

Hyperbaric oxygen therapy has been used in the past to help people with traumatic brain injury, stroke and other conditions involving wounds to the brain. Now, researchers at Shamir Medical Center in Tel Aviv are studying how it could treat Long Covid.
Long COVID is not a single disease, it is a syndrome or cluster of symptoms that can arise from exposure to SARS-CoV-2, a virus that affects an unusually large number of different tissue types. That's because the ACE2 receptor it uses to enter cells is common throughout the body, and inflammation from the immune response fighting that infection can damage surrounding tissue.
One of the most widely shared groups of symptoms is fatigue and what has come to be called “brain fog,” a difficulty focusing and an amorphous feeling of slowed mental functioning and capacity. Researchers have tied these COVID-related symptoms to tissue damage in specific sections of the brain and actual shrinkage in its size.
When Shai Efrati, medical director of the Sagol Center for Hyperbaric Medicine and Research in Tel Aviv, first looked at functional magnetic resonance images (fMRIs) of patients with what is now called long COVID, he saw “micro infarcts along the brain.” It reminded him of similar lesions in other conditions he had treated with hyperbaric oxygen therapy (HBOT). “Once we saw that, we said, this is the type of wound we can treat. It doesn't matter if the primary cause is mechanical injury like TBI [traumatic brain injury] or stroke … we know how to oxidize them.”Efrati came to HBOT almost by accident. The physician had seen how it had helped heal diabetic ulcers and improved the lives of other patients, but he was busy with his own research. Then the director of his Tel Aviv hospital threatened to shut down the small HBOT chamber unless Efrati took on administrative responsibility for it. He reluctantly agreed, a decision that shifted the entire focus of his research.
“The main difference between wounds in the leg and wounds in the brain is that one is something we can see, it's tangible, and the wound in the brain is hidden,” says Efrati. With fMRIs, he can measure how a limited supply of oxygen in blood is shuttled around to fuel activity in various parts of the brain. Years of research have mapped how specific areas of the brain control activity ranging from thinking to moving. An fMRI captures the brain area as it’s activated by supplies of oxygen; lack of activity after the same stimuli suggests damage has occurred in that tissue. Suddenly, what was hidden became visible to researchers using fMRI. It helped to make a diagnosis and measure response to treatment.
HBOT is not a single thing but rather a tool, a process or approach with variations depending on the condition being treated. It aims to increase the amount of oxygen that gets to damaged tissue and speed up healing. Regular air is about 21 percent oxygen. But inside the HBOT chamber the atmospheric pressure can be increased to up to three times normal pressure at sea level and the patient breathes pure oxygen through a mask; blood becomes saturated with much higher levels of oxygen. This can defuse through the damaged capillaries of a wound and promote healing.
The trial
Efrati’s clinical trials started in December 2020, barely a year after SARS-CoV-2 had first appeared in Israel. Patients who’d experienced cognitive issues after having COVID received 40 sessions in the chamber over a period of 60 days. In each session, they spent 90 minutes breathing through a mask at two atmospheres of pressure. While inside, they performed mental exercises to train the brain. The only difference between the two groups of patients was that one breathed pure oxygen while the other group breathed normal air. No one knew who was receiving which level of oxygen.
The results were striking. Before and after fMRIs showed significant repair of damaged tissue in the brain and functional cognition tests improved substantially among those who received pure oxygen. Importantly, 80 percent of patients said they felt back to “normal,” but Efrati says they didn't include patient evaluation in the paper because there was no baseline data to show how they functioned before COVID. After the study was completed, the placebo group was offered a new round of treatments using 100 percent oxygen, and the team saw similar results.
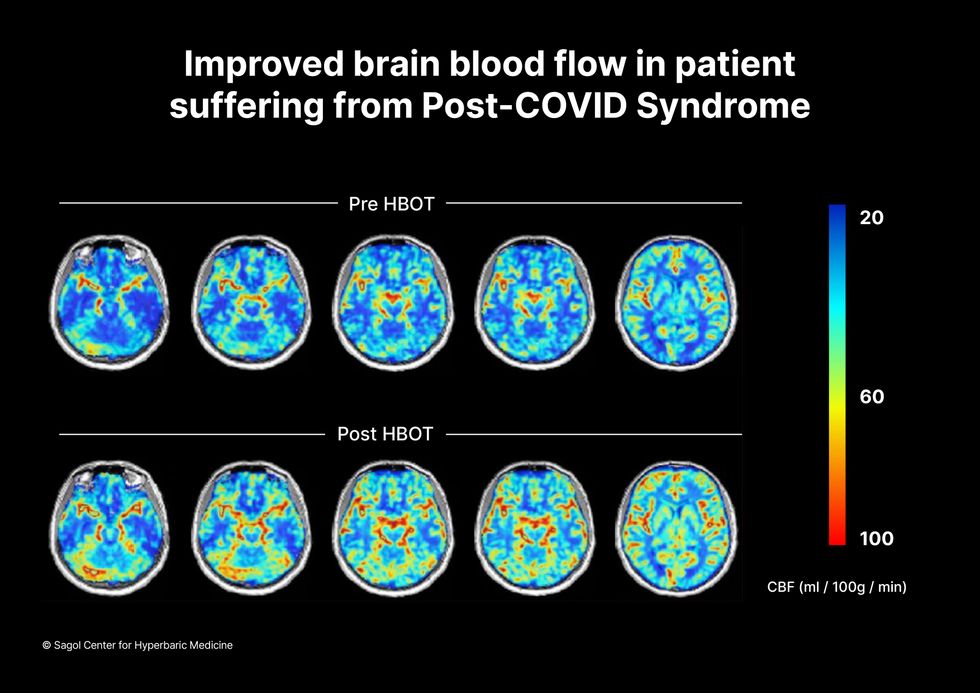
Scans show improved blood flow in a patient suffering from Long Covid.
Sagol Center for Hyperbaric Medicine
Efrati's use of HBOT is part of an emerging geroscience approach to diseases associated with aging. These researchers see systems dysfunctions that are common to several diseases, such as inflammation, which has been shown to play a role in micro infarcts, heart disease and Alzheimer’s disease. Preliminary research suggests that HBOT can retard some underlying mechanisms of aging, which might address several medical conditions. However, the drug approval process is set up to regulate individual disease, not conditions as broad as aging, and so they concentrate on treating the low hanging fruit: disorders where effective treatments currently are limited and success might be demonstrated.
The key to HBOT's effectiveness is something called the hyperoxic-hypoxic paradox where a body does not react to an increase in available oxygen, only to a decrease, regardless of the starting point. That danger signal has a powerful effect on gene expression, resulting in changes in metabolism, and the proliferation of stem cells. That occurs with each cycle of 20 minutes of pure oxygen followed by 5 minutes of regular air circulating through the masks, while the chamber remains pressurized. The high levels of oxygen in the blood provide the fuel necessary for tissue regeneration.
The hyperbaric chamber that Efrati has built can hold a dozen patients and attending medical staff. Think of it as a pressurized airplane cabin, only with much more space than even in first class. In the U.S., people think of HBOT as “a sack of air or some tube that you can buy on Amazon” or find at a health spa. “That is total bullshit,” Efrati says. “It has to be a medical class center where a physician can lose their license if they are not operating it properly.”

Shai Efrati
Alexander Charney, a research psychiatrist at the Icahn School of Medicine at Mount Sinai in New York City, calls Efrati’s study thoughtful and well designed. But it demands a lot from patients with its intense number of sessions. Those types of regimens have proven difficult to roll out to large numbers of patients. Still, the results are intriguing enough to merit additional trials.
John J. Miller, a physician and editor in chief of Psychiatric Times, has seen “many physicians that use hyperbaric oxygen for various brain disorders such as TBI.” He is intrigued by Efrati's work and believes the approach “has great potential to help patients with long COVID whose symptoms are related to brain tissue changes.”
Efrati believes so much in the power of the hyperoxic-hypoxic paradox to heal a variety of tissue injuries that he is leading the medical advisory board at Aviv Clinic, an international network of clinics that are delivering HBOT treatments based on research conducted in Israel. His goal is to silence doubters by quickly opening about 50 such clinics worldwide, based on the model of standalone dialysis clinics in the United States. Sagol Center is treating 300 patients per day, and clinics have opened in Florida and Dubai. There are plans to open another in Manhattan.

Avalanche rescue dogs train to find and dig out people buried in snow slides
By the time he is three, Lume, like Huckleberry, will be a fully trained avy pup and will join seven other avy dogs on Breckenridge ski patrol team. Some of the team members, both human and canine, are also certified to work with Colorado Rapid Avalanche Deployment, a coordinated response team that works with the Summit County Sheriff’s office for avalanche emergencies outside of the ski slopes’ boundaries.
There have been 19 avalanche deaths in the U.S. this season, according to avalanche.org, which tracks slides; eight in Colorado. During the entirety of last season there were 17. Avalanche season runs from November through June, but avalanches can occur year-round.
High tech and high stakes
Complementing avy dogs’ ability to smell people buried in a slide, avalanche detection, rescue and recovery is becoming increasingly high tech. There are transceivers, signal locators, ground scanners and drones, which are considered “games changers” by many in avalanche rescue and recovery
For a person buried in an avalanche, the chance of survival plummets after 20 minutes, so every moment counts.
A drone can provide thermal imaging of objects caught in a slide; what looks like a rock from far away might be a human with a heat signature. Transceivers, also known as beacons, send a signal from an avalanche victim to a companion. Signal locators, like RECCO reflectors which are often sewn directly into gear, can echo back a radar signal sent by a detector; most ski resorts have RECCO detector units.
Research suggests that Ground Penetrating Radar (GPR), an electromagnetic tool used by geophysicists to pull images from inside the ground, could be used to locate an avalanche victim. A new study from the Department of Energy’s Sandia National Laboratories suggests that a computer program developed to pinpoint the source of a chemical or biological terrorist attack could also be used to find someone submerged in an avalanche. The search algorithm allows for small robots (described as cockroach-sized) to “swarm” a search area. Researchers say that this distributed optimization algorithm can help find avalanche victims four times faster than current search mechanisms. For a person buried in an avalanche, the chance of survival plummets after 20 minutes, so every moment counts.

An avy dog in training is picking up scent
Sarah McLear
While rescue gear has been evolving, predicting when a slab will fall remains an emerging science — kind of where weather forecasting science was in the 1980s. Avalanche forecasting still relies on documenting avalanches by going out and looking,” says Ethan Greene, director of the Colorado Avalanche Information Center (CAIC). “So if there's a big snowstorm, and as you might remember, most avalanches happened during snowstorms, we could have 10,000 avalanches that release and we document 50,” says Greene. “Avalanche forecasting is essentially pattern recognition,” he adds--and understanding the layering structure of snow.
However, determining where the hazards lie can be tricky. While a dense layer of snow over a softer, weaker layer may be a recipe for an avalanche, there’s so much variability in snowpack that no one formula can predict the trigger. Further, observing and measuring snow at a single point may not be representative of all nearby slopes. Finally, there’s not enough historical data to help avalanche scientists create better prediction models.
That, however, may be changing.
Last year, an international group of researchers created computer simulations of snow cover using 16 years of meteorological data to forecast avalanche hazards, publishing their research in Cold Regions Science and Technology. They believe their models, which categorize different kinds of avalanches, can support forecasting and determine whether the avalanche is natural (caused by temperature changes, wind, additional snowfall) or artificial (triggered by a human or animal).
With smell receptors ranging from 800 million for an average dog, to 4 billion for scent hounds, canines remain key to finding people caught in slides.
With data from two sites in British Columbia and one in Switzerland, researchers built computer simulations of five different avalanche types. “In terms of real time avalanche forecasting, this has potential to fill in a lot of data gaps, where we don't have field observations of what the snow looks like,” says Simon Horton, a postdoctoral fellow with the Simon Fraser University Centre for Natural Hazards Research and a forecaster with Avalanche Canada, who participated in the study. While complex models that simulate snowpack layers have been around for a few decades, they weren’t easy to apply until recently. “It's been difficult to find out how to apply that to actual decision-making and improving safety,” says Horton. If you can derive avalanche problem types from simulated snowpack properties, he says, you’ll learn “a lot about how you want to manage that risk.”
The five categories include “new snow,” which is unstable and slides down the slope, “wet snow,” when rain or heat makes it liquidly, as well as “wind-drifted snow,” “persistent weak layers” and “old snow.” “That's when there's some type of deeply buried weak layer in the snow that releases without any real change in the weather,” Horton explains. “These ones tend to cause the most accidents.” One step by a person on that structurally weak layer of snow will cause a slide. Horton is hopeful that computer simulations of avalanche types can be used by scientists in different snow climates to help predict hazard levels.
Greene is doubtful. “If you have six slopes that are lined up next to each other, and you're going to try to predict which one avalanches and the exact dimensions and what time, that's going to be really hard to do. And I think it's going to be a long time before we're able to do that,” says Greene.
What both researchers do agree on, though, is that what avalanche prediction really needs is better imagery through satellite detection. “Just being able to count the number of avalanches that are out there will have a huge impact on what we do,” Greene says. “[Satellites] will change what we do, dramatically.” In a 2022 paper, scientists at the University of Aberdeen in England used satellites to study two deadly Himalayan avalanches. The imaging helped them determine that sediment from a 2016 ice avalanche plus subsequent snow avalanches contributed to the 2021 avalanche that caused a flash flood, killing over 200 people. The researchers say that understanding the avalanches characteristics through satellite imagery can inform them how one such event increases the magnitude of another in the same area.

Avy dogs trainers hide in dug-out holes in the snow, teaching the dogs to find buried victims
Sarah McLear
Lifesaving combo: human tech and Mother Nature’s gear
Even as avalanche forecasting evolves, dogs with their built-in rescue mechanisms will remain invaluable. With smell receptors ranging from 800 million for an average dog, to 4 billion for scent hounds, canines remain key to finding people caught in slides. (Humans in comparison, have a meager 12 million.) A new study published in the Journal of Neuroscience revealed that in dogs smell and vision are connected in the brain, which has not been found in other animals. “They can detect the smell of their owner's fingerprints on a glass slide six weeks after they touched it,” says Nicholas Dodman, professor emeritus at Cummings School of Veterinary Medicine at Tufts University. “And they can track from a boat where a box filled with meat was buried in the water, 100 feet below,” says Dodman, who is also co-founder and president of the Center for Canine Behavior Studies.
Another recent study from Queens College in Belfast, United Kingdom, further confirms that dogs can smell when humans are stressed. They can also detect the smell of a person’s breath and the smell of the skin cells of a deceased person.
The emerging avalanche-predicting human-made tech and the incredible nature-made tech of dogs’ olfactory talents is the lifesaving “equipment” that Leffler believes in. Even when human-made technology develops further, it will be most efficient when used together with the millions of dogs’ smell receptors, Leffler believes. “It is a combination of technology and the avalanche dog that will always be effective in finding an avalanche victim.”
