
Coronavirus Risk Calculators: What You Need to Know
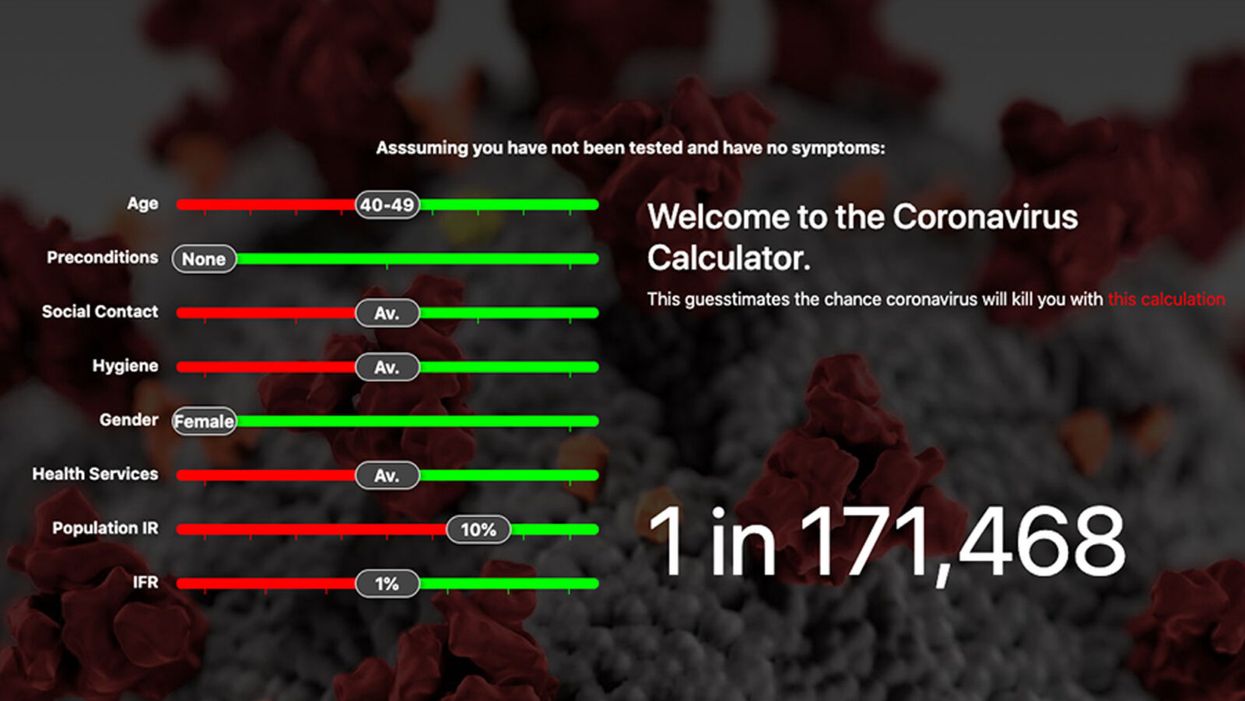
A screenshot of one coronavirus risk calculator.
People in my family seem to develop every ailment in the world, including feline distemper and Dutch elm disease, so I naturally put fingers to keyboard when I discovered that COVID-19 risk calculators now exist.
"It's best to look at your risk band. This will give you a more useful insight into your personal risk."
But the results – based on my answers to questions -- are bewildering.
A British risk calculator developed by the Nexoid software company declared I have a 5 percent, or 1 in 20, chance of developing COVID-19 and less than 1 percent risk of dying if I get it. Um, great, I think? Meanwhile, 19 and Me, a risk calculator created by data scientists, says my risk of infection is 0.01 percent per week, or 1 in 10,000, and it gave me a risk score of 44 out of 100.
Confused? Join the club. But it's actually possible to interpret numbers like these and put them to use. Here are five tips about using coronavirus risk calculators:
1. Make Sure the Calculator Is Designed For You
Not every COVID-19 risk calculator is designed to be used by the general public. Cleveland Clinic's risk calculator, for example, is only a tool for medical professionals, not sick people or the "worried well," said Dr. Lara Jehi, Cleveland Clinic's chief research information officer.
Unfortunately, the risk calculator's web page fails to explicitly identify its target audience. But there are hints that it's not for lay people such as its references to "platelets" and "chlorides."
The 19 and Me or the Nexoid risk calculators, in contrast, are both designed for use by everyone, as is a risk calculator developed by Emory University.
2. Take a Look at the Calculator's Privacy Policy
COVID-19 risk calculators ask for a lot of personal information. The Nexoid calculator, for example, wanted to know my age, weight, drug and alcohol history, pre-existing conditions, blood type and more. It even asked me about the prescription drugs I take.
It's wise to check the privacy policy and be cautious about providing an email address or other personal information. Nexoid's policy says it provides the information it gathers to researchers but it doesn't release IP addresses, which can reveal your location in certain circumstances.
John-Arne Skolbekken, a professor and risk specialist at Norwegian University of Science and Technology, entered his own data in the Nexoid calculator after being contacted by LeapsMag for comment. He noted that the calculator, among other things, asks for information about use of recreational drugs that could be illegal in some places. "I have given away some of my personal data to a company that I can hope will not misuse them," he said. "Let's hope they are trustworthy."
The 19 and Me calculator, by contrast, doesn't gather any data from users, said Cindy Hu, data scientist at Mathematica, which created it. "As soon as the window is closed, that data is gone and not captured."
The Emory University risk calculator, meanwhile, has a long privacy policy that states "the information we collect during your assessment will not be correlated with contact information if you provide it." However, it says personal information can be shared with third parties.
3. Keep an Eye on Time Horizons
Let's say a risk calculator says you have a 1 percent risk of infection. That's fairly low if we're talking about this year as a whole, but it's quite worrisome if the risk percentage refers to today and jumps by 1 percent each day going forward. That's why it's helpful to know exactly what the numbers mean in terms of time.
Unfortunately, this information isn't always readily available. You may have to dig around for it or contact a risk calculator's developers for more information. The 19 and Me calculator's risk percentages refer to this current week based on your behavior this week, Hu said. The Nexoid calculator, by contrast, has an "infinite timeline" that assumes no vaccine is developed, said Jonathon Grantham, the company's managing director. But your results will vary over time since the calculator's developers adjust it to reflect new data.
When you use a risk calculator, focus on this question: "How does your risk compare to the risk of an 'average' person?"
4. Focus on the Big Picture
The Nexoid calculator gave me numbers of 5 percent (getting COVID-19) and 99.309 percent (surviving it). It even provided betting odds for gambling types: The odds are in favor of me not getting infected (19-to-1) and not dying if I get infected (144-to-1).
However, Grantham told me that these numbers "are not the whole story." Instead, he said, "it's best to look at your risk band. This will give you a more useful insight into your personal risk." Risk bands refer to a segmentation of people into five categories, from lowest to highest risk, according to how a person's result sits relative to the whole dataset.
The Nexoid calculator says I'm in the "lowest risk band" for getting COVID-19, and a "high risk band" for dying of it if I get it. That suggests I'd better stay in the lowest-risk category because my pre-existing risk factors could spell trouble for my survival if I get infected.
Michael J. Pencina, a professor and biostatistician at Duke University School of Medicine, agreed that focusing on your general risk level is better than focusing on numbers. When you use a risk calculator, he said, focus on this question: "How does your risk compare to the risk of an 'average' person?"
The 19 and Me calculator, meanwhile, put my risk at 44 out of 100. Hu said that a score of 50 represents the typical person's risk of developing serious consequences from another disease – the flu.
5. Remember to Take Action
Hu, who helped develop the 19 and Me risk calculator, said it's best to use it to "understand the relative impact of different behaviors." As she noted, the calculator is designed to allow users to plug in different answers about their behavior and immediately see how their risk levels change.
This information can help us figure out if we should change the way we approach the world by, say, washing our hands more or avoiding more personal encounters.
"Estimation of risk is only one part of prevention," Pencina said. "The other is risk factors and our ability to reduce them." In other words, odds, percentages and risk bands can be revealing, but it's what we do to change them that matters.

Leaders at Google and other companies are trying to get workers to return to the office, saying remote and hybrid work disrupt work-life boundaries and well-being. These arguments conflict with research on remote work and wellness.
Many leaders at top companies are trying to get workers to return to the office. They say remote and hybrid work are bad for their employees’ mental well-being and lead to a sense of social isolation, meaninglessness, and lack of work-life boundaries, so we should just all go back to office-centric work.
One example is Google, where the company’s leadership is defending its requirement of mostly in-office work for all staff as necessary to protect social capital, meaning people’s connections to and trust in one another. That’s despite a survey of over 1,000 Google employees showing that two-thirds feel unhappy about being forced to work in the office three days per week. In internal meetings and public letters, many have threatened to leave, and some are already quitting to go to other companies with more flexible options.
Last month, GM rolled out a policy similar to Google’s, but had to backtrack because of intense employee opposition. The same is happening in some places outside of the U.S. For instance, three-fifths of all Chinese employers are refusing to offer permanent remote work options, according to a survey this year from The Paper.
For their claims that remote work hurts well-being, some of these office-centric traditionalists cite a number of prominent articles. For example, Arthur Brooks claimed in an essay that “aggravation from commuting is no match for the misery of loneliness, which can lead to depression, substance abuse, sedentary behavior, and relationship damage, among other ills.” An article in Forbes reported that over two-thirds of employees who work from home at least part of the time had trouble getting away from work at the end of the day. And Fast Company has a piece about how remote work can “exacerbate existing mental health issues” like depression and anxiety.
For his part, author Malcolm Gladwell has also championed a swift return to the office, saying there is a “core psychological truth, which is we want you to have a feeling of belonging and to feel necessary…I know it’s a hassle to come into the office, but if you’re just sitting in your pajamas in your bedroom, is that the work life you want to live?”
These arguments may sound logical to some, but they fly in the face of research and my own experience as a behavioral scientist and as a consultant to Fortune 500 companies. In these roles, I have seen the pitfalls of in-person work, which can be just as problematic, if not more so. Remote work is not without its own challenges, but I have helped 21 companies implement a series of simple steps to address them.
Research finds that remote work is actually better for you
The trouble with the articles described above - and claims by traditionalist business leaders and gurus - stems from a sneaky misdirection. They decry the negative impact of remote and hybrid work for wellbeing. Yet they gloss over the damage to wellbeing caused by the alternative, namely office-centric work.
It’s like comparing remote and hybrid work to a state of leisure. Sure, people would feel less isolated if they could hang out and have a beer with their friends instead of working. They could take care of their existing mental health issues if they could visit a therapist. But that’s not in the cards. What’s in the cards is office-centric work. That means the frustration of a long commute to the office, sitting at your desk in an often-uncomfortable and oppressive open office for at least 8 hours, having a sad desk lunch and unhealthy snacks, sometimes at an insanely expensive cost and, for making it through this series of insults, you’re rewarded with more frustration while commuting back home.
In a 2022 survey, the vast majority of respondents felt that working remotely improved their work-life balance. Much of that improvement stemmed from saving time due to not needing to commute and having a more flexible schedule.
So what happens when we compare apples to apples? That’s when we need to hear from the horse’s mouth: namely, surveys of employees themselves, who experienced both in-office work before the pandemic, and hybrid and remote work after COVID struck.
Consider a 2022 survey by Cisco of 28,000 full-time employees around the globe. Nearly 80 percent of respondents say that remote and hybrid work improved their overall well-being: that applies to 83 percent of Millennials, 82 percent of Gen Z, 76 percent of Gen Z, and 66 percent of Baby Boomers. The vast majority of respondents felt that working remotely improved their work-life balance.
Much of that improvement stemmed from saving time due to not needing to commute and having a more flexible schedule: 90 percent saved 4 to 8 hours or more per week. What did they do with that extra time? The top choice for almost half was spending more time with family, friends and pets, which certainly helped address the problem of isolation from the workplace. Indeed, three-quarters of them report that working from home improved their family relationships, and 51 percent strengthened their friendships. Twenty percent used the freed up hours for self-care.
Of the small number who report their work-life balance has not improved or even worsened, the number one reason is the difficulty of disconnecting from work, but 82 percent report that working from anywhere has made them happier. Over half say that remote work decreased their stress levels.
Other surveys back up Cisco’s findings. For example, a 2022 Future Forum survey compared knowledge workers who worked full-time in the office, in a hybrid modality, and fully remote. It found that full-time in-office workers felt the least satisfied with work-life balance, hybrid workers were in the middle, and fully remote workers felt most satisfied. The same distribution applied to questions about stress and anxiety. A mental health website called Tracking Happiness found in a 2022 survey of over 12,000 workers that fully remote employees report a happiness level about 20 percent greater than office-centric ones. Another survey by CNBC in June found that fully remote workers are more often very satisfied with their jobs than workers who are fully in-person.
Academic peer-reviewed research provides further support. Consider a 2022 study published in the International Journal of Environmental Research and Public Health of bank workers who worked on the same tasks of advising customers either remotely or in-person. It found that fully remote workers experienced higher meaningfulness, self-actualization, happiness, and commitment than in-person workers. Another study, published by the National Bureau of Economic Research, reported that hybrid workers, compared to office-centric ones, experienced higher satisfaction with work and had 35 percent more job retention.
What about the supposed burnout crisis associated with remote work? Indeed, burnout is a concern. A survey by Deloitte finds that 77 percent of workers experienced burnout at their current job. Gallup came up with a slightly lower number of 67 percent in its survey. But guess what? Both of those surveys are from 2018, long before the era of widespread remote work.
By contrast, in a Gallup survey in late 2021, 58 percent of respondents reported less burnout. An April 2021 McKinsey survey found burnout in 54 percent of Americans and 49 percent globally. A September 2021 survey by The Hartford reported 61 percent burnout. Arguably, the increase in full or part-time remote opportunities during the pandemic helped to address feelings of burnout, rather than increasing them. Indeed, that finding aligns with the earlier surveys and peer-reviewed research suggesting remote and hybrid work improves wellbeing.
Remote work isn’t perfect – here’s how to fix its shortcomings
Still, burnout is a real problem for hybrid and remote workers, as it is for in-office workers. Employers need to offer mental health benefits with online options to help employees address these challenges, regardless of where they’re working.
Moreover, while they’re better overall for wellbeing, remote and hybrid work arrangements do have specific disadvantages around work-life separation. To address work-life issues, I advise my clients who I helped make the transition to hybrid and remote work to establish norms and policies that focus on clear expectations and setting boundaries.
For working at home and collaborating with others, there’s sometimes an unhealthy expectation that once you start your workday in your home office chair, and that you’ll work continuously while sitting there.
Some people expect their Slack or Microsoft Teams messages to be answered within an hour, while others check Slack once a day. Some believe email requires a response within three hours, and others feel three days is fine. As a result of such uncertainty and lack of clarity about what’s appropriate, too many people feel uncomfortable disconnecting and not replying to messages or doing work tasks after hours. That might stem from a fear of not meeting their boss’s expectations or not wanting to let their colleagues down.
To solve this problem, companies need to establish and incentivize clear expectations and boundaries. They should develop policies and norms around response times for different channels of communication. They also need to clarify work-life boundaries – for example, the frequency and types of unusual circumstances that will require employees to work outside of regular hours.
Moreover, for working at home and collaborating with others, there’s sometimes an unhealthy expectation that once you start your workday in your home office chair, and that you’ll work continuously while sitting there (except for your lunch break). That’s not how things work in the office, which has physical and mental breaks built in throughout the day. You took 5-10 minutes to walk from one meeting to another, or you went to get your copies from the printer and chatted with a coworker on the way.
Those and similar physical and mental breaks, research shows, decrease burnout, improve productivity, and reduce mistakes. That’s why companies should strongly encourage employees to take at least a 10-minute break every hour during remote work. At least half of those breaks should involve physical activity, such as stretching or walking around, to counteract the dangerous effects of prolonged sitting. Other breaks should be restorative mental activities, such as meditation, brief naps, walking outdoors, or whatever else feels restorative to you.
To facilitate such breaks, my client organizations such as the University of Southern California’s Information Sciences Institute shortened hour-long meetings to 50 minutes and half-hour meetings to 25 minutes, to give everyone – both in-person and remote workers – a mental and physical break and transition time.
Very few people will be reluctant to have shorter meetings. After that works out, move to other aspects of setting boundaries and expectations. Doing so will require helping team members get on the same page and reduce conflicts and tensions. By setting clear expectations, you’ll address the biggest challenge for wellbeing for remote and hybrid work: establishing clear work-life boundaries.

A company has slashed the cost of assessing a person's genome to just $100. With lower costs - and as other genetic tools mature and evolve - a wave of new therapies could be coming in the near future.
In May 2022, Californian biotech Ultima Genomics announced that its UG 100 platform was capable of sequencing an entire human genome for just $100, a landmark moment in the history of the field. The announcement was particularly remarkable because few had previously heard of the company, a relative unknown in an industry long dominated by global giant Illumina which controls about 80 percent of the world’s sequencing market.
Ultima’s secret was to completely revamp many technical aspects of the way Illumina have traditionally deciphered DNA. The process usually involves first splitting the double helix DNA structure into single strands, then breaking these strands into short fragments which are laid out on a glass surface called a flow cell. When this flow cell is loaded into the sequencing machine, color-coded tags are attached to each individual base letter. A laser scans the bases individually while a camera simultaneously records the color associated with them, a process which is repeated until every single fragment has been sequenced.
Instead, Ultima has found a series of shortcuts to slash the cost and boost efficiency. “Ultima Genomics has developed a fundamentally new sequencing architecture designed to scale beyond conventional approaches,” says Josh Lauer, Ultima’s chief commercial officer.
This ‘new architecture’ is a series of subtle but highly impactful tweaks to the sequencing process ranging from replacing the costly flow cell with a silicon wafer which is both cheaper and allows more DNA to be read at once, to utilizing machine learning to convert optical data into usable information.
To put $100 genome in perspective, back in 2012 the cost of sequencing a single genome was around $10,000, a price tag which dropped to $1,000 a few years later. Before Ultima’s announcement, the cost of sequencing an individual genome was around $600.
Several studies have found that nearly 12 percent of healthy people who have their genome sequenced, then discover they have a variant pointing to a heightened risk of developing a disease that can be monitored, treated or prevented.
While Ultima’s new machine is not widely available yet, Illumina’s response has been rapid. Last month the company unveiled the NovaSeq X series, which it describes as its fastest most cost-efficient sequencing platform yet, capable of sequencing genomes at $200, with further price cuts likely to follow.
But what will the rapidly tumbling cost of sequencing actually mean for medicine? “Well to start with, obviously it’s going to mean more people getting their genome sequenced,” says Michael Snyder, professor of genetics at Stanford University. “It'll be a lot more accessible to people.”
At the moment sequencing is mainly limited to certain cancer patients where it is used to inform treatment options, and individuals with undiagnosed illnesses. In the past, initiatives such as SeqFirst have attempted further widen access to genome sequencing based on growing amounts of research illustrating the potential benefits of the technology in healthcare. Several studies have found that nearly 12 percent of healthy people who have their genome sequenced, then discover they have a variant pointing to a heightened risk of developing a disease that can be monitored, treated or prevented.
“While whole genome sequencing is not yet widely used in the U.S., it has started to come into pediatric critical care settings such as newborn intensive care units,” says Professor Michael Bamshad, who heads the genetic medicine division in the University of Washington’s pediatrics department. “It is also being used more often in outpatient clinical genetics services, particularly when conventional testing fails to identify explanatory variants.”
But the cost of sequencing itself is only one part of the price tag. The subsequent clinical interpretation and genetic counselling services often come to several thousand dollars, a cost which insurers are not always willing to pay.
As a result, while Bamshad and others hope that the arrival of the $100 genome will create new opportunities to use genetic testing in innovative ways, the most immediate benefits are likely to come in the realm of research.
Bigger Data
There are numerous ways in which cheaper sequencing is likely to advance scientific research, for example the ability to collect data on much larger patient groups. This will be a major boon to scientists working on complex heterogeneous diseases such as schizophrenia or depression where there are many genes involved which all exert subtle effects, as well as substantial variance across the patient population. Bigger studies could help scientists identify subgroups of patients where the disease appears to be driven by similar gene variants, who can then be more precisely targeted with specific drugs.
If insurers can figure out the economics, Snyder even foresees a future where at a certain age, all of us can qualify for annual sequencing of our blood cells to search for early signs of cancer or the potential onset of other diseases like type 2 diabetes.
David Curtis, a genetics professor at University College London, says that scientists studying these illnesses have previously been forced to rely on genome-wide association studies which are limited because they only identify common gene variants. “We might see a significant increase in the number of large association studies using sequence data,” he says. “It would be far preferable to use this because it provides information about rare, potentially functional variants.”
Cheaper sequencing will also aid researchers working on diseases which have traditionally been underfunded. Bamshad cites cystic fibrosis, a condition which affects around 40,000 children and adults in the U.S., as one particularly pertinent example.
“Funds for gene discovery for rare diseases are very limited,” he says. “We’re one of three sites that did whole genome sequencing on 5,500 people with cystic fibrosis, but our statistical power is limited. A $100 genome would make it much more feasible to sequence everyone in the U.S. with cystic fibrosis and make it more likely that we discover novel risk factors and pathways influencing clinical outcomes.”
For progressive diseases that are more common like cancer and type 2 diabetes, as well as neurodegenerative conditions like multiple sclerosis and ALS, geneticists will be able to go even further and afford to sequence individual tumor cells or neurons at different time points. This will enable them to analyze how individual DNA modifications like methylation, change as the disease develops.
In the case of cancer, this could help scientists understand how tumors evolve to evade treatments. Within in a clinical setting, the ability to sequence not just one, but many different cells across a patient’s tumor could point to the combination of treatments which offer the best chance of eradicating the entire cancer.
“What happens at the moment with a solid tumor is you treat with one drug, and maybe 80 percent of that tumor is susceptible to that drug,” says Neil Ward, vice president and general manager in the EMEA region for genomics company PacBio. “But the other 20 percent of the tumor has already got mutations that make it resistant, which is probably why a lot of modern therapies extend life for sadly only a matter of months rather than curing, because they treat a big percentage of the tumor, but not the whole thing. So going forwards, I think that we will see genomics play a huge role in cancer treatments, through using multiple modalities to treat someone's cancer.”
If insurers can figure out the economics, Snyder even foresees a future where at a certain age, all of us can qualify for annual sequencing of our blood cells to search for early signs of cancer or the potential onset of other diseases like type 2 diabetes.
“There are companies already working on looking for cancer signatures in methylated DNA,” he says. “If it was determined that you had early stage cancer, pre-symptomatically, that could then be validated with targeted MRI, followed by surgery or chemotherapy. It makes a big difference catching cancer early. If there were signs of type 2 diabetes, you could start taking steps to mitigate your glucose rise, and possibly prevent it or at least delay the onset.”
This would already revolutionize the way we seek to prevent a whole range of illnesses, but others feel that the $100 genome could also usher in even more powerful and controversial preventative medicine schemes.
Newborn screening
In the eyes of Kári Stefánsson, the Icelandic neurologist who been a visionary for so many advances in the field of human genetics over the last 25 years, the falling cost of sequencing means it will be feasible to sequence the genomes of every baby born.
“We have recently done an analysis of genomes in Iceland and the UK Biobank, and in 4 percent of people you find mutations that lead to serious disease, that can be prevented or dealt with,” says Stefansson, CEO of deCODE genetics, a subsidiary of the pharmaceutical company Amgen. “This could transform our healthcare systems.”
As well as identifying newborns with rare diseases, this kind of genomic information could be used to compute a person’s risk score for developing chronic illnesses later in life. If for example, they have a higher than average risk of colon or breast cancer, they could be pre-emptively scheduled for annual colonoscopies or mammograms as soon as they hit adulthood.
To a limited extent, this is already happening. In the UK, Genomics England has launched the Newborn Genomes Programme, which plans to undertake whole-genome sequencing of up to 200,000 newborn babies, with the aim of enabling the early identification of rare genetic diseases.
"I have not had my own genome sequenced and I would not have wanted my parents to have agreed to this," Curtis says. "I don’t see that sequencing children for the sake of some vague, ill-defined benefits could ever be justifiable.”
However, some scientists feel that it is tricky to justify sequencing the genomes of apparently healthy babies, given the data privacy issues involved. They point out that we still know too little about the links which can be drawn between genetic information at birth, and risk of chronic illness later in life.
“I think there are very difficult ethical issues involved in sequencing children if there are no clear and immediate clinical benefits,” says Curtis. “They cannot consent to this process. I have not had my own genome sequenced and I would not have wanted my parents to have agreed to this. I don’t see that sequencing children for the sake of some vague, ill-defined benefits could ever be justifiable.”
Curtis points out that there are many inherent risks about this data being available. It may fall into the hands of insurance companies, and it could even be used by governments for surveillance purposes.
“Genetic sequence data is very useful indeed for forensic purposes. Its full potential has yet to be realized but identifying rare variants could provide a quick and easy way to find relatives of a perpetrator,” he says. “If large numbers of people had been sequenced in a healthcare system then it could be difficult for a future government to resist the temptation to use this as a resource to investigate serious crimes.”
While sequencing becoming more widely available will present difficult ethical and moral challenges, it will offer many benefits for society as a whole. Cheaper sequencing will help boost the diversity of genomic datasets which have traditionally been skewed towards individuals of white, European descent, meaning that much of the actionable medical information which has come out of these studies is not relevant to people of other ethnicities.
Ward predicts that in the coming years, the growing amount of genetic information will ultimately change the outcomes for many with rare, previously incurable illnesses.
“If you're the parent of a child that has a susceptible or a suspected rare genetic disease, their genome will get sequenced, and while sadly that doesn’t always lead to treatments, it’s building up a knowledge base so companies can spring up and target that niche of a disease,” he says. “As a result there’s a whole tidal wave of new therapies that are going to come to market over the next five years, as the genetic tools we have, mature and evolve.”