

Which foods are actually healthy for your individual gut microbiome? Several companies are offering personalized dietary guidance based on your test results, but their answers in one experiment turned up with some conflicting advice.
I recently got on the scale to weigh myself, thinking I've got to eat better. With so many trendy diets today claiming to improve health, from Keto to Paleo to Whole30, it can be confusing to figure out what we should and shouldn't eat for optimal nutrition.
A number of companies are now selling the concept of "personalized" nutrition based on the genetic makeup of your individual gut bugs.
My next thought was: I've got to lose a few pounds.
Consider a weird factoid: In addition to my fat, skin, bone and muscle, I'm carrying around two or three pounds of straight-up bacteria. Like you, I am the host to trillions of micro-organisms that live in my gut and are collectively known as my microbiome. An explosion of research has occurred in the last decade to try to understand exactly how these microbial populations, which are unique to each of us, may influence our overall health and potentially even our brains and behavior.
Lots of mysteries still remain, but it is established that these "bugs" are crucial to keeping our body running smoothly, performing functions like stimulating the immune system, synthesizing important vitamins, and aiding digestion. The field of microbiome science is evolving rapidly, and a number of companies are now selling the concept of "personalized" nutrition based on the genetic makeup of your individual gut bugs. The two leading players are Viome and DayTwo, but the landscape includes the newly launched startup Onegevity Health and others like Thryve, which offers customized probiotic supplements in addition to dietary recommendations.
The idea has immediate appeal – if science could tell you exactly what to make for lunch and what to avoid, you could forget about the fad diets and go with your own bespoke food pyramid. Wondering if the promise might be too good to be true, I decided to perform my own experiment.
Last fall, I sent the identical fecal sample to both Viome (I paid $425, but the price has since dropped to $299) and DayTwo ($349). A couple of months later, both reports finally arrived, and I eagerly opened each app to compare their recommendations.
First, I examined my results from Viome, which was founded in 2016 in Cupertino, Calif., and declares without irony on its website that "conflicting food advice is now obsolete."
I learned I have "average" metabolic fitness and "average" inflammatory activity in my gut, which are scores that the company defines based on a proprietary algorithm. But I have "low" microbial richness, with only 62 active species of bacteria identified in my sample, compared with the mean of 157 in their test population. I also received a list of the specific species in my gut, with names like Lactococcus and Romboutsia.
But none of it meant anything to me without actionable food advice, so I clicked through to the Recommendations page and found a list of My Superfoods (cranberry, garlic, kale, salmon, turmeric, watermelon, and bone broth) and My Foods to Avoid (chickpeas, kombucha, lentils, and rice noodles). There was also a searchable database of many foods that had been categorized for me, like "bell pepper; minimize" and "beef; enjoy."
"I just don't think sufficient data is yet available to make reliable personalized dietary recommendations based on one's microbiome."
Next, I looked at my results from DayTwo, which was founded in 2015 from research out of the Weizmann Institute of Science in Israel, and whose pitch to consumers is, "Blood sugar made easy. The algorithm diet personalized to you."
This app had some notable differences. There was no result about my metabolic fitness, microbial richness, or list of the species in my sample. There was also no list of superfoods or foods to avoid. Instead, the app encouraged me to build a meal by searching for foods in their database and combining them in beneficial ways for my blood sugar. Two slices of whole wheat bread received a score of 2.7 out of 10 ("Avoid"), but if combined with one cup of large curd cottage cheese, the score improved to 6.8 ("Limit"), and if I added two hard-boiled eggs, the score went up to 7.5 ("Good").
Perusing my list of foods with "Excellent" scores, I noticed some troubling conflicts with the other app. Lentils, which had been a no-no according to Viome, received high marks from DayTwo. Ditto for Kombucha. My purported superfood of cranberry received low marks. Almonds got an almost perfect score (9.7) while Viome told me to minimize them. I found similarly contradictory advice for foods I regularly eat, including navel oranges, peanuts, pork, and beets.
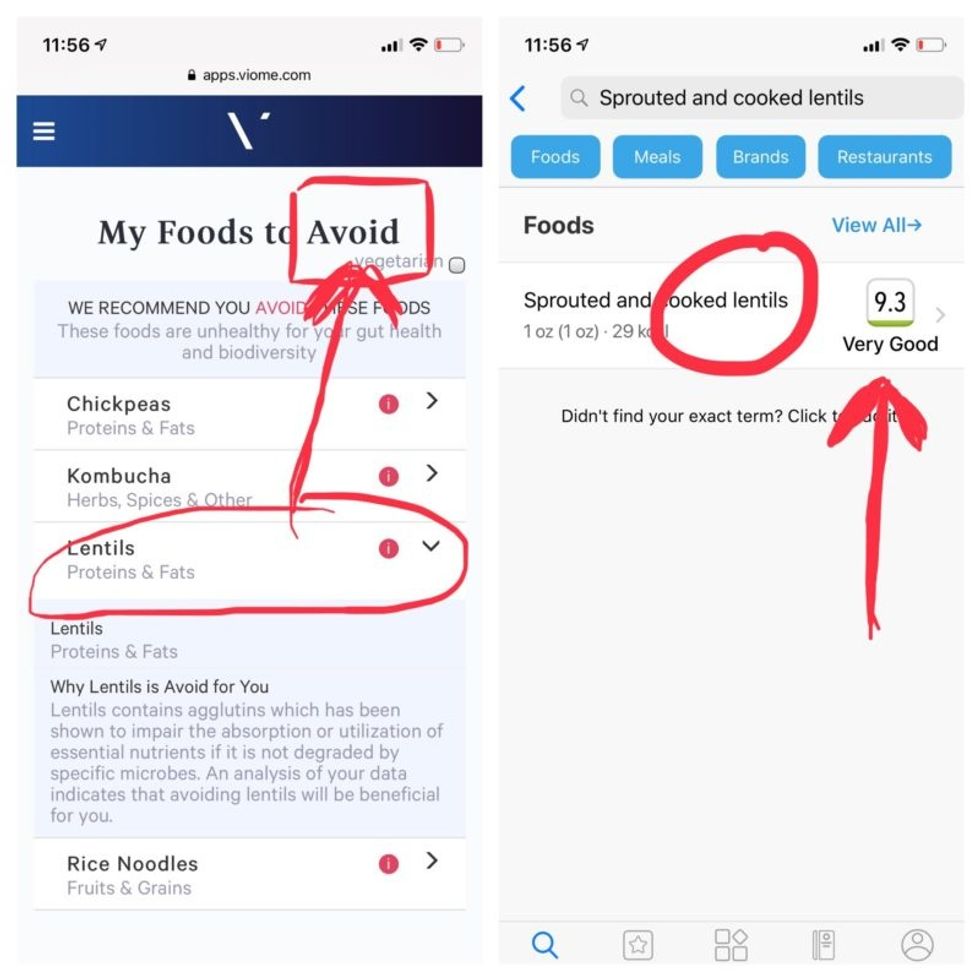
Contradictory dietary guidance that Kira Peikoff received from Viome (left) and DayTwo from an identical sample.
To be sure, there was some overlap. Both apps agreed on rice noodles (bad), chickpeas (bad), honey (bad), carrots (good), and avocado (good), among other foods.
But still, I was left scratching my head. Which set of recommendations should I trust, if either? And what did my results mean for the accuracy of this nascent field?
I called a couple of experts to find out.
"I have worked on the microbiome and nutrition for the last 20 years and I would be absolutely incapable of finding you evidence in the scientific literature that lentils have a detrimental effect based on the microbiome," said Dr. Jens Walter, an Associate Professor and chair for Nutrition, Microbes, and Gastrointestinal Health at the University of Alberta. "I just don't think sufficient data is yet available to make reliable personalized dietary recommendations based on one's microbiome. And even if they would have proprietary algorithms, at least one of them is not doing it right."
There is definite potential for personalized nutrition based on the microbiome, he said, but first, predictive models must be built and standardized, then linked to clinical endpoints, and tested in a large sample of healthy volunteers in order to enable extrapolations for the general population.
"It is mindboggling what you would need to do to make this work," he observed. "There are probably hundreds of relevant dietary compounds, then the microbiome has at least a hundred relevant species with a hundred or more relevant genes each, then you'd have to put all this together with relevant clinical outcomes. And there's a hundred-fold variation in that information between individuals."
However, Walter did acknowledge that the companies might be basing their algorithms on proprietary data that could potentially connect all the dots. I reached out to them to find out.
Amir Golan, the Chief Commercial Officer of DayTwo, told me, "It's important to emphasize this is a prediction, as the microbiome field is in a very early stage of research." But he added, "I believe we are the only company that has very solid science published in top journals and we can bring very actionable evidence and benefit to our uses."
He was referring to pioneering work out of the Weizmann Institute that was published in 2015 in the journal Cell, which logged the glycemic responses of 800 people in response to nearly 50,000 meals; adding information about the subjects' microbiomes enabled more accurate glycemic response predictions. Since then, Golan said, additional trials have been conducted, most recently with the Mayo Clinic, to duplicate the results, and other studies are ongoing whose results have not yet been published.
He also pointed out that the microbiome was merely one component that goes into building a client's profile, in addition to medical records, including blood glucose levels. (I provided my HbA1c levels, a measure of average blood sugar over the previous several months.)
"We are not saying we want to improve your gut microbiome. We provide a dynamic tool to help guide what you should eat to control your blood sugar and think about combinations," he said. "If you eat one thing, or with another, it will affect you in a different way."
Viome acknowledged that the two companies are taking very different approaches.
"DayTwo is primarily focused on the glycemic response," Naveen Jain, the CEO, told me. "If you can only eat butter for rest of your life, you will have no glycemic response but will probably die of a heart attack." He laughed. "Whereas we came from very different angle – what is happening inside the gut at a microbial level? When you eat food like spinach, how will that be metabolized in the gut? Will it produce the nutrients you need or cause inflammation?"
He said his team studied 1000 people who were on continuous glucose monitoring and fed them 45,000 meals, then built a proprietary data prediction model, looking at which microbes existed and how they actively broke down the food.
Jain pointed out that DayTwo sequences the DNA of the microbes, while Viome sequences the RNA – the active expression of DNA. That difference, in his opinion, is key to making accurate predictions.
"DNA is extremely stable, so when you eat any food and measure the DNA [in a fecal sample], you get all these false positives--you get DNA from plant food and meat, and you have no idea if those organisms are dead and simply transient, or actually exist. With RNA, you see what is actually alive in the gut."
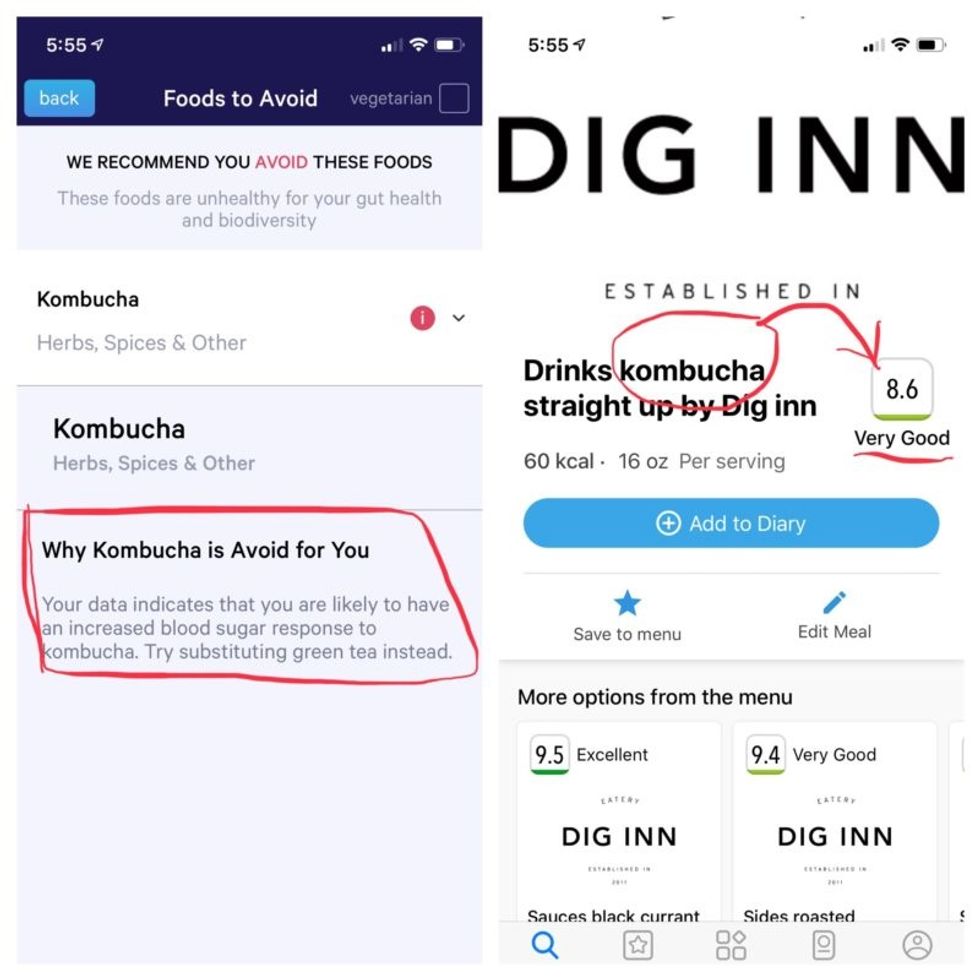
More contradictory food advice from Viome (left) and DayTwo.
Note that controversy exists over how it is possible with a fecal sample to effectively measure RNA, which degrades within minutes, though Jain said that his company has the technology to keep RNA stable for fourteen days.
Viome's approach, Jain maintains, is 90 percent accurate, based on as-yet unpublished data; a patent was filed just last week. DayTwo's approach is 66 percent accurate according to the latest published research.
Natasha Haskey, a registered dietician and doctoral student conducting research in the field of microbiome science and nutrition, is skeptical of both companies. "We can make broad statements, like eat more fruits and vegetables and fiber, but when it comes to specific foods, the science is just not there yet," she said. "I think there is a future, and we will be doing that someday, but not yet. Maybe we will be closer in ten years."
Professor Walter wholeheartedly agrees with Haskey, and suggested that if people want to eat a gut-healthy diet, they should focus on beneficial oils, fruits and vegetables, fish, a variety of whole grains, poultry and beans, and limit red meat and cheese, as well as avoid processed meats.
"These services are far over the tips of their science skis," Arthur Caplan, the founding head of New York University's Division of Medical Ethics, said in an email. "We simply don't know enough about the gut microbiome, its fluctuations and variability from person to person to support general [direct-to-consumer] testing. This is simply premature. We need standards for accuracy, specificity, and sensitivity, plus mandatory competent counseling for all such testing. They don't exist. Neither should DTC testing—yet."
Meanwhile, it's time for lunch. I close out my Viome and DayTwo apps and head to the kitchen to prepare a peanut butter sandwich. My gut tells me I'll be just fine.


Recent immigration restrictions have left many foreign researchers' projects and careers in limbo—and some in jeopardy.
"I spent about $4,000 on lawyer fees and another $1,200 to pay for the motions I filed," she recalls. "I had to borrow money from my parents and my cousin because without my salary I just didn't have the $7,000 at hand." But the already narrow window of opportunity slammed completely shut when the Trump administration suspended issuing new visas for foreign researchers in June. All Mohan's attempts were denied. In August, she had to leave the country. "Given the recent work visa ban by the administration, all my options in the U.S. are closed," she wrote a bitter note on Twitter. "I have to uproot my entire life in NY for the past 6 years and leave." She eventually found a temporary position in Calcutta, where she can continue research.
Mohan is hardly alone in her visa saga. Many foreign scholars on H- and J-type visas and other permits that let them remain employed in America had been struggling to keep their rights to continue research, which in certain cases is crucial to battling the pandemic. Some had to leave the country, some filed every possible extension to buy time, and others are stuck in their home countries, unable to return. The already cumbersome process of applying for visas and extensions became crippled during the lockdowns. But in June, when President Trump extended and expanded immigration restrictions to cut the number of immigrant workers entering the U.S., the new limits left researchers' projects and careers in limbo—and some in jeopardy.
"We have been a beneficiary of this flow of human capacity and resource investment for many generations—and this is now threatened."
Rakesh Ramachandran, whose computational biology work contributed to one of the first coronavirus studies to map out its protein structures—is stranded in India. In early March, he had travelled there to attend a conference and visit the American consulate to stamp his H1 visa for a renewal, already granted. The pandemic shut down both the conference and the consulates, and Ramachandran hasn't been able to come back since. The consulates finally opened in September, but so far the online portal has no available appointment slots. "I'm told to keep trying," Ramachandran says.
The visa restrictions affected researchers worldwide, regardless of disciplines or countries. A Ph.D. student in neuroscience, Morgane Leroux had to do her experiments with mice at Gladstone Institutes in America and analyze the data back home at Sorbonne University in France. She had finished her first round of experiments when the lockdowns forced her to return to Paris, and she hasn't been able to come back to resume her work since. "I can't continue the experiments, which is really frustrating," she says, especially because she doesn't know what it means for her Ph.D. "I may have to entirely change my subject," she says, which she doesn't want to do—it would be a waste of time and money.
But besides wreaking havoc in scholars' personal lives and careers, the visa restrictions had—and will continue to have—tremendous deleterious effects on America's research and its global scientific competitiveness. "It's incredibly short-sighted and self-destructing to restrict the immigration of scientists into the U.S.," says Benjamin G. Neel, who directs the Laura and Isaac Perlmutter Cancer Center at New York University. "If they can't come here, they will go elsewhere," he says, causing a brain drain.

Neel in his lab with postdocs
(Courtesy of Neel)
Neel felt the outcomes of the shortsighted policies firsthand. In the past few months, his lab lost two postdoctoral researchers who had made major strides in understanding the biology of several particularly stubborn, treatment-resistant malignancies. One postdoc studied the underlying mechanisms responsible for 90 percent of pancreatic cancers and half of the colon ones. The other one devised a new system of modeling ovarian cancer in mice to test new therapeutic drug combinations for the deadliest tumor types—but had to return home to China.
"By working around the clock, she was able to get her paper accepted, but she hasn't been able to train us to use this new system, which can set us back six months," Neel says.
Her discoveries also helped the lab secure about $900,000 in grants for new research. Losing people like this is "literally killing the goose that lays the golden eggs," Neel adds. "If you want to make America poor again, this is the way to do it."
Cassidy R. Sugimoto at Indiana University Bloomington, who studies how scientific knowledge is produced and disseminated, says that scientists are the most productive when they are free to move, exchange ideas, and work at labs with the best equipment. Restricting that freedom reduces their achievement.
"Several empirical studied demonstrated the benefits to the U.S. by attracting and retaining foreign scientists. The disproportional number of our Nobel Prize winners were not only foreign-born but also foreign-educated," she says. Scientific advancement bolsters the country's economic prowess, too, so turning scholars away is bad for the economy long-term. "We have been a beneficiary of this flow of human capacity and resource investment for many generations—and this is now threatened," Sugimoto adds—because scientists will look elsewhere. "We are seeing them shifting to other countries that are more hospitable, both ideologically and in terms of health security. Many visiting scholars, postdocs, and graduate students who would otherwise come to the United States are now moving to Canada."
It's not only the Ph.D. students and postdocs who are affected. In some cases, even well-established professors who have already made their marks in the field and direct their own labs at prestigious research institutions may have to pack up and leave the country in the next few months. One scientist who directs a prominent neuroscience lab is betting on his visa renewal and a green card application, but if that's denied, the entire lab may be in jeopardy, as many grants hinge on his ability to stay employed in America.
"It's devastating to even think that it can happen," he says—after years of efforts invested. "I can't even comprehend how it would feel. It would be terrifying and really sad." (He asked to withhold his name for fear that it may adversely affect his applications.) Another scientist who originally shared her story for this article, later changed her mind and withdrew, worrying that speaking out may hurt the entire project, a high-profile COVID-19 effort. It's not how things should work in a democratic country, scientists admit, but that's the reality.
Still, some foreign scholars are speaking up. Mehmet Doğan, a physicist at University of California Berkeley who has been fighting a visa extension battle all year, says it's important to push back in an organized fashion with petitions and engage legislators. "This administration was very creative in finding subtle and not so subtle ways to make our lives more difficult," Doğan says. He adds that the newest rules, proposed by the Department of Homeland Security on September 24, could further limit the time scholars can stay, forcing them into continuous extension battles. That's why the upcoming election might be a turning point for foreign academics. "This election will decide if many of us will see the U.S. as the place to stay and work or whether we look at other countries," Doğan says, echoing the worries of Neel, Sugimoto, and others in academia.

Dogan on Zoom talking to his fellow union members of the Academic Researchers United, a union of almost 5,000 Academic Researchers.
(Credit: Ceyda Durmaz Dogan)
If this year has shown us anything, it is that viruses and pandemics know no borders as they sweep across the globe. Likewise, science can't be restrained by borders either. "Science is an international endeavor," says Neel—and right now humankind now needs unified scientific research more than ever, unhindered by immigration hurdles and visa wars. Humanity's wellbeing in America and beyond depends on it.
[Editor's Note: To read other articles in this special magazine issue, visit the beautifully designed e-reader version.]