

A woman suffers from a debilitating headache during a hangover.
Probiotics seem to be everywhere these days. They are marketed for numerous health issues, from irritable bowel syndrome and vaginal yeast infections to life-threatening disorders like the bacterial infection Clostridium difficile.
The new probiotic drink is made of genetically engineered bacteria meant to help people feel better the day after drinking.
While the probiotic gummies that you'll find in supermarkets may not do much for you, good clinical evidence does support the C. difficile treatment, known as a fecal transplant, despite a recent setback, and there are always new probiotic regimens entering the scene. One emerging such treatment targets the hangover.
The Lowdown
You read that right – although "hangover" is a loaded term, according to ZBiotics, the company that's developing the product. The popular understanding of a hangover implies a collection of symptoms like a headache and fatigue, many of which result simply from dehydration and low-quality sleep. But those aren't the problems that the new product, a genetically engineered form of a common bacterial species, was developed to confront.
"Dehydration and poor sleep have actually always been pretty simple to deal with by having a good breakfast and some caffeine," notes ZBiotics founder and microbiologist Zack Abbott. Instead, the product targets acetaldehyde, a chemical that accumulates in the body if more than small amounts of alcohol are consumed.
Normally, body cells produce an enzyme that converts acetaldehyde into harmless acetic acid. But the enzyme becomes overwhelmed if you drink more than a little alcohol, or if you have a certain genetic deficiency.

A new probiotic drink aims to neutralize a chemical that builds up in the body after drinking alcohol.
(Zbiotics)
"I started ZBiotics with the hypothesis that if we used edible probiotic bacteria to make enzymes, and chose applications in which the enzymes these microbes make would be useful directly in the gut after you eat them, we could create all sorts of beneficial products," says Abbott. "I started with alcohol with the idea that we can augment the body's natural ability to digest its nasty byproduct, acetaldehyde, helping people feel better the day after drinking."
Next Steps
Based on the premise that the engineered bacteria augments a natural body function, ZBiotics had the product "sampled by thousands of beta-testers," including ZBiotics personnel, with "almost unanimously positive feedback," says Abbott.
"We are working on future scientifically controlled testing for publication."
ZBiotics is to set to launch on the market next week as a probiotic supplement, a category that does not require FDA approval. But some observers are troubled over whether the new product is attempting to serve a medical function without going through the standard drug testing process.
"I am skeptical of any new alternative product that is not FDA approved, has not undergone rigorous double-blind placebo control testing and adverse effects evaluation, and cites anecdotes as evidence of its efficacy," warns Heather Berlin, a cognitive neuroscientist and assistant professor of psychiatry at Icahn School of Medicine at Mount Sinai, in New York.
Abbott acknowledges that his product still needs to undergo rigorous study. "We are working on future scientifically controlled testing for publication," he says, noting that the company was "founded and [is] run by people with backgrounds in academic research."
Open Questions
Moving beyond the need for proper testing, Berlin has an additional concern: will a "hangover"-blocking substance cause people to drink more alcohol, or mask important physiological sensations like thirst?
"If that negative feeling is obscured, they may not [rehydrate], which can cause numerous adverse effects," Berlin says.
As for excessive drinking, there is a treatment on the market that does the opposite of Zbiotics. Disulfiram, commonly given to alcohol abusers, inhibits the very enzyme that ZBiotics supplements, causing acetaldehyde to accumulate especially fast. This makes drinking a pretty miserable experience.
But Abbott says his product would not interfere with disulfiram.
"[Zbiotics] is about enjoying the special moments in life where alcohol happens to be involved, but isn't the main focus."
"Disulfiram globally inhibits the enzyme throughout the entire body, including the liver, creating a massive amount of acetaldehyde at once, making the person ill immediately and forcing them to stop drinking right away," Abbott explains, whereas his product exerts its effects in the gut, and is really only helpful the next day. Thus, timing is everything; the probiotic would not change the experience at the moment of drinking.
"ZBiotics isn't about going out and ripping shots all night," Abbott says. "It's about enjoying the special moments in life where alcohol happens to be involved, but isn't the main focus. Weddings, celebrations, weekends with friends. And wanting to do that enjoyably while being safe and responsible at the same time."
Recent advancements in engineering mean that the first preclinical trials for an artificial kidney could happen as soon as 18 months from now
Still, the devices aren’t ready for testing in humans—yet. But recent advancements in engineering mean that the first preclinical trials for an artificial kidney could happen as soon as 18 months from now, according to Jonathan Himmelfarb, a nephrologist at the University of Washington.
“It would liberate people with kidney failure,” Himmelfarb says.
An engineering marvel
Compared to the heart or the brain, the kidney doesn’t get as much respect from the medical profession, but its job is far more complex. “It does hundreds of different things,” says UCLA’s Ira Kurtz.
Kurtz would know. He’s worked as a nephrologist for 37 years, devoting his career to helping those with kidney disease. While his colleagues in cardiology and endocrinology have seen major advances in the development of artificial hearts and insulin pumps, little has changed for patients on hemodialysis. The machines remain bulky and require large volumes of a liquid called dialysate to remove toxins from a patient’s blood, along with gallons of purified water. A kidney transplant is the next best thing to someone’s own, functioning organ, but with over 600,000 Americans on dialysis and only about 100,000 kidney transplants each year, most of those in kidney failure are stuck on dialysis.
Part of the lack of progress in artificial kidney design is the sheer complexity of the kidney’s job. Each of the 45 different cell types in the kidney do something different.
Part of the lack of progress in artificial kidney design is the sheer complexity of the kidney’s job. To build an artificial heart, Kurtz says, you basically need to engineer a pump. An artificial pancreas needs to balance blood sugar levels with insulin secretion. While neither of these tasks is simple, they are fairly straightforward. The kidney, on the other hand, does more than get rid of waste products like urea and other toxins. Each of the 45 different cell types in the kidney do something different, helping to regulate electrolytes like sodium, potassium, and phosphorous; maintaining blood pressure and water balance; guiding the body’s hormonal and inflammatory responses; and aiding in the formation of red blood cells.
There's been little progress for patients during Ira Kurtz's 37 years as a nephrologist. Artificial kidneys would change that.
UCLA
Dialysis primarily filters waste, and does so well enough to keep someone alive, but it isn’t a true artificial kidney because it doesn’t perform the kidney’s other jobs, according to Kurtz, such as sensing levels of toxins, wastes, and electrolytes in the blood. Due to the size and water requirements of existing dialysis machines, the equipment isn’t portable. Physicians write a prescription for a certain duration of dialysis and assess how well it’s working with semi-regular blood tests. The process of dialysis itself, however, is conducted blind. Doctors can’t tell how much dialysis a patient needs based on kidney values at the time of treatment, says Meera Harhay, a nephrologist at Drexel University in Philadelphia.
But it’s the impact of dialysis on their day-to-day lives that creates the most problems for patients. Only one-quarter of those on dialysis are able to remain employed (compared to 85% of similar-aged adults), and many report a low quality of life. Having more flexibility in life would make a major different to her patients, Harhay says.
“Almost half their week is taken up by the burden of their treatment. It really eats away at their freedom and their ability to do things that add value to their life,” she says.
Art imitates life
The challenge for artificial kidney designers was how to compress the kidney’s natural functions into a portable, wearable, or implantable device that wouldn’t need constant access to gallons of purified and sterilized water. The other universal challenge they faced was ensuring that any part of the artificial kidney that would come in contact with blood was kept germ-free to prevent infection.
As part of last year’s KidneyX Prize, a partnership between the U.S. Department of Health and Human Services and the American Society of Nephrology, inventors were challenged to create prototypes for artificial kidneys. Himmelfarb’s team at the University of Washington’s Center for Dialysis Innovation won the prize by focusing on miniaturizing existing technologies to create a portable dialysis machine. The backpack sized AKTIV device (Ambulatory Kidney to Increase Vitality) will recycle dialysate in a closed loop system that removes urea from blood and uses light-based chemical reactions to convert the urea to nitrogen and carbon dioxide, which allows the dialysate to be recirculated.
Himmelfarb says that the AKTIV can be used when at home, work, or traveling, which will give users more flexibility and freedom. “If you had a 30-pound device that you could put in the overhead bins when traveling, you could go visit your grandkids,” he says.
Kurtz’s team at UCLA partnered with the U.S. Kidney Research Corporation and Arkansas University to develop a dialysate-free desktop device (about the size of a small printer) as the first phase of a progression that will he hopes will lead to something small and implantable. Part of the reason for the artificial kidney’s size, Kurtz says, is the number of functions his team are cramming into it. Not only will it filter urea from blood, but it will also use electricity to help regulate electrolyte levels in a process called electrodeionization. Kurtz emphasizes that these additional functions are what makes his design a true artificial kidney instead of just a small dialysis machine.
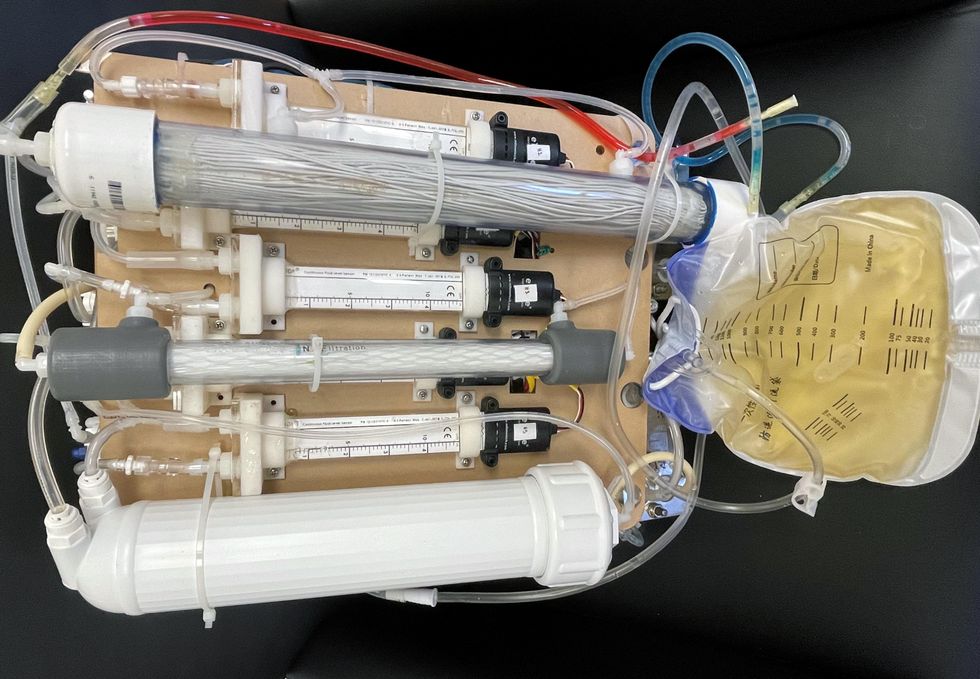
One version of an artificial kidney.
UCLA
“It doesn't have just a static function. It has a bank of sensors that measure chemicals in the blood and feeds that information back to the device,” Kurtz says.
Other startups are getting in on the game. Nephria Bio, a spinout from the South Korean-based EOFlow, is working to develop a wearable dialysis device, akin to an insulin pump, that uses miniature cartridges with nanomaterial filters to clean blood (Harhay is a scientific advisor to Nephria). Ian Welsford, Nephria’s co-founder and CTO, says that the device’s design means that it can also be used to treat acute kidney injuries in resource-limited settings. These potentials have garnered interest and investment in artificial kidneys from the U.S. Department of Defense.
For his part, Burton is most interested in an implantable device, as that would give him the most freedom. Even having a regular outpatient procedure to change batteries or filters would be a minor inconvenience to him.
“Being plugged into a machine, that’s not mimicking life,” he says.
