

This Jarvik-7 artificial heart was used in the first bridge operation in 1985 meant to replace a failing heart while the patient waited for a donor organ.
In June, a team of surgeons at Duke University Hospital implanted the latest model of an artificial heart in a 39-year-old man with severe heart failure, a condition in which the heart doesn't pump properly. The man's mechanical heart, made by French company Carmat, is a new generation artificial heart and the first of its kind to be transplanted in the United States. It connects to a portable external power supply and is designed to keep the patient alive until a replacement organ becomes available.
Many patients die while waiting for a heart transplant, but artificial hearts can bridge the gap. Though not a permanent solution for heart failure, artificial hearts have saved countless lives since their first implantation in 1982.
What might surprise you is that the origin of the artificial heart dates back decades before, when an inventive television actor teamed up with a famous doctor to design and patent the first such device.
A man of many talents
Paul Winchell was an entertainer in the 1950s and 60s, rising to fame as a ventriloquist and guest-starring as an actor on programs like "The Ed Sullivan Show" and "Perry Mason." When children's animation boomed in the 1960s, Winchell made a name for himself as a voice actor on shows like "The Smurfs," "Winnie the Pooh," and "The Jetsons." He eventually became famous for originating the voices of Tigger from "Winnie the Pooh" and Gargamel from "The Smurfs," among many others.
But Winchell wasn't just an entertainer: He also had a quiet passion for science and medicine. Between television gigs, Winchell busied himself working as a medical hypnotist and acupuncturist, treating the same Hollywood stars he performed alongside. When he wasn't doing that, Winchell threw himself into engineering and design, building not only the ventriloquism dummies he used on his television appearances but a host of products he'd dreamed up himself. Winchell spent hours tinkering with his own inventions, such as a set of battery-powered gloves and something called a "flameless lighter." Over the course of his life, Winchell designed and patented more than 30 of these products – mostly novelties, but also serious medical devices, such as a portable blood plasma defroster.

| Ventriloquist Paul Winchell with Jerry Mahoney, his dummy, in 1951 |
A meeting of the minds
In the early 1950s, Winchell appeared on a variety show called the "Arthur Murray Dance Party" and faced off in a dance competition with the legendary Ricardo Montalban (Winchell won). At a cast party for the show later that same night, Winchell met Dr. Henry Heimlich – the same doctor who would later become famous for inventing the Heimlich maneuver, who was married to Murray's daughter. The two hit it off immediately, bonding over their shared interest in medicine. Before long, Heimlich invited Winchell to come observe him in the operating room at the hospital where he worked. Winchell jumped at the opportunity, and not long after he became a frequent guest in Heimlich's surgical theatre, fascinated by the mechanics of the human body.
One day while Winchell was observing at the hospital, he witnessed a patient die on the operating table after undergoing open-heart surgery. He was suddenly struck with an idea: If there was some way doctors could keep blood pumping temporarily throughout the body during surgery, patients who underwent risky operations like open-heart surgery might have a better chance of survival. Winchell rushed to Heimlich with the idea – and Heimlich agreed to advise Winchell and look over any design drafts he came up with. So Winchell went to work.
Winchell's heart
As it turned out, building ventriloquism dummies wasn't that different from building an artificial heart, Winchell noted later in his autobiography – the shifting valves and chambers of the mechanical heart were similar to the moving eyes and opening mouths of his puppets. After each design, Winchell would go back to Heimlich and the two would confer, making adjustments along the way to.
By 1956, Winchell had perfected his design: The "heart" consisted of a bag that could be placed inside the human body, connected to a battery-powered motor outside of the body. The motor enabled the bag to pump blood throughout the body, similar to a real human heart. Winchell received a patent for the design in 1963.
At the time, Winchell never quite got the credit he deserved. Years later, researchers at the University of Utah, working on their own artificial heart, came across Winchell's patent and got in touch with Winchell to compare notes. Winchell ended up donating his patent to the team, which included Dr. Richard Jarvik. Jarvik expanded on Winchell's design and created the Jarvik-7 – the world's first artificial heart to be successfully implanted in a human being in 1982.
The Jarvik-7 has since been replaced with newer, more efficient models made up of different synthetic materials, allowing patients to live for longer stretches without the heart clogging or breaking down. With each new generation of hearts, heart failure patients have been able to live relatively normal lives for longer periods of time and with fewer complications than before – and it never would have been possible without the unsung genius of a puppeteer and his love of science.

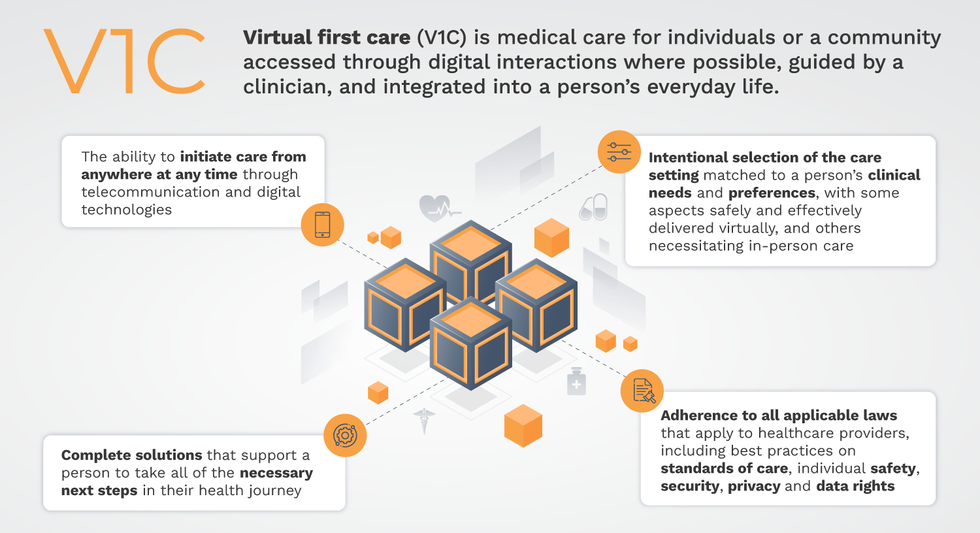
Virtual-first care, or V1C, could increase the quality of healthcare and make it more patient-centric by letting patients combine in-person visits with virtual options such as video for seeing their care providers.
That’s the idea behind virtual-first care (V1C), a new care model centered on convenient, customized, high-quality care that integrates a full suite of services tailored directly to patients’ clinical needs and preferences. This package includes asynchronous communication such as texting; video and other live virtual modes; and in-person options.
V1C goes beyond what you might think of as standard “telehealth” by using evidence-based protocols and tools that include traditional and digital therapeutics and testing, personalized care plans, dynamic patient monitoring, and team-based approaches to care. This could include spit kits mailed for laboratory tests and complementing clinical care with health coaching. V1C also replaces some in-person exams with ongoing monitoring, using sensors for more ‘whole person’ care.
Amidst all this momentum, we have the opportunity to rethink the goals of healthcare innovation, but that means bringing together key stakeholders to demonstrate that sustainable V1C can redefine healthcare.
Established V1C healthcare providers such as Omada, Headspace, and Heartbeat Health, as well as emerging market entrants like Oshi, Visana, and Wellinks, work with a variety of patients who have complicated long-term conditions such as diabetes, heart failure, gastrointestinal illness, endometriosis, and COPD. V1C is comprehensive in ways that are lacking in digital health and its other predecessors: it has the potential to integrate multiple data streams, incorporate more frequent touches and check-ins over time, and manage a much wider range of chronic health conditions, improving lives and reducing disease burden now and in the future.
Recognizing the pandemic-driven interest in virtual care, significant energy and resources are already flowing fast toward V1C. Some of the world’s largest innovators jumped into V1C early on: Verily, Alphabet’s Life Sciences Company, launched Onduo in 2016 to disrupt the diabetes healthcare market, and is now well positioned to scale its solutions. Major insurers like Aetna and United now offer virtual-first plans to members, responding as organizations expand virtual options for employees. Amidst all this momentum, we have the opportunity to rethink the goals of healthcare innovation, but that means bringing together key stakeholders to demonstrate that sustainable V1C can redefine healthcare.
That was the immediate impetus for IMPACT, a consortium of V1C companies, investors, payers and patients founded last year to ensure access to high-quality, evidence-based V1C. Developed by our team at the Digital Medicine Society (DiMe) in collaboration with the American Telemedicine Association (ATA), IMPACT has begun to explore key issues that include giving patients more integrated experiences when accessing both virtual and brick-and-mortar care.
Digital Medicine Society
V1C is not, nor should it be, virtual-only care. In this new era of hybrid healthcare, success will be defined by how well providers help patients navigate the transitions. How do we smoothly hand a patient off from an onsite primary care physician to, say, a virtual cardiologist? How do we get information from a brick-and-mortar to a digital portal? How do you manage dataflow while still staying HIPAA compliant? There are many complex regulatory implications for these new models, as well as an evolving landscape in terms of privacy, security and interoperability. It will be no small task for groups like IMPACT to determine the best path forward.
None of these factors matter unless the industry can recruit and retain clinicians. Our field is facing an unprecedented workforce crisis. Traditional healthcare is making clinicians miserable, and COVID has only accelerated the trend of overworked, disenchanted healthcare workers leaving in droves. Clinicians want more interactions with patients, and fewer with computer screens – call it “More face time, less FaceTime.” No new model will succeed unless the industry can more efficiently deploy its talent – arguably its most scarce and precious resource. V1C can help with alleviating the increasing burden and frustration borne by individual physicians in today’s status quo.
In healthcare, new technological approaches inevitably provoke no shortage of skepticism. Past lessons from Silicon Valley-driven fixes have led to understandable cynicism. But V1C is a different breed of animal. By building healthcare around the patient, not the clinic, V1C can make healthcare work better for patients, payers and providers. We’re at a fork in the road: we can revert back to a broken sick-care system, or dig in and do the hard work of figuring out how this future-forward healthcare system gets financed, organized and executed. As a field, we must find the courage and summon the energy to embrace this moment, and make it a moment of change.
