
As Our AI Systems Get Better, So Must We

In order to build the future we want, we must also become ever better humans, explains the futurist Jamie Metzl in this opinion essay.
As the power and capability of our AI systems increase by the day, the essential question we now face is what constitutes peak human. If we stay where we are while the AI systems we are unleashing continually get better, they will meet and then exceed our capabilities in an ever-growing number of domains. But while some technology visionaries like Elon Musk call for us to slow down the development of AI systems to buy time, this approach alone will simply not work in our hyper-competitive world, particularly when the potential benefits of AI are so great and our frameworks for global governance are so weak. In order to build the future we want, we must also become ever better humans.
The list of activities we once saw as uniquely human where AIs have now surpassed us is long and growing. First, AI systems could beat our best chess players, then our best Go players, then our best champions of multi-player poker. They can see patterns far better than we can, generate medical and other hypotheses most human specialists miss, predict and map out new cellular structures, and even generate beautiful, and, yes, creative, art.
A recent paper by Microsoft researchers analyzing the significant leap in capabilities in OpenAI’s latest AI bot, ChatGPT-4, asserted that the algorithm can “solve novel and difficult tasks that span mathematics, coding, vision, medicine, law, psychology and more, without needing any special prompting.” Calling this functionality “strikingly close to human-level performance,” the authors conclude it “could reasonably be viewed as an early (yet still incomplete) version of an artificial general intelligence (AGI) system.”
The concept of AGI has been around for decades. In its common use, the term suggests a time when individual machines can do many different things at a human level, not just one thing like playing Go or analyzing radiological images. Debating when AGI might arrive, a favorite pastime of computer scientists for years, now has become outdated.
We already have AI algorithms and chatbots that can do lots of different things. Based on the generalist definition, in other words, AGI is essentially already here.
Unfettered by the evolved capacity and storage constraints of our brains, AI algorithms can access nearly all of the digitized cultural inheritance of humanity since the dawn of recorded history and have increasing access to growing pools of digitized biological data from across the spectrum of life.
Once we recognize that both AI systems and humans have unique superpowers, the essential question becomes what each of us can do better than the other and what humans and AIs can best do in active collaboration. The future of our species will depend upon our ability to safely, dynamically, and continually figure that out.
With these ever-larger datasets, rapidly increasing computing and memory power, and new and better algorithms, our AI systems will keep getting better faster than most of us can today imagine. These capabilities have the potential to help us radically improve our healthcare, agriculture, and manufacturing, make our economies more productive and our development more sustainable, and do many important things better.
Soon, they will learn how to write their own code. Like human children, in other words, AI systems will grow up. But even that doesn’t mean our human goose is cooked.
Just like dolphins and dogs, these alternate forms of intelligence will be uniquely theirs, not a lesser or greater version of ours. There are lots of things AI systems can't do and will never be able to do because our AI algorithms, for better and for worse, will never be human. Our embodied human intelligence is its own thing.
Our human intelligence is uniquely ours based on the capacities we have developed in our 3.8-billion-year journey from single cell organisms to us. Our brains and bodies represent continuous adaptations on earlier models, which is why our skeletal systems look like those of lizards and our brains like most other mammals with some extra cerebral cortex mixed in. Human intelligence isn’t just some type of disembodied function but the inextricable manifestation of our evolved physical reality. It includes our sensory analytical skills and all of our animal instincts, intuitions, drives, and perceptions. Disembodied machine intelligence is something different than what we have evolved and possess.
Because of this, some linguists including Noam Chomsky have recently argued that AI systems will never be intelligent as long as they are just manipulating symbols and mathematical tokens without any inherent understanding. Nothing could be further from the truth. Anyone interacting with even first-generation AI chatbots quickly realizes that while these systems are far from perfect or omniscient and can sometimes be stupendously oblivious, they are surprisingly smart and versatile and will get more so… forever. We have little idea even how our own minds work, so judging AI systems based on their output is relatively close to how we evaluate ourselves.
Anyone not awed by the potential of these AI systems is missing the point. AI’s newfound capacities demand that we work urgently to establish norms, standards, and regulations at all levels from local to global to manage the very real risks. Pausing our development of AI systems now doesn’t make sense, however, even if it were possible, because we have no sufficient ways of uniformly enacting such a pause, no plan for how we would use the time, and no common framework for addressing global collective challenges like this.
But if all we feel is a passive awe for these new capabilities, we will also be missing the point.
Human evolution, biology, and cultural history are not just some kind of accidental legacy, disability, or parlor trick, but our inherent superpower. Our ancestors outcompeted rivals for billions of years to make us so well suited to the world we inhabit and helped build. Our social organization at scale has made it possible for us to forge civilizations of immense complexity, engineer biology and novel intelligence, and extend our reach to the stars. Our messy, embodied, intuitive, social human intelligence is roughly mimicable by AI systems but, by definition, never fully replicable by them.
Once we recognize that both AI systems and humans have unique superpowers, the essential question becomes what each of us can do better than the other and what humans and AIs can best do in active collaboration. We still don't know. The future of our species will depend upon our ability to safely, dynamically, and continually figure that out.
As we do, we'll learn that many of our ideas and actions are made up of parts, some of which will prove essentially human and some of which can be better achieved by AI systems. Those in every walk of work and life who most successfully identify the optimal contributions of humans, AIs, and the two together, and who build systems and workflows empowering humans to do human things, machines to do machine things, and humans and machines to work together in ways maximizing the respective strengths of each, will be the champions of the 21st century across all fields.
The dawn of the age of machine intelligence is upon us. It’s a quantum leap equivalent to the domestication of plants and animals, industrialization, electrification, and computing. Each of these revolutions forced us to rethink what it means to be human, how we live, and how we organize ourselves. The AI revolution will happen more suddenly than these earlier transformations but will follow the same general trajectory. Now is the time to aggressively prepare for what is fast heading our way, including by active public engagement, governance, and regulation.
AI systems will not replace us, but, like these earlier technology-driven revolutions, they will force us to become different humans as we co-evolve with our technology. We will never reach peak human in our ongoing evolutionary journey, but we’ve got to manage this transition wisely to build the type of future we’d like to inhabit.
Alongside our ascending AIs, we humans still have a lot of climbing to do.

Last month, a paper published in Cell by Harvard biologist David Sinclair explored root cause of aging, as well as examining whether this process can be controlled. We talked with Dr. Sinclair about this new research.
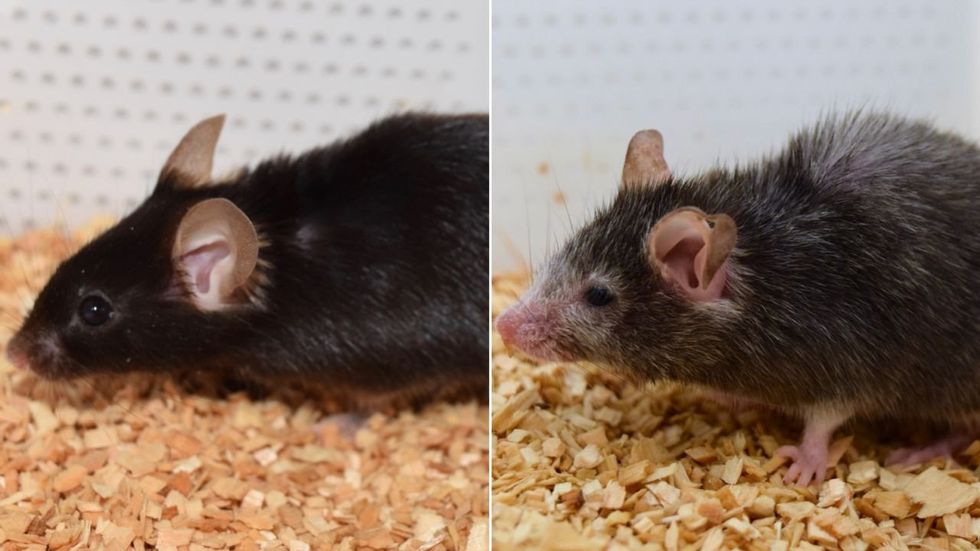
What causes aging? In a paper published last month, Dr. David Sinclair, Professor in the Department of Genetics at Harvard Medical School, reports that he and his co-authors have found the answer. Harnessing this knowledge, Dr. Sinclair was able to reverse this process, making mice younger, according to the study published in the journal Cell.
I talked with Dr. Sinclair about his new study for the latest episode of Making Sense of Science. Turning back the clock on mouse age through what’s called epigenetic reprogramming – and understanding why animals get older in the first place – are key steps toward finding therapies for healthier aging in humans. We also talked about questions that have been raised about the research.
Show links:
Dr. Sinclair's paper, published last month in Cell.
Recent pre-print paper - not yet peer reviewed - showing that mice treated with Yamanaka factors lived longer than the control group.
Dr. Sinclair's podcast.
Previous research on aging and DNA mutations.
Dr. Sinclair's book, Lifespan.

Harvard Medical School
Breakthrough therapies are breaking patients' banks. Key changes could improve access, experts say.

Single-treatment therapies are revolutionizing medicine. But insurers and patients wonder whether they can afford treatment and, if they can, whether the high costs are worthwhile.
CSL Behring’s new gene therapy for hemophilia, Hemgenix, costs $3.5 million for one treatment, but helps the body create substances that allow blood to clot. It appears to be a cure, eliminating the need for other treatments for many years at least.
Likewise, Novartis’s Kymriah mobilizes the body’s immune system to fight B-cell lymphoma, but at a cost $475,000. For patients who respond, it seems to offer years of life without the cancer progressing.
These single-treatment therapies are at the forefront of a new, bold era of medicine. Unfortunately, they also come with new, bold prices that leave insurers and patients wondering whether they can afford treatment and, if they can, whether the high costs are worthwhile.
“Most pharmaceutical leaders are there to improve and save people’s lives,” says Jeremy Levin, chairman and CEO of Ovid Therapeutics, and immediate past chairman of the Biotechnology Innovation Organization. If the therapeutics they develop are too expensive for payers to authorize, patients aren’t helped.
“The right to receive care and the right of pharmaceuticals developers to profit should never be at odds,” Levin stresses. And yet, sometimes they are.
Leigh Turner, executive director of the bioethics program, University of California, Irvine, notes this same tension between drug developers that are “seeking to maximize profits by charging as much as the market will bear for cell and gene therapy products and other medical interventions, and payers trying to control costs while also attempting to provide access to medical products with promising safety and efficacy profiles.”
Why Payers Balk
Health insurers can become skittish around extremely high prices, yet these therapies often accompany significant overall savings. For perspective, the estimated annual treatment cost for hemophilia exceeds $300,000. With Hemgenix, payers would break even after about 12 years.
But, in 12 years, will the patient still have that insurer? Therein lies the rub. U.S. payers, are used to a “pay-as-you-go” model, in which the lifetime costs of therapies typically are shared by multiple payers over many years, as patients change jobs. Single treatment therapeutics eliminate that cost-sharing ability.
"As long as formularies are based on profits to middlemen…Americans’ healthcare costs will continue to skyrocket,” says Patricia Goldsmith, the CEO of CancerCare.
“There is a phenomenally complex, bureaucratic reimbursement system that has grown, layer upon layer, during several decades,” Levin says. As medicine has innovated, payment systems haven’t kept up.
Therefore, biopharma companies begin working with insurance companies and their pharmacy benefit managers (PBMs), which act on an insurer’s behalf to decide which drugs to cover and by how much, early in the drug approval process. Their goal is to make sophisticated new drugs available while still earning a return on their investment.
New Payment Models
Pay-for-performance is one increasingly popular strategy, Turner says. “These models typically link payments to evidence generation and clinically significant outcomes.”
A biotech company called bluebird bio, for example, offers value-based pricing for Zynteglo, a $2.8 million possible cure for the rare blood disorder known as beta thalassaemia. It generally eliminates patients’ need for blood transfusions. The company is so sure it works that it will refund 80 percent of the cost of the therapy if patients need blood transfusions related to that condition within five years of being treated with Zynteglo.
In his February 2023 State of the Union speech, President Biden proposed three pilot programs to reduce drug costs. One of them, the Cell and Gene Therapy Access Model calls on the federal Centers for Medicare & Medicaid Services to establish outcomes-based agreements with manufacturers for certain cell and gene therapies.
A mortgage-style payment system is another, albeit rare, approach. Amortized payments spread the cost of treatments over decades, and let people change employers without losing their healthcare benefits.
Only about 14 percent of all drugs that enter clinical trials are approved by the FDA. Pharma companies, therefore, have an exigent need to earn a profit.
The new payment models that are being discussed aren’t solutions to high prices, says Bill Kramer, senior advisor for health policy at Purchaser Business Group on Health (PBGH), a nonprofit that seeks to lower health care costs. He points out that innovative pricing models, although well-intended, may distract from the real problem of high prices. They are attempts to “soften the blow. The best thing would be to charge a reasonable price to begin with,” he says.
Instead, he proposes making better use of research on cost and clinical effectiveness. The Institute for Clinical and Economic Review (ICER) conducts such research in the U.S., determining whether the benefits of specific drugs justify their proposed prices. ICER is an independent non-profit research institute. Its reports typically assess the degrees of improvement new therapies offer and suggest prices that would reflect that. “Publicizing that data is very important,” Kramer says. “Their results aren’t used to the extent they could and should be.” Pharmaceutical companies tend to price their therapies higher than ICER’s recommendations.
Drug Development Costs Soar
Drug developers have long pointed to the onerous costs of drug development as a reason for high prices.
A 2020 study found the average cost to bring a drug to market exceeded $1.1 billion, while other studies have estimated overall costs as high as $2.6 billion. The development timeframe is about 10 years. That’s because modern therapeutics target precise mechanisms to create better outcomes, but also have high failure rates. Only about 14 percent of all drugs that enter clinical trials are approved by the FDA. Pharma companies, therefore, have an exigent need to earn a profit.
Skewed Incentives Increase Costs
Pricing isn’t solely at the discretion of pharma companies, though. “What patients end up paying has much more to do with their PBMs than the actual price of the drug,” Patricia Goldsmith, CEO, CancerCare, says. Transparency is vital.
PBMs control patients’ access to therapies at three levels, through price negotiations, pricing tiers and pharmacy management.
When negotiating with drug manufacturers, Goldsmith says, “PBMs exchange a preferred spot on a formulary (the insurer’s or healthcare provider’s list of acceptable drugs) for cash-base rebates.” Unfortunately, 25 percent of the time, those rebates are not passed to insurers, according to the PBGH report.
Then, PBMs use pricing tiers to steer patients and physicians to certain drugs. For example, Kramer says, “Sometimes PBMs put a high-cost brand name drug in a preferred tier and a lower-cost competitor in a less preferred, higher-cost tier.” As the PBGH report elaborates, “(PBMs) are incentivized to include the highest-priced drugs…since both manufacturing rebates, as well as the administrative fees they charge…are calculated as a percentage of the drug’s price.
Finally, by steering patients to certain pharmacies, PBMs coordinate patients’ access to treatments, control patients’ out-of-pocket costs and receive management fees from the pharmacies.
Therefore, Goldsmith says, “As long as formularies are based on profits to middlemen…Americans’ healthcare costs will continue to skyrocket.”
Transparency into drug pricing will help curb costs, as will new payment strategies. What will make the most impact, however, may well be the development of a new reimbursement system designed to handle dramatic, breakthrough drugs. As Kramer says, “We need a better system to identify drugs that offer dramatic improvements in clinical care.”