture trends do you think or hope will persist once the crisis eventually abates?
Wendy: As in many areas, the COVID crisis has accelerated trends in the scientific world that were already well underway. For instance, this moment has propelled broad movements toward open publication and open sharing of data and samples—something that has always been a core belief in how we support and advance science.
We believe collaboration is an essential ingredient for progress in all areas. Early in this pandemic, Schmidt Futures held a virtual gathering of 160 people across 70 organizations in philanthropy, government, and business interested in accelerating research and response to the virus, and thought at the time, it's pretty amazing this kind of thing doesn't go all the time. We are obviously going to go farther together than on our own...
My husband, Eric, has observed that in the past two months, we've all catapulted 10 years forward in our use of technology, so there are trends already underway that are likely accelerated and will become part of the fabric of the post-COVID world—like working remotely; online learning; increased online shopping, even for groceries; telemedicine; increasing use of AI to create smarter delivery systems for healthcare and many other applications in a world that has grown more virtual overnight.
"Our deepest hope is that out of these alarming and uncertain times will come a renewed appreciation for the tools of science, as they help humans to navigate a world of interconnected living systems, of which viruses are a large part."
We fully expect these trends to continue and expand across the sciences, sped up by the pressures of the health crisis. Schmidt Ocean Institute and Schmidt Futures have been pressing in these directions for years, so we are pleased to see the expansions that should help more scientists work productively, together.
Editors: Trying to find the good amid a horrible crisis, are there any other new horizons in science, philanthropy, and/or your own work that could transform our world for the better that you'd like to share?
Wendy: Our deepest hope is that out of these alarming and uncertain times will come a renewed appreciation for the tools of science, as they help humans to navigate a world of interconnected living systems, of which viruses are a large part. The more we investigate the Ocean, the more we look deeply into what lies in our soils and beneath them, the more we realize we do not know, and moreover, how vulnerable humanity is to the forces of the natural world.
Philanthropy has an important role to play in influencing how people perceive our place in the world and understand the impact of human activity on the rest of the planet. I believe it's philanthropy's role to take risks, to invest early in innovative technologies, to lead where governments and industry aren't ready to go yet. We're fortunate at this time to be able to help those working on tools to better diagnose and treat the virus, and to invest in those working to improve information systems, so citizens and policy makers can make better decisions that can reduce impacts on families and institutions.
From all we know, this isn't likely to be the last pandemic the world will see. It's been said that a crisis comes before change, and we would hope that we can play a role in furthering the work to build systems that are resilient—in information, energy, agriculture and in all the ways we work, recreate, and use the precious resources of our planet.
[This article was originally published on June 8th, 2020 as part of a standalone magazine called GOOD10: The Pandemic Issue. Produced as a partnership among LeapsMag, The Aspen Institute, and GOOD, the magazine is available for free online.]
Kira Peikoff was the editor-in-chief of Leaps.org from 2017 to 2021. As a journalist, her work has appeared in The New York Times, Newsweek, Nautilus, Popular Mechanics, The New York Academy of Sciences, and other outlets. She is also the author of four suspense novels that explore controversial issues arising from scientific innovation: Living Proof, No Time to Die, Die Again Tomorrow, and Mother Knows Best. Peikoff holds a B.A. in Journalism from New York University and an M.S. in Bioethics from Columbia University. She lives in New Jersey with her husband and two young sons. Follow her on Twitter @KiraPeikoff.