
February 19 | 2020
Americans Fell for a Theranos-Style Scam 100 Years Ago. Will We Ever Learn?
Randy Dotinga is former president of the American Society of Journalists and Authors, a non-profit association of freelance writers and non-fiction authors. He has been a freelance writer since 1999 and specializes in health/medicine, politics, books, and the odd and unusual. You can follow him at @rdotinga.

Medical scams like Theranos are as American as America itself.
(© Syda Productions/Adobe, left, and on right, photo credit: Drew Kelly, Courtesy of HBO)
The huckster understands what people want – an easy route to good health -- and figures out just how to provide it as long as no one asks too many questions.
"Americans are very much prone to this sort of thinking: Give me a pill or give me a magical bean that can make me lose weight!"
The keys to success: Hoopla, fancy technology, and gullibility. And oh yes, one more thing: a blood sample. Well, lots and lots of blood samples. Every testing fee counts.
Sound familiar? It could be the story of the preternaturally persuasive Elizabeth Holmes, the disgraced founder of Theranos who stands accused of perpetrating a massive blood-testing fraud. But this is a different story from a different time, one that dates back 100 years but sounds almost like it could unfold on the front page of The Wall Street Journal today.
The main difference: Back then, watchdogs thought they'd be able to vanquish fake medicine and scam science. Fat chance, it turned out. It seems like we're more likely to lose-weight-quick than make much of a dent into quackery and health fraud.
Why? Have we learned anything at all over the past century? As we sweep into a new decade, experts says we're not as advanced as we'd like to think. But the fight against fraud and fakery continues.
Quackery: As American As America Itself
In the 17th century, British healers of questionable reputation got a new name -- "quack," from the Dutch word "quacksalver," which originally referred to someone who treats others with home remedies but developed a new meaning along the lines of "charlatan." And these quacks got a new place to sell their wares: the American colonies.
By 1692, a Boston newspaper advertised a patent medicine that promised to cure "the Griping of the Guts, and the Wind Cholick" and – for good measure – "preventeth that woeful Distemper of the Dry Belly Ach." A couple centuries later, the most famous woman in the United States wasn't a first lady or feminist but a hawker of nostrums named Lydia Estes Pinkham whose "vegetable compound" promised to banish "female complaints." One advertisement suggested that the "sure cure" would have saved the life of a Connecticut clergyman whose wife killed him after suffering from feminine maladies for 16 years.
By the early 20th century, Americans were fascinated by electricity and radiation, and both healers and hucksters embraced the new high-tech era. Men with flagging libidos, for example, could irradiate their private parts with the radioactive Radiendocrinator or buy battery-powered electric belts equipped with dangling bits to supercharge their, um, dangling bits.
The Rise of the Radio Wave 'Cure'
Enter radionics, the (supposed) science of better health via radio waves. The idea was that "healthy people radiate healthy energy," and sickness could be reversed through diagnosis and re-tuning, write Dr. Lydia Kang and Nate Pedersen in their 2017 book "Quackery: A Brief History of the Worst Ways to Cure Everything."
Detecting illness and fixing it required machinery -- Dynamizers, Radioclasts and Oscillocasts – that could cost hundreds of dollars each. Thousands of physicians bought them. Fortunately, they could work remotely, for a fee. The worried-and-potentially-unwell just needed to send a blood sample and, of course, a personal check.
Sting operations revealed radionics to be bogus. A skeptic sent a blood sample to one radionics practitioner in Albuquerque who reported back with news of an infected fallopian tube. In fact, the blood sample came from a male guinea pig. As an American Medical Association leader reported, the guinea pig "had shown no female characteristics up to that time, and a postmortem examination yielded no evidence of ladylike attributes."
When Quackery Refused to Yield
The rise of bogus medical technology in the early 20th century spawned a watchdog industry as organizations like the American Medical Association swept into action, said medical historian Eric Boyle, author of 2012's "Quack Medicine: A History of Combating Health Fraud in Twentieth-Century America."
"When quackery was recognized as a major problem, the people who campaigned for its demise were confident that they could get rid of it," he said. "A lot of people believed that increased education, the truths of science, and laws designed to protect consumers would ultimately drive quackery from the marketplace. And then throughout the century, as modern medicine developed, and more effectively treated one disease after another, many observers remained confident in that prediction."
There's a bid to "flood the information highway with truth to turn the storm of fake promotional stuff into a trickle."
But fake medicine persisted as Americans continued their quest to get- healthy-quick… or get-rich-quick by promising to help others to get- healthy-quick. Even radionics refused to die. It's still around in various forms. And, as the Theranos scandal reveals, we're still hoping our blood can offer the keys to longevity and good health.
Why Do We Still Fall for Scams?
In our own era, the Theranos company rose to prominence when founder and CEO Elizabeth Holmes convinced journalists and investors that she'd found a way to cheaply test drops of blood for hundreds of conditions. Then it all fell apart, famously, when the world learned that the technology didn't work. The company has folded, and Holmes faces a federal trial on fraud charges this year.
"There were a lot of prominent, very smart people who bought into the myth of Elizabeth Holmes," a former employee told "60 Minutes," even though the blood tests never actually worked as advertised.
Shouldn't "prominent, very smart people" know better? "People are gullible," said Dr. Stephen Barrett, a psychiatrist and leading quack-buster who runs the QuackWatch website. But there's more to the story. According to him, we're uniquely vulnerable as individuals to bogus medicine.
Scam artists specifically pinpoint their target audiences, such as "smart people," desperate people and alienated people, he said.
Smart people, for example, might be overconfident about their ability to detect fraud and fall for bogus medicine. Alienated people may distrust the establishment, whether it's the medical field or government watchdogs, and be more receptive to alternative sources of information.
Dr. Barrett also points a finger at magical thinking, which comes in different forms. It could mean a New Age-style belief that our minds can control the world around us. Or, as professional quack-buster Alex Berezow said, it could refer to "our cultural obsession with quick fixes."
"Americans are very much prone to this sort of thinking: Give me a pill or give me a magical bean that can make me lose weight! But complex problems need complex solutions," said Berezow, a microbiologist who debunks junk science in his job as a spokesman for the American Council on Science & Health.
American mistrust of expertise makes matters worse, he said. "When I tell people they need to get vaccinated, I'm called a shill for the pharmaceutical industry," he said. "If I say dietary supplements generally don't work, I'm a shill for doctors who want to keep people sick."
What can ordinary citizens do to protect themselves from fake medicine? "You have to have a healthy skepticism of everything," Berezow said. "When you come across something new, is someone trying to take advantage of you? It's a horrible way to think about the world, but there's some truth to it."
"Like any chronic disease, we will have to live with it while we do our best to fight it."
The government and experts have their own roles to play via regulation and education, respectively. For all the criticism it gets, the Food & Drug Administration does serve as a bulwark against fakery in prescription medicine. And while celebrities like Gwyneth "Goop" Paltrow hawk countless questionable medical products on the Internet, scientists and physicians are fighting back by using social media as a tool to promote the truth. There's a bid to "flood the information highway with truth to turn the storm of fake promotional stuff into a trickle," said Dr. Randi Hutter Epstein, a writer in residence at Yale School of Medicine and author of 2018's "Aroused: The History of Hormones and How They Control Just About Everything."
What's next? Like death, taxes and Cher, charlatans are likely to always be with us. Boyle quoted the late William Jarvis, a pioneering quack-buster in the late 20th century who believed health fraud would never be eradicated: "Like any chronic disease, we will have to live with it while we do our best to fight it."
Randy Dotinga is former president of the American Society of Journalists and Authors, a non-profit association of freelance writers and non-fiction authors. He has been a freelance writer since 1999 and specializes in health/medicine, politics, books, and the odd and unusual. You can follow him at @rdotinga.
December 23 | 2019
A New Test Aims to Objectively Measure Pain. It Could Help Legitimate Sufferers Access the Meds They Need.
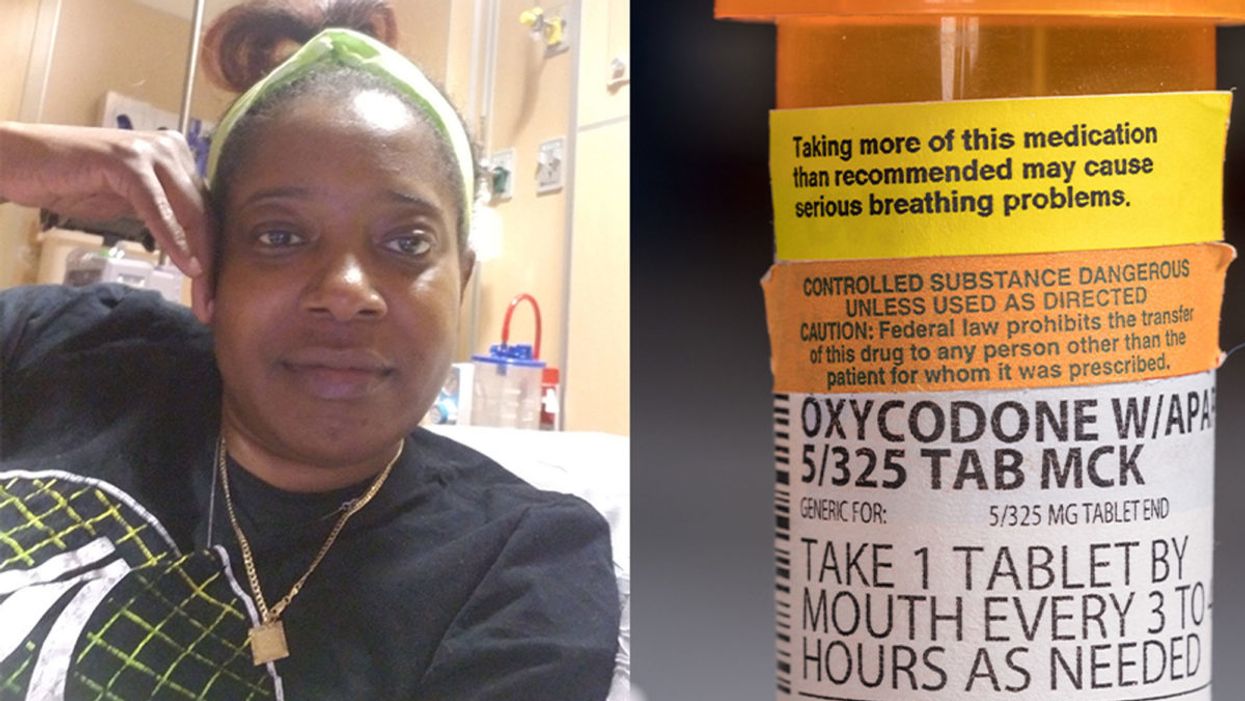
Sickle cell patient Bridgett Willkie found herself being labeled an addict when she sought an opioid prescription to control her pain.
(Left photo, courtesy of Willkie; on right, photo © by steheap/Adobe)
"That throbbing you feel for the first minute after a door slams on your finger."
This is how Central Florida resident Bridgett Willkie describes the attacks of pain caused by her sickle cell anemia – a genetic blood disorder in which a patient's red blood cells become shaped like sickles and get stuck in blood vessels, thereby obstructing the flow of blood and oxygen.
"I found myself being labeled as an addict and I never was."
Willkie's lifelong battle with the condition has led to avascular necrosis in both of her shoulders, hips, knees and ankles. This means that her bone tissue is dying due to insufficient blood supply (sickle cell anemia is among the medical conditions that can decrease blood flow to one's bones).
"That adds to the pain significantly," she says. "Every time my heart beats, it hurts. And the pain moves. It follows the path of circulation. I liken it to a traffic jam in my veins."
For more than a decade, she received prescriptions for Oxycontin. Then, four years ago, her hematologist – who had been her doctor for 18 years – suffered a fatal heart attack. She says her longtime doctor's replacement lacked experience treating sickle cell patients and was uncomfortable writing her a prescription for opioids. What's more, this new doctor wanted to place her in a drug rehab facility.
"Because I refused to go, he stopped writing my scripts," she says. The ensuing three months were spent at home, detoxing. She describes the pain as unbearable. "Sometimes I just wanted to die."
One of the effects of the opioid epidemic is that many legitimate pain patients have seen their opioids significantly reduced or downright discontinued because of their doctors' fears of over-prescribing addictive medications.
"I found myself being labeled as an addict and I never was...Being treated like a drug-seeking patient is degrading and humiliating," says Willkie, who adds that when she is at the hospital, "it's exhausting arguing with the doctors...You dread them making their rounds because every day they come in talking about weaning you off your meds."
Situations such as these are fraught with tension between patients and doctors, who must remain wary about the risk of over-prescribing powerful and addictive medications. Adding to the complexity is that it can be very difficult to reliably assess a patient's level of physical pain.
However, this difficulty may soon decline, as Indiana University School of Medicine researchers, led by Dr. Alexander B. Niculescu, have reportedly devised a way to objectively assess physical pain by analyzing biomarkers in a patient's blood sample. The results of a study involving more than 300 participants were published earlier this year in the journal Molecular Psychiatry.
Niculescu – who is both a professor of psychiatry and medical neuroscience at the IU School of Medicine – explains that, when someone is in severe physical pain, a blood sample will show biomarkers related to intracellular adhesion and cell-signaling mechanisms. He adds that some of these biomarkers "have prior convergent evidence from animal or human studies for involvement in pain."
Aside from reliably measuring pain severity, Niculescu says blood biomarkers can measure the degree of one's response to treatment and also assess the risk of future recurrences of pain. He believes this new method's greatest benefit, however, might be the ability to identify a number of non-opioid medications that a particular patient is likely to respond to, based on his or her biomarker profile.
Clearly, such a method could be a gamechanger for pain patients and the professionals who treat them. As of yet, health workers have been forced to make crucial decisions based on their clinical impressions of patients; such impressions are invariably subjective. A method that enables people to prove the extent of their pain could remove the stigma that many legitimate pain patients face when seeking to obtain their needed medicine. It would also improve their chances of receiving sufficient treatment.
Niculescu says it's "theoretically possible" that there are some conditions which, despite being severe, might not reveal themselves through his testing method. But he also says that, "even if the same molecular markers that are involved in the pain process are not reflected in the blood, there are other indirect markers that should reflect the distress."
Niculescu expects his testing method will be available to the medical community at large within one to three years.
Willkie says she would welcome a reliable pain assessment method. Well-aware that she is not alone in her plight, she has more than 500 Facebook friends with sickle cell disease, and she says that "all of their opioid meds have been restricted or cut" as a result of the opioid crisis. Some now feel compelled to find their opioids "on the streets." She says she personally has never obtained opioids this way. Instead, she relies on marijuana to mitigate her pain.
Niculescu expects his testing method will be available to the medical community at large within one to three years: "It takes a while for things to translate from a lab setting to a commercial testing arena."
In the meantime, for Willkie and other patients, "we have to convince doctors and nurses that we're in pain."
Keep Reading
Keep Reading
Ray Cavanaugh is a freelance writer from Massachusetts. He enjoys very long walks, stopping occasionally to indulge in his Kindle Paperwhite.

Some people can eat red meat without negative health consequences, which may be due to variability between people's gut microbes.
(Photo by Sander Dalhuisen on Unsplash)
In different countries' national dietary guidelines, red meats (beef, pork, and lamb) are often confined to a very small corner. Swedish officials, for example, advise the population to "eat less red and processed meat". Experts in Greece recommend consuming no more than four servings of red meat — not per week, but per month.
"Humans 100% rely on the microbes to digest this food."
Yet somehow, the matter is far from settled. Quibbles over the scientific evidence emerge on a regular basis — as in a recent BMJ article titled, "No need to cut red meat, say new guidelines." News headlines lately have declared that limiting red meat may be "bad advice," while carnivore diet enthusiasts boast about the weight loss and good health they've achieved on an all-meat diet. The wildly successful plant-based burgers? To them, a gimmick. The burger wars are on.
Nutrition science would seem the best place to look for answers on the health effects of specific foods. And on one hand, the science is rather clear: in large populations, people who eat more red meat tend to have more health problems, including cardiovascular disease, colorectal cancer, and other conditions. But this sort of correlational evidence fails to settle the matter once and for all; many who look closely at these studies cite methodological shortcomings and a low certainty of evidence.
Some scientists, meanwhile, are trying to cut through the noise by increasing their focus on the mechanisms: exactly how red meat is digested and the step-by-step of how this affects human health. And curiously, as these lines of evidence emerge, several of them center around gut microbes as active participants in red meat's ultimate effects on human health.
Dr. Stanley Hazen, researcher and medical director of preventive cardiology at Cleveland Clinic, was one of the first to zero in on gut microorganisms as possible contributors to the health effects of red meat. In looking for chemical compounds in the blood that could predict the future development of cardiovascular disease, his lab identified a molecule called trimethylamine-N-oxide (TMAO). Little by little, he and his colleagues began to gather both human and animal evidence that TMAO played a role in causing heart disease.
Naturally, they tried to figure out where the TMAO came from. Hazen says, "We found that animal products, and especially red meat, were a dietary source that, [along with] gut microbes, would generate this product that leads to heart disease development." They observed that the gut microbes were essential for making TMAO out of dietary compounds (like red meat) that contained its precursor, trimethylamine (TMA).
So in linking red meat to cardiovascular disease through TMAO, the surprising conclusion, says Hazen, was that, "Without a doubt, [the microbes] are the most important aspect of the whole pathway."
"I think it's just a matter of time [before] we will have therapeutic interventions that actually target our gut microbes, just like the way we take drugs that lower cholesterol levels."
Other researchers have taken an interest in different red-meat-associated health problems, like colorectal cancer and the inflammation that accompanies it. This was the mechanistic link tackled by the lab of professor Karsten Zengler of the UC San Diego Departments of Pediatrics and Bioengineering—and it also led straight back to the gut microbes.
Zengler and colleagues recently published a paper in Nature Microbiology that focused on the effects of a red meat carbohydrate (or sugar) called Neu5Gc.
He explains, "If you eat animal proteins in your diet… the bound sugars in your diet are cleaved off in your gut and they get recycled. Your own cells will not recognize between the foreign sugars and your own sugars, because they look almost identical." The unsuspecting human cells then take up these foreign sugars — spurring antibody production and creating inflammation.
Zengler showed, however, that gut bacteria use enzymes to cleave off the sugar during digestion, stopping the inflammation and rendering the sugar harmless. "There's no enzyme in the human body that can cleave this [sugar] off. Humans 100% rely on the microbes to digest this food," he says.
Both researchers are quick to caution that the health effects of diet are complex. Other work indicates, for example, that while intake of red meat can affect TMAO levels, so can intake of fish and seafood. But these new lines of evidence could help explain why some people, ironically, seem to be in perfect health despite eating a lot of red meat: their ideal frequency of meat consumption may depend on their existing community of gut microbes.
"It helps explain what accounts for inter-person variability," Hazen says.
These emerging mechanisms reinforce overall why it's prudent to limit red meat, just as the nutritional guidelines advised in the first place. But both Hazen and Zengler predict that interventions to buffer the effects of too many ribeyes may be just around the corner.
Zengler says, "Our idea is that you basically can help your own digestive system detoxify these inflammatory compounds in meat, if you continue eating red meat or you want to eat a high amount of red meat." A possibly strategy, he says, is to use specific pre- or probiotics to cultivate an inflammation-reducing gut microbial community.
Hazen foresees the emergence of drugs that act not on the human, but on the human's gut microorganisms. "I think it's just a matter of time [before] we will have therapeutic interventions that actually target our gut microbes, just like the way we take drugs that lower cholesterol levels."
He adds, "It's a matter of 'stay tuned', I think."
Keep Reading
Keep Reading
Kristina Campbell is a Canadian writer who covers microbiome science for digital and print media around the world. She is author of The Well-Fed Microbiome Cookbook (Rockridge Press, 2016) and co-author of an academic textbook for health professionals, Gut Microbiota: Interactive Effects on Nutrition and Health (Elsevier, 2018).