
Abortions Before Fetal Viability Are Legal: Might Science and the Change on the Supreme Court Undermine That?

The United States Supreme Court Building in Washington, D.C.
This article is part of the magazine, "The Future of Science In America: The Election Issue," co-published by LeapsMag, the Aspen Institute Science & Society Program, and GOOD.
Viability—the potential for a fetus to survive outside the womb—is a core dividing line in American law. For almost 50 years, the Supreme Court of the United States has struck down laws that ban all or most abortions, ruling that women's constitutional rights include choosing to end pregnancies before the point of viability. Once viability is reached, however, states have a "compelling interest" in protecting fetal life. At that point, states can choose to ban or significantly restrict later-term abortions provided states allow an exception to preserve the life or health of the mother.
This distinction between a fetus that could survive outside its mother's body, albeit with significant medical intervention, and one that could not, is at the heart of the court's landmark 1973 decision in Roe v. Wade. The framework of viability remains central to the country's abortion law today, even as some states have passed laws in the name of protecting women's health that significantly undermine Roe. Over the last 30 years, the Supreme Court has upheld these laws, which have the effect of restricting pre-viability abortion access, imposing mandatory waiting periods, requiring parental consent for minors, and placing restrictions on abortion providers.
Viability has always been a slippery notion on which to pin legal rights.
Today, the Guttmacher Institute reports that more than half of American women live in states whose laws are considered hostile to abortion, largely as a result of these intrusions on pre-viability abortion access. Nevertheless, the viability framework stands: while states can pass pre-viability abortion restrictions that (ostensibly) protect the health of the woman or that strike some kind a balance between women's rights and fetal life, it is only after viability that they can completely favor fetal life over the rights of the woman (with limited exceptions when the woman's life is threatened). As a result, judges have struck down certain states' so-called heartbeat laws, which tried to prohibit abortions after detection of a fetal heartbeat (as early as six weeks of pregnancy). Bans on abortion after 12 or 15 weeks' gestation have also been reversed.
Now, with a new Supreme Court Justice expected to be hostile to abortion rights, advances in the care of preterm babies and ongoing research on artificial wombs suggest that the point of viability is already sooner than many assume and could soon be moved radically earlier in gestation, potentially providing a legal basis for earlier and earlier abortion bans.
Viability has always been a slippery notion on which to pin legal rights. It represents an inherently variable and medically shifting moment in the pregnancy timeline that the Roe majority opinion declined to firmly define, noting instead that "[v]iability is usually placed at about seven months (28 weeks) but may occur earlier, even at 24 weeks." Even in 1977, this definition was an optimistic generalization. Every baby is different, and while some 28-week infants born the year Roe was decided did indeed live into adulthood, most died at or shortly after birth. The prognosis for infants born at 24 weeks was much worse.
Today, a baby born at 28 weeks' gestation can be expected to do much better, largely due to the development of surfactant treatment in the early 1990s to help ease the air into babies' lungs. Now, the majority of 24-week-old babies can survive, and several very premature babies, born just shy of 22 weeks' gestation, have lived into childhood. All this variability raises the question: Should the law take a very optimistic, if largely unrealistic, approach to defining viability and place it at 22 weeks, even though the overall survival rate for those preemies remains less than 10% today? Or should the law recognize that keeping a premature infant alive requires specialist care, meaning that actual viability differs not just pregnancy-to-pregnancy but also by healthcare facility and from country to country? A 24-week premature infant born in a rural area or in a developing nation may not be viable as a practical matter, while one born in a major U.S. city with access to state-of-the-art care has a greater than 70% chance of survival. Just as some extremely premature newborns survive, some full-term babies die before, during, or soon after birth, regardless of whether they have access to advanced medical care.
To be accurate, viability should be understood as pregnancy-specific and should take into account the healthcare resources available to that woman. But state laws can't capture this degree of variability by including gestation limits in their abortion laws. Instead, many draw a somewhat arbitrary line at 22, 24, or 28 weeks' gestation, regardless of the particulars of the pregnancy or the medical resources available in that state.
As variable and resource-dependent as viability is today, science may soon move that point even earlier. Ectogenesis is a term coined in 1923 for the growth of an organism outside the body. Long considered science fiction, this technology has made several key advances in the past few years, with scientists announcing in 2017 that they had successfully gestated premature lamb fetuses in an artificial womb for four weeks. Currently in development for use in human fetuses between 22 and 23 weeks' gestation, this technology will almost certainly seek to push viability earlier in pregnancy.
Ectogenesis and other improvements in managing preterm birth deserve to be celebrated, offering new hope to the parents of very premature infants. But in the U.S., and in other nations whose abortion laws are fixed to viability, these same advances also pose a threat to abortion access. Abortion opponents have long sought to move the cutoff for legal abortions, and it is not hard to imagine a state prohibiting all abortions after 18 or 20 weeks by arguing that medical advances render this stage "the new viability," regardless of whether that level of advanced care is available to women in that state. If ectogenesis advances further, the limit could be moved to keep pace.
The Centers for Disease Control and Prevention reports that over 90% of abortions in America are performed at or before 13 weeks, meaning that in the short term, only a small number women would be affected by shifting viability standards. Yet these women are in difficult situations and deserve care and consideration. Research has shown that women seeking later terminations often did not recognize that they were pregnant or had their dates quite wrong, while others report that they had trouble accessing a termination earlier in pregnancy, were afraid to tell their partner or parents, or only recently received a diagnosis of health problems with the fetus.
Shifts in viability over the past few decades have already affected these women, many of whom report struggling to find a provider willing to perform a termination at 18 or 20 weeks out of concern that the woman may have her dates wrong. Ever-earlier gestational limits would continue this chilling effect, making doctors leery of terminating a pregnancy that might be within 2–4 weeks of each new ban. Some states' existing gestational limits on abortion are also inconsistent with prenatal care, which includes genetic testing between 12 and 20 weeks' gestation, as well as an anatomy scan to check the fetus's organ development performed at approximately 20 weeks. If viability moves earlier, prenatal care will be further undermined.
Perhaps most importantly, earlier and earlier abortion bans are inconsistent with the rights and freedoms on which abortion access is based, including recognition of each woman's individual right to bodily integrity and decision-making authority over her own medical care. Those rights and freedoms become meaningless if abortion bans encroach into the weeks that women need to recognize they are pregnant, assess their options, seek medical advice, and access appropriate care. Fetal viability, with its shifting goalposts, isn't the best framework for abortion protection in light of advancing medical science.
Ideally, whether to have an abortion would be a decision that women make in consultation with their doctors, free of state interference. The vast majority of women already make this decision early in pregnancy; the few who come to the decision later do so because something has gone seriously wrong in their lives or with their pregnancies. If states insist on drawing lines based on historical measures of viability, at 24 or 26 or 28 weeks, they should stick with those gestational limits and admit that they no longer represent actual viability but correspond instead to some form of common morality about when the fetus has a protected, if not absolute, right to life. Women need a reasonable amount of time to make careful and informed decisions about whether to continue their pregnancies precisely because these decisions have a lasting impact on their bodies and their lives. To preserve that time, legislators and the courts should decouple abortion rights from ectogenesis and other advances in the care of extremely premature infants that move the point of viability ever earlier.
[Editor's Note: This article was updated after publication to reflect Amy Coney Barrett's confirmation. To read other articles in this special magazine issue, visit the e-reader version.]
Coronavirus Risk Calculators: What You Need to Know
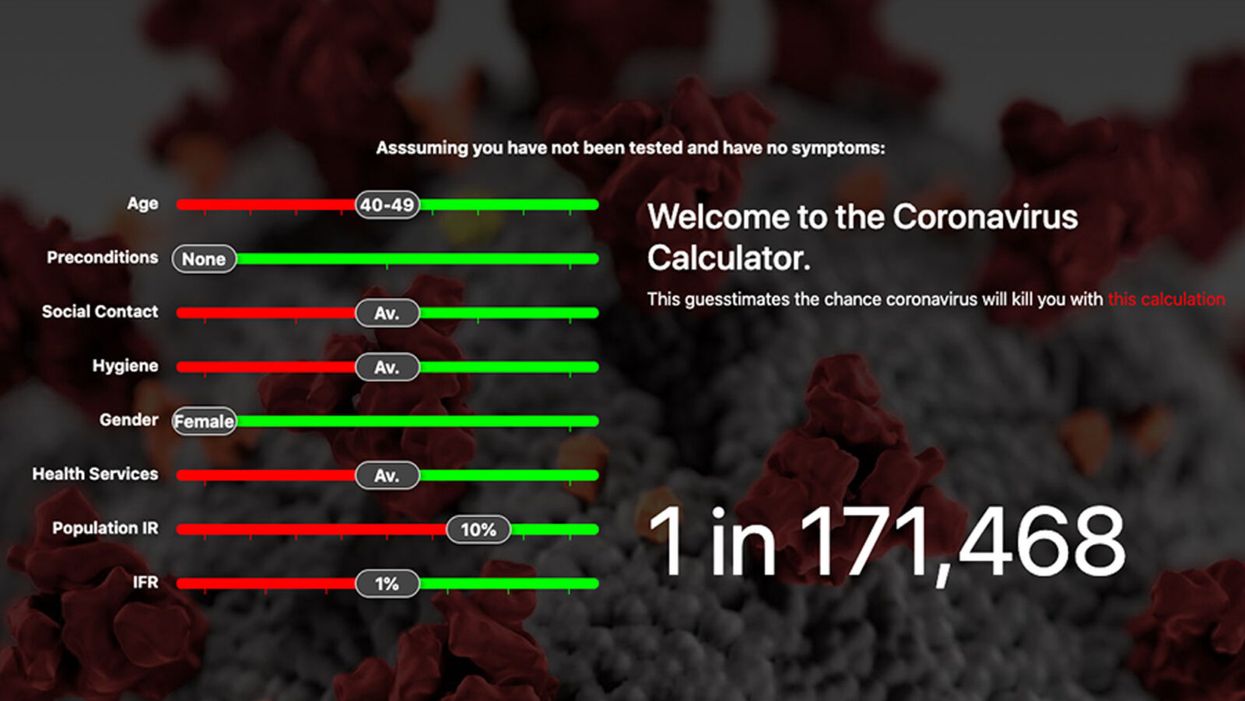
A screenshot of one coronavirus risk calculator.
People in my family seem to develop every ailment in the world, including feline distemper and Dutch elm disease, so I naturally put fingers to keyboard when I discovered that COVID-19 risk calculators now exist.
"It's best to look at your risk band. This will give you a more useful insight into your personal risk."
But the results – based on my answers to questions -- are bewildering.
A British risk calculator developed by the Nexoid software company declared I have a 5 percent, or 1 in 20, chance of developing COVID-19 and less than 1 percent risk of dying if I get it. Um, great, I think? Meanwhile, 19 and Me, a risk calculator created by data scientists, says my risk of infection is 0.01 percent per week, or 1 in 10,000, and it gave me a risk score of 44 out of 100.
Confused? Join the club. But it's actually possible to interpret numbers like these and put them to use. Here are five tips about using coronavirus risk calculators:
1. Make Sure the Calculator Is Designed For You
Not every COVID-19 risk calculator is designed to be used by the general public. Cleveland Clinic's risk calculator, for example, is only a tool for medical professionals, not sick people or the "worried well," said Dr. Lara Jehi, Cleveland Clinic's chief research information officer.
Unfortunately, the risk calculator's web page fails to explicitly identify its target audience. But there are hints that it's not for lay people such as its references to "platelets" and "chlorides."
The 19 and Me or the Nexoid risk calculators, in contrast, are both designed for use by everyone, as is a risk calculator developed by Emory University.
2. Take a Look at the Calculator's Privacy Policy
COVID-19 risk calculators ask for a lot of personal information. The Nexoid calculator, for example, wanted to know my age, weight, drug and alcohol history, pre-existing conditions, blood type and more. It even asked me about the prescription drugs I take.
It's wise to check the privacy policy and be cautious about providing an email address or other personal information. Nexoid's policy says it provides the information it gathers to researchers but it doesn't release IP addresses, which can reveal your location in certain circumstances.
John-Arne Skolbekken, a professor and risk specialist at Norwegian University of Science and Technology, entered his own data in the Nexoid calculator after being contacted by LeapsMag for comment. He noted that the calculator, among other things, asks for information about use of recreational drugs that could be illegal in some places. "I have given away some of my personal data to a company that I can hope will not misuse them," he said. "Let's hope they are trustworthy."
The 19 and Me calculator, by contrast, doesn't gather any data from users, said Cindy Hu, data scientist at Mathematica, which created it. "As soon as the window is closed, that data is gone and not captured."
The Emory University risk calculator, meanwhile, has a long privacy policy that states "the information we collect during your assessment will not be correlated with contact information if you provide it." However, it says personal information can be shared with third parties.
3. Keep an Eye on Time Horizons
Let's say a risk calculator says you have a 1 percent risk of infection. That's fairly low if we're talking about this year as a whole, but it's quite worrisome if the risk percentage refers to today and jumps by 1 percent each day going forward. That's why it's helpful to know exactly what the numbers mean in terms of time.
Unfortunately, this information isn't always readily available. You may have to dig around for it or contact a risk calculator's developers for more information. The 19 and Me calculator's risk percentages refer to this current week based on your behavior this week, Hu said. The Nexoid calculator, by contrast, has an "infinite timeline" that assumes no vaccine is developed, said Jonathon Grantham, the company's managing director. But your results will vary over time since the calculator's developers adjust it to reflect new data.
When you use a risk calculator, focus on this question: "How does your risk compare to the risk of an 'average' person?"
4. Focus on the Big Picture
The Nexoid calculator gave me numbers of 5 percent (getting COVID-19) and 99.309 percent (surviving it). It even provided betting odds for gambling types: The odds are in favor of me not getting infected (19-to-1) and not dying if I get infected (144-to-1).
However, Grantham told me that these numbers "are not the whole story." Instead, he said, "it's best to look at your risk band. This will give you a more useful insight into your personal risk." Risk bands refer to a segmentation of people into five categories, from lowest to highest risk, according to how a person's result sits relative to the whole dataset.
The Nexoid calculator says I'm in the "lowest risk band" for getting COVID-19, and a "high risk band" for dying of it if I get it. That suggests I'd better stay in the lowest-risk category because my pre-existing risk factors could spell trouble for my survival if I get infected.
Michael J. Pencina, a professor and biostatistician at Duke University School of Medicine, agreed that focusing on your general risk level is better than focusing on numbers. When you use a risk calculator, he said, focus on this question: "How does your risk compare to the risk of an 'average' person?"
The 19 and Me calculator, meanwhile, put my risk at 44 out of 100. Hu said that a score of 50 represents the typical person's risk of developing serious consequences from another disease – the flu.
5. Remember to Take Action
Hu, who helped develop the 19 and Me risk calculator, said it's best to use it to "understand the relative impact of different behaviors." As she noted, the calculator is designed to allow users to plug in different answers about their behavior and immediately see how their risk levels change.
This information can help us figure out if we should change the way we approach the world by, say, washing our hands more or avoiding more personal encounters.
"Estimation of risk is only one part of prevention," Pencina said. "The other is risk factors and our ability to reduce them." In other words, odds, percentages and risk bands can be revealing, but it's what we do to change them that matters.
Pseudoscience Is Rampant: How Not to Fall for It
A metaphorical rendering of scientific truth gone awry.
Whom to believe?
The relentless and often unpredictable coronavirus (SARS-CoV-2) has, among its many quirky terrors, dredged up once again the issue that will not die: science versus pseudoscience.
How does one learn to spot the con without getting a Ph.D. and spending years in a laboratory?
The scientists, experts who would be the first to admit they are not infallible, are now in danger of being drowned out by the growing chorus of pseudoscientists, conspiracy theorists, and just plain troublemakers that seem to be as symptomatic of the virus as fever and weakness.
How is the average citizen to filter this cacophony of information and misinformation posing as science alongside real science? While all that noise makes it difficult to separate the real stuff from the fakes, there is at least one positive aspect to it all.
A famous aphorism by one Charles Caleb Colton, a popular 19th-century English cleric and writer, says that "imitation is the sincerest form of flattery."
The frauds and the paranoid conspiracy mongers who would perpetrate false science on a susceptible public are at least recognizing the value of science—they imitate it. They imitate the ways in which science works and make claims as if they were scientists, because even they recognize the power of a scientific approach. They are inadvertently showing us how much we value science. Unfortunately they are just shabby counterfeits.
Separating real science from pseudoscience is not a new problem. Philosophers, politicians, scientists, and others have been worrying about this perhaps since science as we know it, a science based entirely on experiment and not opinion, arrived in the 1600s. The original charter of the British Royal Society, the first organized scientific society, stated that at their formal meetings there would be no discussion of politics, religion, or perpetual motion machines.
The first two of those for the obvious purpose of keeping the peace. But the third is interesting because at that time perpetual motion machines were one of the main offerings of the imitators, the bogus scientists who were sure that you could find ways around the universal laws of energy and make a buck on it. The motto adopted by the society was, and remains, Nullius in verba, Latin for "take nobody's word for it." Kind of an early version of Missouri's venerable state motto: "Show me."
You might think that telling phony science from the real thing wouldn't be so difficult, but events, historical and current, tell a very different story—often with tragic outcomes. Just one terrible example is the estimated 350,000 additional HIV deaths in South Africa directly caused by the now-infamous conspiracy theories of their own elected President no less (sound familiar?). It's surprisingly easy to dress up phony science as the real thing by simply adopting, or appearing to adopt, the trappings of science.
Thus, the anti-vaccine movement claims to be based on suspicion of authority, beginning with medical authority in this case, stemming from the fraudulent data published by the now-disgraced Andrew Wakefield, an English gastroenterologist. And it's true that much of science is based on suspicion of authority. Science got its start when the likes of Galileo and Copernicus claimed that the Church, the State, even Aristotle, could no longer be trusted as authoritative sources of knowledge.
But Galileo and those who followed him produced alternative explanations, and those alternatives were based on data that arose independently from many sources and generated a great deal of debate and, most importantly, could be tested by experiments that could prove them wrong. The anti-vaccine movement imitates science, still citing the discredited Wakefield report, but really offers nothing but suspicion—and that is paranoia, not science.
Similarly, there are those who try to cloak their nefarious motives in the trappings of science by claiming that they are taking the scientific posture of doubt. Science after all depends on doubt—every scientist doubts every finding they make. Every scientist knows that they can't possibly foresee all possible instances or situations in which they could be proven wrong, no matter how strong their data. Einstein was doubted for two decades, and cosmologists are still searching for experimental proofs of relativity. Science indeed progresses by doubt. In science revision is a victory.
But the imitators merely use doubt to suggest that science is not dependable and should not be used for informing policy or altering our behavior. They claim to be taking the legitimate scientific stance of doubt. Of course, they don't doubt everything, only what is problematic for their individual enterprises. They don't doubt the value of blood pressure medicine to control their hypertension. But they should, because every medicine has side effects and we don't completely understand how blood pressure is regulated and whether there may not be still better ways of controlling it.
But we use the pills we have because the science is sound even when it is not completely settled. Ask a hypertensive oil executive who would like you to believe that climate science should be ignored because there are too many uncertainties in the data, if he is willing to forgo his blood pressure medicine—because it, too, has its share of uncertainties and unwanted side effects.
The apparent success of pseudoscience is not due to gullibility on the part of the public. The problem is that science is recognized as valuable and that the imitators are unfortunately good at what they do. They take a scientific pose to gain your confidence and then distort the facts to their own purposes. How does one learn to spot the con without getting a Ph.D. and spending years in a laboratory?
"If someone claims to have the ultimate answer or that they know something for certain, the only thing for sure is that they are trying to fool you."
What can be done to make the distinction clearer? Several solutions have been tried—and seem to have failed. Radio and television shows about the latest scientific breakthroughs are a noble attempt to give the public a taste of good science, but they do nothing to help you distinguish between them and the pseudoscience being purveyed on the neighboring channel and its "scientific investigations" of haunted houses.
Similarly, attempts to inculcate what are called "scientific habits of mind" are of little practical help. These habits of mind are not so easy to adopt. They invariably require some amount of statistics and probability and much of that is counterintuitive—one of the great values of science is to help us to counter our normal biases and expectations by showing that the actual measurements may not bear them out.
Additionally, there is math—no matter how much you try to hide it, much of the language of science is math (Galileo said that). And half the audience is gone with each equation (Stephen Hawking said that). It's hard to imagine a successful program of making a non-scientifically trained public interested in adopting the rigors of scientific habits of mind. Indeed, I suspect there are some people, artists for example, who would be rightfully suspicious of changing their thinking to being habitually scientific. Many scientists are frustrated by the public's inability to think like a scientist, but in fact it is neither easy nor always desirable to do so. And it is certainly not practical.
There is a more intuitive and simpler way to tell the difference between the real thing and the cheap knock-off. In fact, it is not so much intuitive as it is counterintuitive, so it takes a little bit of mental work. But the good thing is it works almost all the time by following a simple, if as I say, counterintuitive, rule.
True science, you see, is mostly concerned with the unknown and the uncertain. If someone claims to have the ultimate answer or that they know something for certain, the only thing for sure is that they are trying to fool you. Mystery and uncertainty may not strike you right off as desirable or strong traits, but that is precisely where one finds the creative solutions that science has historically arrived at. Yes, science accumulates factual knowledge, but it is at its best when it generates new and better questions. Uncertainty is not a place of worry, but of opportunity. Progress lives at the border of the unknown.
How much would it take to alter the public perception of science to appreciate unknowns and uncertainties along with facts and conclusions? Less than you might think. In fact, we make decisions based on uncertainty every day—what to wear in case of 60 percent chance of rain—so it should not be so difficult to extend that to science, in spite of what you were taught in school about all the hard facts in those giant textbooks.
You can believe science that says there is clear evidence that takes us this far… and then we have to speculate a bit and it could go one of two or three ways—or maybe even some way we don't see yet. But like your blood pressure medicine, the stuff we know is reliable even if incomplete. It will lower your blood pressure, no matter that better treatments with fewer side effects may await us in the future.
Unsettled science is not unsound science. The honesty and humility of someone who is willing to tell you that they don't have all the answers, but they do have some thoughtful questions to pursue, are easy to distinguish from the charlatans who have ready answers or claim that nothing should be done until we are an impossible 100-percent sure.
Imitation may be the sincerest form of flattery.
The problem, as we all know, is that flattery will get you nowhere.
[Editor's Note: This article was originally published on June 8th, 2020 as part of a standalone magazine called GOOD10: The Pandemic Issue. Produced as a partnership among LeapsMag, The Aspen Institute, and GOOD, the magazine is available for free online.]