
Coronavirus Risk Calculators: What You Need to Know
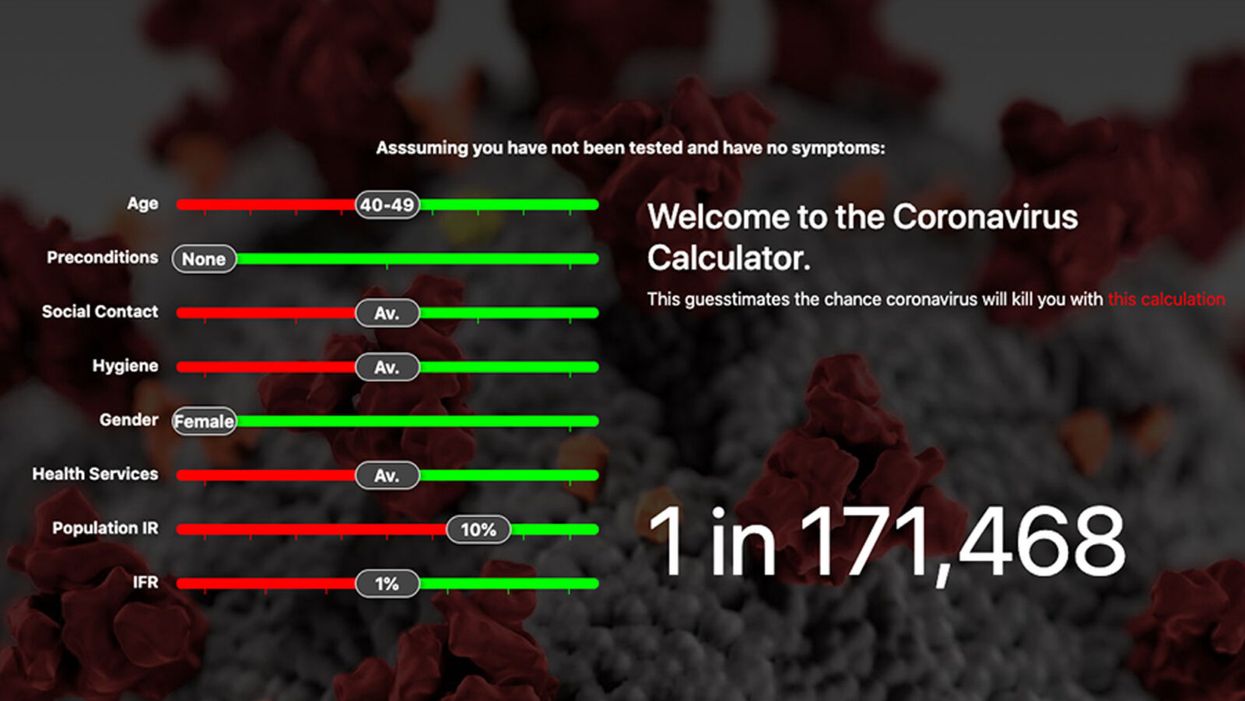
A screenshot of one coronavirus risk calculator.
People in my family seem to develop every ailment in the world, including feline distemper and Dutch elm disease, so I naturally put fingers to keyboard when I discovered that COVID-19 risk calculators now exist.
"It's best to look at your risk band. This will give you a more useful insight into your personal risk."
But the results – based on my answers to questions -- are bewildering.
A British risk calculator developed by the Nexoid software company declared I have a 5 percent, or 1 in 20, chance of developing COVID-19 and less than 1 percent risk of dying if I get it. Um, great, I think? Meanwhile, 19 and Me, a risk calculator created by data scientists, says my risk of infection is 0.01 percent per week, or 1 in 10,000, and it gave me a risk score of 44 out of 100.
Confused? Join the club. But it's actually possible to interpret numbers like these and put them to use. Here are five tips about using coronavirus risk calculators:
1. Make Sure the Calculator Is Designed For You
Not every COVID-19 risk calculator is designed to be used by the general public. Cleveland Clinic's risk calculator, for example, is only a tool for medical professionals, not sick people or the "worried well," said Dr. Lara Jehi, Cleveland Clinic's chief research information officer.
Unfortunately, the risk calculator's web page fails to explicitly identify its target audience. But there are hints that it's not for lay people such as its references to "platelets" and "chlorides."
The 19 and Me or the Nexoid risk calculators, in contrast, are both designed for use by everyone, as is a risk calculator developed by Emory University.
2. Take a Look at the Calculator's Privacy Policy
COVID-19 risk calculators ask for a lot of personal information. The Nexoid calculator, for example, wanted to know my age, weight, drug and alcohol history, pre-existing conditions, blood type and more. It even asked me about the prescription drugs I take.
It's wise to check the privacy policy and be cautious about providing an email address or other personal information. Nexoid's policy says it provides the information it gathers to researchers but it doesn't release IP addresses, which can reveal your location in certain circumstances.
John-Arne Skolbekken, a professor and risk specialist at Norwegian University of Science and Technology, entered his own data in the Nexoid calculator after being contacted by LeapsMag for comment. He noted that the calculator, among other things, asks for information about use of recreational drugs that could be illegal in some places. "I have given away some of my personal data to a company that I can hope will not misuse them," he said. "Let's hope they are trustworthy."
The 19 and Me calculator, by contrast, doesn't gather any data from users, said Cindy Hu, data scientist at Mathematica, which created it. "As soon as the window is closed, that data is gone and not captured."
The Emory University risk calculator, meanwhile, has a long privacy policy that states "the information we collect during your assessment will not be correlated with contact information if you provide it." However, it says personal information can be shared with third parties.
3. Keep an Eye on Time Horizons
Let's say a risk calculator says you have a 1 percent risk of infection. That's fairly low if we're talking about this year as a whole, but it's quite worrisome if the risk percentage refers to today and jumps by 1 percent each day going forward. That's why it's helpful to know exactly what the numbers mean in terms of time.
Unfortunately, this information isn't always readily available. You may have to dig around for it or contact a risk calculator's developers for more information. The 19 and Me calculator's risk percentages refer to this current week based on your behavior this week, Hu said. The Nexoid calculator, by contrast, has an "infinite timeline" that assumes no vaccine is developed, said Jonathon Grantham, the company's managing director. But your results will vary over time since the calculator's developers adjust it to reflect new data.
When you use a risk calculator, focus on this question: "How does your risk compare to the risk of an 'average' person?"
4. Focus on the Big Picture
The Nexoid calculator gave me numbers of 5 percent (getting COVID-19) and 99.309 percent (surviving it). It even provided betting odds for gambling types: The odds are in favor of me not getting infected (19-to-1) and not dying if I get infected (144-to-1).
However, Grantham told me that these numbers "are not the whole story." Instead, he said, "it's best to look at your risk band. This will give you a more useful insight into your personal risk." Risk bands refer to a segmentation of people into five categories, from lowest to highest risk, according to how a person's result sits relative to the whole dataset.
The Nexoid calculator says I'm in the "lowest risk band" for getting COVID-19, and a "high risk band" for dying of it if I get it. That suggests I'd better stay in the lowest-risk category because my pre-existing risk factors could spell trouble for my survival if I get infected.
Michael J. Pencina, a professor and biostatistician at Duke University School of Medicine, agreed that focusing on your general risk level is better than focusing on numbers. When you use a risk calculator, he said, focus on this question: "How does your risk compare to the risk of an 'average' person?"
The 19 and Me calculator, meanwhile, put my risk at 44 out of 100. Hu said that a score of 50 represents the typical person's risk of developing serious consequences from another disease – the flu.
5. Remember to Take Action
Hu, who helped develop the 19 and Me risk calculator, said it's best to use it to "understand the relative impact of different behaviors." As she noted, the calculator is designed to allow users to plug in different answers about their behavior and immediately see how their risk levels change.
This information can help us figure out if we should change the way we approach the world by, say, washing our hands more or avoiding more personal encounters.
"Estimation of risk is only one part of prevention," Pencina said. "The other is risk factors and our ability to reduce them." In other words, odds, percentages and risk bands can be revealing, but it's what we do to change them that matters.
Friday Five Podcast: New drug may slow the rate of Alzheimer's disease

On September 27, pharmaceuticals Biogen and Eisai announced that their drug, lecanemab, can slow the rate of Alzheimer's disease, according to a clinical trial. Today's Friday Five episode covers this story and other health research over the month of September.
The Friday Five covers important stories in health and science research that you may have missed - usually over the previous week, but today's episode is a lookback on important studies over the month of September.
Most recently, on September 27, pharmaceuticals Biogen and Eisai announced that a clinical trial showed their drug, lecanemab, can slow the rate of Alzheimer's disease. There are plenty of controversies and troubling ethical issues in science – and we get into many of them in our online magazine – but this news roundup focuses on scientific creativity and progress to give you a therapeutic dose of inspiration headed into the weekend and the new month.
Listen on Apple | Listen on Spotify | Listen on Stitcher | Listen on Amazon | Listen on Google
This Friday Five episode covers the following studies published and announced over the past month:
- A new drug is shown to slow the rate of Alzheimer's disease
- The need for speed if you want to reduce your risk of dementia
- How to refreeze the north and south poles
- Ancient wisdom about Neti pots could pay off for Covid
- Two women, one man and a baby
Could epigenetic reprogramming reverse aging?

A range of strategies are being explored to reprogram the body's cells to an earlier state. Most scientists aren't betting on a new fountain of youth just yet - but, in theory, epigenetic reprogramming is a recipe for self-renewal.
Ten thousand years ago, the average human spent a maximum of 30 years on Earth. Despite the glory of Ancient Greece and the Roman Empire, most of their inhabitants didn’t surpass the age of 35. Between the 1500s and 1800, life expectancy (at least in Europe) fluctuated between 30 and 40 years.
Public health advancements like control of infectious diseases, better diet and clean sanitation, as well as social improvements have made it possible for human lifespans to double since 1800. Although lifespan differs widely today from country to country according to socioeconomic health, the average has soared to 73.2 years.
But this may turn out to be on the low side if epigenetic rejuvenation fulfills its great promise: to reverse aging, perhaps even completely. Epigenetic rejuvenation, or partial reprogramming, is the process by which a set of therapies are trying to manipulate epigenetics – how various changes can affect our genes – and the Yamanaka factors. These Yamanaka factors are a group of proteins that can convert any cell of the body into pluripotent stem cells, a group of cells that can turn into brand new cells, such as those of the brain or skin. At least in theory, it could be a recipe for self-renewal.
“Partial reprogramming tries to knock a few years off of people’s biological age, while preserving their original cell identity and function,” says Yuri Deigin, cofounder and director of YouthBio Therapeutics, a longevity startup utilizing partial reprogramming to develop gene therapies aimed at the renewal of epigenetic profiles. YouthBio plans to experiment with injecting these gene therapies into target organs. Once the cargo is delivered, a specific small molecule will trigger gene expression and rejuvenate those organs.
“Our ultimate mission is to find the minimal number of tissues we would need to target to achieve significant systemic rejuvenation,” Deigin says. Initially, YouthBio will apply these therapies to treat age-related conditions. Down the road, though, their goal is for everyone to get younger. “We want to use them for prophylaxis, which is rejuvenation that would lower disease risk,” Deigin says.
Epigenetics has swept the realm of biology off its feet over the last decade. We now know that we can switch genes on and off by tweaking the chemical status quo of the DNA’s local environment. "Epigenetics is a fascinating and important phenomenon in biology,’’ says Henry Greely, a bioethicist at Stanford Law School. Greely is quick to stress that this kind of modulation (turning genes on and off and not the entire DNA) happens all the time. “When you eat and your blood sugar goes up, the gene in the beta cells of your pancreas that makes insulin is turned on or up. Almost all medications are going to have effects on epigenetics, but so will things like exercise, food, and sunshine.”
Can intentional control over epigenetic mechanisms lead to novel and useful therapies? “It is a very plausible scenario,” Greely says, though a great deal of basic research into epigenetics is required before it becomes a well-trodden way to stay healthy or treat disease. Whether these therapies could cause older cells to become younger in ways that have observable effects is “far from clear,” he says. “Historically, betting on someone’s new ‘fountain of youth’ has been a losing strategy.”
The road to de-differentiation, the process by which cells return to an earlier state, is not paved with roses; de-differentiate too much and you may cause pathology and even death.
In 2003 researchers finished sequencing the roughly 3 billion letters of DNA that make up the human genome. The human genome sequencing was hailed as a vast step ahead in our understanding of how genetics contribute to diseases like cancer or to developmental disorders. But for Josephine Johnston, director of research and research scholar at the Hastings Center, the hype has not lived up to its initial promise. “Other than some quite effective tests to diagnose certain genetic conditions, there isn't a radical intervention that reverses things yet,” Johnston says. For her, this is a testament to the complexity of biology or at least to our tendency to keep underestimating it. And when it comes to epigenetics specifically, Johnston believes there are some hard questions we need to answer before we can safely administer relevant therapies to the population.
“You'd need to do longitudinal studies. You can't do a study and look at someone and say they’re safe only six months later,” Johnston says. You can’t know long-term side effects this way, and how will companies position their therapies on the market? Are we talking about interventions that target health problems, or life enhancements? “If you describe something as a medical intervention, it is more likely to be socially acceptable, to attract funding from governments and ensure medical insurance, and to become a legitimate part of medicine,” she says.
Johnston’s greatest concerns are of the philosophical and ethical nature. If we’re able to use epigenetic reprogramming to double the human lifespan, how much of the planet’s resources will we take up during this long journey? She believes we have a moral obligation to make room for future generations. “We should also be honest about who's actually going to afford such interventions; they would be extraordinarily expensive and only available to certain people, and those are the people who would get to live longer, healthier lives, and the rest of us wouldn't.”
That said, Johnston agrees there is a place for epigenetic reprogramming. It could help people with diseases that are caused by epigenetic problems such as Fragile X syndrome, Prader-Willi syndrome and various cancers.
Zinaida Good, a postdoctoral fellow at Stanford Cancer Institute, says these problems are still far in the future. Any change will be incremental. “Thinking realistically, there’s not going to be a very large increase in lifespan anytime soon,” she says. “I would not expect something completely drastic to be invented in the next 5 to 10 years. ”
Good won’t get any such treatment for herself until it’s shown to be effective and safe. Nature has programmed our bodies to resist hacking, she says, in ways that could undermine any initial benefits to longevity. A preprint that is not yet peer-reviewed reports cellular reprogramming may lead to premature death due to liver and intestinal problems, and using the Yamanaka factors may have the potential to cause cancer, at least in animal studies.
“Side effects are an open research question that all partial reprogramming companies and labs are trying to address,” says Deigin. The road to de-differentiation, the process by which cells return to an earlier state, is not paved with roses; de-differentiate too much and you may cause pathology and even death. Deigin is exploring other, less risky approaches. “One way is to look for novel factors tailored toward rejuvenation rather than de-differentiation.” Unlike Yamanaka factors, such novel factors would never involve taking a given cell to a state in which it could turn cancerous, according to Deigin.
An example of a novel factor that could lower the risk of cancer is artificially introducing mRNA molecules, or molecules carrying the genetic information necessary to make proteins, by using electricity to penetrate the cell instead of a virus. There is also chemical-based reprogramming, in which chemicals are applied to convert regular cells into pluripotent cells. This approach is currently effective only for mice though.
“The search for novel factors tailored toward rejuvenation without de-differentiation is an ongoing research and development effort by several longevity companies, including ours,” says Deigin.
He isn't disclosing the details of his own company’s underlying approach to lowering the risk, but he’s hopeful that something will eventually end up working in humans. Yet another challenge is that, partly because of the uncertainties, the FDA hasn’t seen fit to approve a single longevity therapy. But with the longevity market projected to soar to $600 billion by 2025, Deigin says naysayers are clinging irrationally to the status quo. “Thankfully, scientific progress is moved forward by those who bet for something while disregarding the skeptics - who, in the end, are usually proven wrong.”