

Scientists are making progress to create a one-time therapy that would permanently lower LDL cholesterol to prevent heart attacks caused by high LDL.
Later this year, Verve Therapeutics of Cambridge, Ma., will initiate Phase 1 clinical trials to test VERVE-101, a new medication that, if successful, will employ gene editing to significantly reduce low-density lipoprotein cholesterol, or LDL.
LDL is sometimes referred to as the “bad” cholesterol because it collects in the walls of blood vessels, and high levels can increase chances of a heart attack, cardiovascular disease or stroke. There are approximately 600,000 heart attacks per year due to blood cholesterol damage in the United States, and heart disease is the number one cause of death in the world. According to the CDC, a 10 percent decrease in total blood cholesterol levels can reduce the incidence of heart disease by as much as 30 percent.
Verve’s Founder and CEO, Sekar Kathiresan, spent two decades studying the genetic basis for heart attacks while serving as a professor of medicine at Harvard Medical School. His research led to two critical insights.
“One is that there are some people that are naturally resistant to heart attack and have lifelong, low levels of LDL,” the cardiologist says. “Second, there are some genes that can be switched off that lead to very low LDL cholesterol, and individuals with those genes switched off are resistant to heart attacks.”
Kathiresan and his team formed a hypothesis in 2016 that if they could develop a medicine that mimics the natural protection that some people enjoy, then they might identify a powerful new way to treat and ultimately prevent heart attacks. They launched Verve in 2018 with the goal of creating a one-time therapy that would permanently lower LDL and eliminate heart attacks caused by high LDL.
"Imagine a future where somebody gets a one-time treatment at the time of their heart attack or before as a preventive measure," says Kathiresan.
The medication is targeted specifically for patients who have a genetic form of high cholesterol known as heterozygous familial hypercholesterolemia, or FH, caused by expression of a gene called PCSK9. Verve also plans to develop a program to silence a gene called ANGPTL3 for patients with FH and possibly those with or at risk of atherosclerotic cardiovascular disease.
FH causes cholesterol to be high from birth, reaching levels of 200 to 300 milligrams per deciliter. Suggested normal levels are around 100 to 129 mg/dl, and anything above 130 mg/dl is considered high. Patients with cardiovascular disease usually are asked to aim for under 70 mg/dl, but many still have unacceptably high LDL despite taking oral medications such as statins. They are more likely to have heart attacks in their 30s, 40s and 50s, and require lifelong LDL control.
The goal for drug treatments for high LDL, Kathiresan says, is to reduce LDL as low as possible for as long as possible. Physicians and researchers also know that a sizeable portion of these patients eventually start to lose their commitment to taking their statins and other LDL-controlling medications regularly.
“If you ask 100 patients one year after their heart attack what fraction are still taking their cholesterol-lowering medications, it’s less than half,” says Kathiresan. “So imagine a future where somebody gets a one-time treatment at the time of their heart attack or before as a preventive measure. It’s right in front of us, and it’s something that Verve is looking to do.”
In late 2020, Verve completed primate testing with monkeys that had genetically high cholesterol, using a one-time intravenous injection of VERVE-101. It reduced the monkeys’ LDL by 60 percent and, 18 months later, remains at that level. Kathiresan expects the LDL to stay low for the rest of their lives.
Verve’s gene editing medication is packaged in a lipid nanoparticle to serve as the delivery mechanism into the liver when infused intravenously. The drug is absorbed and makes its way into the nucleus of the liver cells.
Verve’s program targeting PCSK9 uses precise, single base, pair base editing, Kathiresan says, meaning it doesn't cut DNA like CRISPR gene editing systems do. Instead, it changes one base, or letter, in the genome to a different one without affecting the letters around it. Comparing it to a pencil and eraser, he explains that the medication erases out a letter A and makes it a letter G in the A, C, G and T code in DNA.
“We need to continue to advance our approach and tools to make sure that we have the absolute maximum ability to detect off-target effects,” says Euan Ashley, professor of medicine and genetics at Stanford University.
By making that simple change from A to G, the medication switches off the PCSK9 gene, automatically lowering LDL cholesterol.
“Once the DNA change is made, all the cells in the liver will have that single A to G change made,” Kathiresan says. “Then the liver cells divide and give rise to future liver cells, but every time the cell divides that change, the new G is carried forward.”
Additionally, Verve is pursuing its second gene editing program to eliminate ANGPTL3, a gene that raises both LDL and blood triglycerides. In 2010, Kathiresan's research team learned that people who had that gene completely switched off had LDL and triglyceride levels of about 20 and were very healthy with no heart attacks. The goal of Verve’s medication will be to switch off that gene, too, as an option for additional LDL or triglyceride lowering.
“Success with our first drug, VERVE-101, will give us more confidence to move forward with our second drug,” Kathiresan says. “And it opens up this general idea of making [genomic] spelling changes in the liver to treat other diseases.”
The approach is less ethically concerning than other gene editing technologies because it applies somatic editing that affects only the individual patient, whereas germline editing in the patient’s sperm or egg, or in an embryo, gets passed on to children. Additionally, gene editing therapies receive the same comprehensive amount of testing for side effects as any other medicine.
“We need to continue to advance our approach and tools to make sure that we have the absolute maximum ability to detect off-target effects,” says Euan Ashley, professor of medicine and genetics at Stanford University and founding director of its Center for Inherited Cardiovascular Disease. Ashley and his colleagues at Stanford’s Clinical Genomics Program and beyond are increasingly excited about the promise of gene editing.
“We can offer precision diagnostics, so increasingly we’re able to define the disease at a much deeper level using molecular tools and sequencing,” he continues. “We also have this immense power of reading the genome, but we’re really on the verge of taking advantage of the power that we now have to potentially correct some of the variants that we find on a genome that contribute to disease.”
He adds that while the gene editing medicines in development to correct genomes are ahead of the delivery mechanisms needed to get them into the body, particularly the heart and brain, he’s optimistic that those aren’t too far behind.
“It will probably take a few more years before those next generation tools start to get into clinical trials,” says Ashley, whose book, The Genome Odyssey, was published last year. “The medications might be the sexier part of the research, but if you can’t get it into the right place at the right time in the right dose and not get it to the places you don’t want it to go, then that tool is not of much use.”
Medical experts consider knocking out the PCSK9 gene in patients with the fairly common genetic disorder of familial hypercholesterolemia – roughly one in 250 people – a potentially safe approach to gene editing and an effective means of significantly lowering their LDL cholesterol.

Nurse Erin McGlennon has an Implantable Cardioverter Defibrillator and takes medications, but she is also hopeful that a gene editing medication will be developed in the near future.
Erin McGlennon
Mary McGowan, MD, chief medical officer for The Family Heart Foundation in Pasadena, CA, sees the tremendous potential for VERVE-101 and believes patients should be encouraged by the fact that this kind of research is occurring and how much Verve has accomplished in a relatively short time. However, she offers one caveat, since even a 60 percent reduction in LDL won’t completely eliminate the need to reduce the remaining amount of LDL.
“This technology is very exciting,” she said, “but we want to stress to our patients with familial hypercholesterolemia that we know from our published research that most people require several therapies to get their LDL down., whether that be in primary prevention less than 100 mg/dl or secondary prevention less than 70 mg/dl, So Verve’s medication would be an add-on therapy for most patients.”
Dr. Kathiresan concurs: “We expect our medicine to lower LDL cholesterol by about 60 percent and that our patients will be on background oral medications, including statins that lower LDL cholesterol.”
Several leading research centers are investigating gene editing treatments for other types of cardiovascular diseases. Elizabeth McNally, Elizabeth Ward Professor and Director at the Center for Genetic Medicine at Northwestern University’s Feinberg School of Medicine, pursues advanced genetic correction in neuromuscular diseases such as Duchenne muscular dystrophy and spinal muscular atrophy. A cardiologist, she and her colleagues know these diseases frequently have cardiac complications.
“Even though the field is driven by neuromuscular specialists, it’s the first therapies in patients with neuromuscular diseases that are also expected to make genetic corrections in the heart,” she says. “It’s almost like an afterthought that we’re potentially fixing the heart, too.”
Another limitation McGowan sees is that too many healthcare providers are not yet familiar with how to test patients to determine whether or not they carry genetic mutations that need to be corrected. “We need to get more genetic testing done,” she says. “For example, that’s the case with hypertrophic cardiomyopathy, where a lot of the people who probably carry that diagnosis and have never been genetically identified at a time when genetic testing has never been easier.”
One patient who has been diagnosed with hypertrophic cardiomyopathy also happens to be a nurse working in research at Genentech Pharmaceutical, now a member of the Roche Group, in South San Francisco. To treat the disease, Erin McGlennon, RN, has an Implantable Cardioverter Defibrillator and takes medications, but she is also hopeful that a gene editing medication will be developed in the near future.
“With my condition, the septum muscles are just growing thicker, so I’m on medicine to keep my heart from having dangerous rhythms,” says McGlennon of the disease that carries a low risk of sudden cardiac death. “So, the possibility of having a treatment option that can significantly improve my day-to-day functioning would be a major breakthrough.”
McGlennon has some control over cardiovascular destiny through at least one currently available technology: in vitro fertilization. She’s going through it to ensure that her children won't express the gene for hypertrophic cardiomyopathy.


Doctors worry that fungal pathogens may cause the next pandemic.
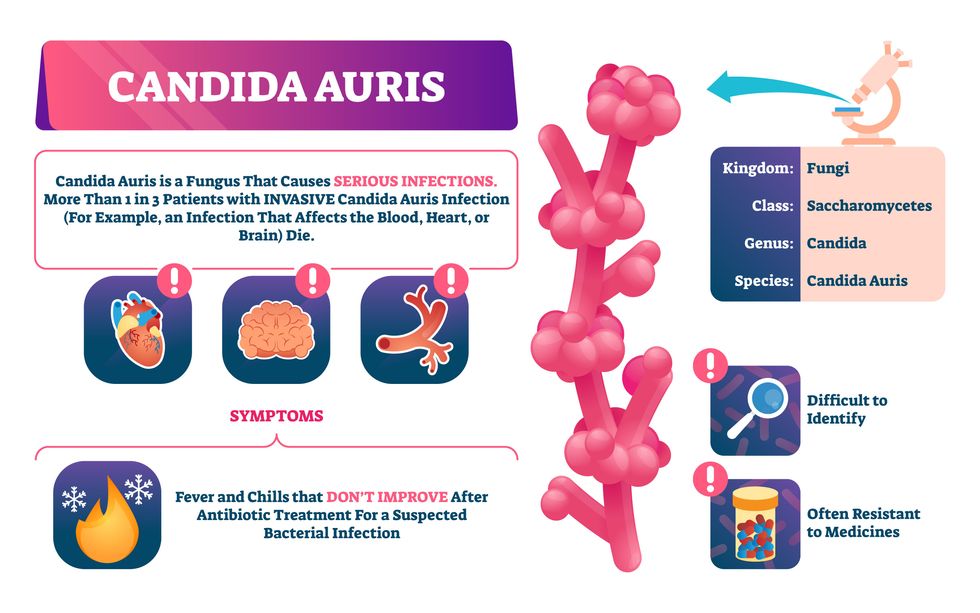
Although C. auris typically doesn’t sicken healthy people, it afflicts immunocompromised hospital patients and may cause severe infections that can lead to sepsis, a life-threatening condition in which the overwhelmed immune system begins to attack the body’s own organs. Between 30 and 60 percent of patients who contract a C. auris infection die from it, according to the CDC. People who are undergoing stem cell transplants, have catheters or have taken antifungal or antibiotic medicines are at highest risk. “We’re coming to a perfect storm of increasing resistance rates, increasing numbers of immunosuppressed patients worldwide and a bug that is adapting to higher temperatures as the climate changes,” says Prabhavathi Fernandes, chair of the National BioDefense Science Board.
Most Candida species aren’t well-adapted to our body temperatures so they aren’t a threat. C. auris, however, thrives at human body temperatures.
Although medical professionals aren’t concerned at this point about C. auris evolving to affect healthy people, they worry that its presence in hospitals can turn routine surgeries into life-threatening calamities. “It’s coming,” says Fernandes. “It’s just a matter of time.”
An emerging global threat
“Fungi are found in the environment,” explains Fernandes, so Candida spores can easily wind up on people’s skin. In hospitals, they can be transferred from contact with healthcare workers or contaminated surfaces. Most Candida species aren’t well-adapted to our body temperatures so they aren’t a threat. C. auris, however, thrives at human body temperatures. It can enter the body during medical treatments that break the skin—and cause an infection. Overall, fungal infections cost some $48 billion in the U.S. each year. And infection rates are increasing because, in an ironic twist, advanced medical therapies are enabling severely ill patients to live longer and, therefore, be exposed to this pathogen.
The first-ever case of a C. auris infection was reported in Japan in 2009, although an analysis of Candida samples dated the earliest strain to a 1996 sample from South Korea. Since then, five separate varieties – called clades, which are similar to strains among bacteria – developed independently in different geographies: South Asia, East Asia, South Africa, South America and, recently, Iran. So far, C. auris infections have been reported in 35 countries.
In the U.S., the first infection was reported in 2016, and the CDC started tracking it nationally two years later. During that time, 5,654 cases have been reported to the CDC, which only tracks U.S. data.
What’s more notable than the number of cases is their rate of increase. In 2016, new cases increased by 175 percent and, on average, they have approximately doubled every year. From 2016 through 2022, the number of infections jumped from 63 to 2,377, a roughly 37-fold increase.
“This reminds me of what we saw with epidemics from 2013 through 2020… with Ebola, Zika and the COVID-19 pandemic,” says Robin Robinson, CEO of Spriovas and founding director of the Biomedical Advanced Research and Development Authority (BARDA), which is part of the U.S. Department of Health and Human Services. These epidemics started with a hockey stick trajectory, Robinson says—a gradual growth leading to a sharp spike, just like the shape of a hockey stick.
Another challenge is that right now medics don’t have rapid diagnostic tests for fungal infections. Currently, patients are often misdiagnosed because C. auris resembles several other easily treated fungi. Or they are diagnosed long after the infection begins and is harder to treat.
The problem is that existing diagnostics tests can only identify C. auris once it reaches the bloodstream. Yet, because this pathogen infects bodily tissues first, it should be possible to catch it much earlier before it becomes life-threatening. “We have to diagnose it before it reaches the bloodstream,” Walsh says.
The most alarming fact is that some Candida infections no longer respond to standard therapeutics.
“We need to focus on rapid diagnostic tests that do not rely on a positive blood culture,” says John Sperzel, president and CEO of T2 Biosystems, a company specializing in diagnostics solutions. Blood cultures typically take two to three days for the concentration of Candida to become large enough to detect. The company’s novel test detects about 90 percent of Candida species within three to five hours—thanks to its ability to spot minute quantities of the pathogen in blood samples instead of waiting for them to incubate and proliferate.
Unlike other Candida species C. auris thrives at human body temperatures
Adobe Stock
Tackling the resistance challenge
The most alarming fact is that some Candida infections no longer respond to standard therapeutics. The number of cases that stopped responding to echinocandin, the first-line therapy for most Candida infections, tripled in 2020, according to a study by the CDC.
Now, each of the first four clades shows varying levels of resistance to all three commonly prescribed classes of antifungal medications, such as azoles, echinocandins, and polyenes. For example, 97 percent of infections from C. auris Clade I are resistant to fluconazole, 54 percent to voriconazole and 30 percent of amphotericin. Nearly half are resistant to multiple antifungal drugs. Even with Clade II fungi, which has the least resistance of all the clades, 11 to 14 percent have become resistant to fluconazole.
Anti-fungal therapies typically target specific chemical compounds present on fungi’s cell membranes, but not on human cells—otherwise the medicine would cause damage to our own tissues. Fluconazole and other azole antifungals target a compound called ergosterol, preventing the fungal cells from replicating. Over the years, however, C. auris evolved to resist it, so existing fungal medications don’t work as well anymore.
A newer class of drugs called echinocandins targets a different part of the fungal cell. “The echinocandins – like caspofungin – inhibit (a part of the fungi) involved in making glucan, which is an essential component of the fungal cell wall and is not found in human cells,” Fernandes says. New antifungal treatments are needed, she adds, but there are only a few magic bullets that will hit just the fungus and not the human cells.
Research to fight infections also has been challenged by a lack of government support. That is changing now that BARDA is requesting proposals to develop novel antifungals. “The scope includes C. auris, as well as antifungals following a radiological/nuclear emergency, says BARDA spokesperson Elleen Kane.
The remaining challenge is the number of patients available to participate in clinical trials. Large numbers are needed, but the available patients are quite sick and often die before trials can be completed. Consequently, few biopharmaceutical companies are developing new treatments for C. auris.
ClinicalTrials.gov reports only two drugs in development for invasive C. auris infections—those than can spread throughout the body rather than localize in one particular area, like throat or vaginal infections: ibrexafungerp by Scynexis, Inc., fosmanogepix, by Pfizer.
Scynexis’ ibrexafungerp appears active against C. auris and other emerging, drug-resistant pathogens. The FDA recently approved it as a therapy for vaginal yeast infections and it is undergoing Phase III clinical trials against invasive candidiasis in an attempt to keep the infection from spreading.
“Ibreafungerp is structurally different from other echinocandins,” Fernandes says, because it targets a different part of the fungus. “We’re lucky it has activity against C. auris.”
Pfizer’s fosmanogepix is in Phase II clinical trials for patients with invasive fungal infections caused by multiple Candida species. Results are showing significantly better survival rates for people taking fosmanogepix.
Although C. auris does pose a serious threat to healthcare worldwide, scientists try to stay optimistic—because they recognized the problem early enough, they might have solutions in place before the perfect storm hits. “There is a bit of hope,” says Robinson. “BARDA has finally been able to fund the development of new antifungal agents and, hopefully, this year we can get several new classes of antifungals into development.”