

If approved by the FDA, a new procedure for kidney transplants that doesn't require anti-rejection medication could soon become the standard of care.
Talaris is now moving into the final clinical trial, phase III, before submitting for FDA approval. Known as Freedom-1, this trial has 17 sites open throughout the U.S., and Talaris will enroll a total of 120 kidney transplant recipients. One day after receiving their donor’s kidney, 80 people will undergo the company’s therapy, involving the donor’s stem cells and other critical cells that are processed at their facility. Forty will have a regular kidney transplant and remain on immunosuppression to provide a control group.
“The beauty of this procedure is that I don’t have to take all of the anti-rejection drugs,” says Robert Waddell, a finance professional. “I forget that I ever had any kidney issues. That’s how impactful it is.”
The procedure was pioneered decades ago by Suzanne Ildstad as a faculty member at the University of Pittsburgh before she became founding CEO of Talaris and then its Chief Scientific Officer. If approved by the FDA, the method could soon become the standard of care for patients in need of a kidney transplant.
“We are working to find a way to reprogram the immune system of transplant recipients so that it sees the donated organ as [belonging to one]self and doesn’t attack it,” explains Scott Requadt, CEO of Talaris. “That obviates the need for lifelong immunosuppression.”
Each year, there are roughly 20,000 kidney transplants, making kidneys the most transplanted organ. About 6,500 of those come from living donors, while deceased donors provide roughly 13,000.
One of the challenges, Requadt points out, is that kidney transplant recipients aren’t always aware of all the implications of immunosuppression. Typically, they will need to take about 20 anti-rejection drugs several times a day to provide immunosuppression as well as treat complications caused by the toxicities of immunosuppression medications. The side effects of chronic immunosuppression include weight gain, high blood pressure, and high cholesterol. These cardiovascular comorbidities, Requadt says, are “often more frequently the cause of death than failure of a transplanted organ.”
Patients who are chronically immunosuppressed generally have much higher rates of infections and cancers that have an immune component to them, such as skin cancers.
For the past couple of years, those patients have experienced heightened anxiety because of the COVID-19 pandemic. Immune-suppressing medicine used to protect their new organ also makes it hard for patients to build immunity to foreign invaders like COVID-19.
A study appearing in the Proceedings of the National Academy of Sciences found the probability of a pandemic with similar impact to COVID-19 is about 2 percent in any year, and estimated that the probability of novel disease outbreaks will grow three-fold in the next few decades. All the more reason to identify an FDA-approved alternative to harsh immunosuppressive drugs.
Of the 18 patients during the phase II research trial who received the Talaris therapy, didn’t take immunosuppression medication and were vaccinated, only two ended up with a COVID infection, according to a review of the data. Among patients who needed to continue taking immunosuppressants or those who didn’t have them but were unvaccinated, the rates of infection were between 40 and 60 percent.
In the earlier phase II study by Talaris with 37 patients, the combined transplantation approach allowed 70 percent of patients to get off all immunosuppression.
“We’ve followed that whole cohort for more than six and a half years and one of them for 12 years from transplant, and every single patient that we got off immunosuppression has been able to stay off,” Requadt says.
That one patient, Robert Waddell, 55, was especially thankful to be weaned off immunosuppressive drugs approximately one year after his transplant procedure. The Louisville resident had long watched his mother, sister and other family members with polycystic kidney disease, or PKD, suffer the effects of chronic immunosuppression. That became his greatest fear when he was diagnosed with end stage renal failure.
Waddell enrolled in the phase II research taking place in Louisville after learning about it in early 2006. He chose to remain in the study when it relocated its clinical headquarters to Northwestern University’s medical center in Chicago a couple years later.
Before surgery, he underwent an enervating regimen of chemotherapy and radiation. It’s required to clear out a patient’s bone marrow cells so that they can be replaced by the donor’s cells. Waddell says the result was worth it: he had his combined kidney and immune system stem cell transplant in May 2009, without any need for chronic immunosuppression.
“I call it ‘short-term pain, long-term gain,’ because it was difficult to go through the conditioning, but after that, it was great,” he says. “I’ve talked to so many kidney recipients who say, ‘I wish I would have done that,’ because most people don’t think about clinical trials, but I was very fortunate.”
Waddell has every reason to support the success of this research, especially given the genetic disorder, PKD, that has plagued his family. One of his four children has PKD. He is anxious for the procedure to become standard of care, if and when his son needs it.

The Talaris procedure was pioneered decades ago by Suzanne Ildstad, founding CEO of Talaris and the company's Chief Scientific Officer, pictured here with the current CEO, Scott Requadt.
Talaris
“The beauty of this procedure is that I don’t have to take all of the anti-rejection drugs,” says Waddell, a finance professional. “I forget that I ever had any kidney issues. That’s how impactful it is.”
Talaris will continue to follow Waddell and the rest of his cohort to track the effectiveness and safety of the procedure. According to Requadt, the average life of a transplanted kidney is 12 to 15 years, partly because the immunosuppressive drugs worsen the functioning of the organ each year.
“We were the first group to show that we could robustly and fairly reproducibly do this in a clinical setting in humans,” Requadt says. “Most important, we’ve been able to show that we can still get a good engraftment of the stem cells from the donor, even if there is a profound…mismatch between the donor and the recipient’s immune systems.”
In kidney transplantation, it’s important to match for human leukocyte antigens (HLA) because there is a better graft survival in HLA-identical kidney transplants compared with HLA mismatched transplants.
About three months after the transplant, Talaris researchers look for evidence that the donated immune cells and stem cells have engrafted, while making a donor immune system for the patient. If more than 50 percent of the T cells contain the donor’s DNA after six months, patients can start taking fewer immunosuppressants.
“We know from phase II that in our patients who were able to tolerize [accept the organ without rejection] to their donated organ, we saw completely preserved and in fact slightly increased kidney function,” Requadt says. “So, it stands to reason that if you eliminate the drugs that are associated with declining kidney function that you would preserve kidney function, so hopefully the patient will have that one kidney for life.”
Matthew Cooper, director of kidney and pancreas transplantation for MedStar Georgetown Transplant Institute in Washington, DC, states that, “Right now, the Achilles’ heel is we have such a long waiting list and few donors that people die every day waiting for a kidney transplant. Eventually, we will eliminate the organ shortage so that people won’t die from organ failure.”
Cooper, a nationally recognized clinical transplant surgeon for 20 years, says when he started his career, finding a way for patients to forgo immunosuppression was considered “the Holy Grail” of modern transplant medicine.
“Now that we’ve got the protocols in place and some personal examples of how that can happen, it’s pretty exciting to see that all coming together,” he adds.

Thanks to safety cautions from the COVID-19 pandemic, a strain of influenza has been completely eliminated.
The flu shot, explained
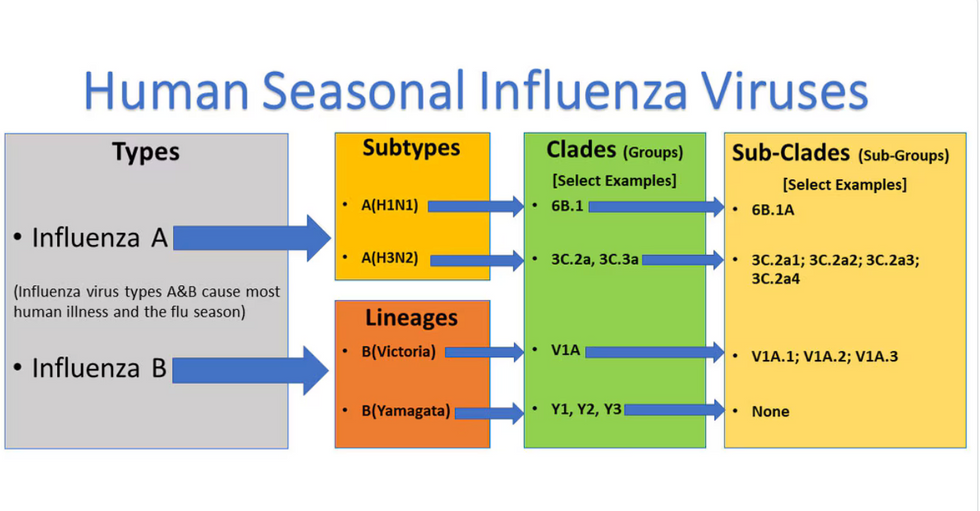
Influenza viruses type A and B are responsible for the majority of human illnesses and the flu season.
Centers for Disease Control
For more than a decade, flu shots have protected against two types of the influenza virus–type A and type B. While there are four different strains of influenza in existence (A, B, C, and D), only strains A, B, and C are capable of infecting humans, and only A and B cause pandemics. In other words, if you catch the flu during flu season, you’re most likely sick with flu type A or B.
Flu vaccines contain inactivated—or dead—influenza virus. These inactivated viruses can’t cause sickness in humans, but when administered as part of a vaccine, they teach a person’s immune system to recognize and kill those viruses when they’re encountered in the wild.
Each spring, a panel of experts gives a recommendation to the US Food and Drug Administration on which strains of each flu type to include in that year’s flu vaccine, depending on what surveillance data says is circulating and what they believe is likely to cause the most illness during the upcoming flu season. For the past decade, Americans have had access to vaccines that provide protection against two strains of influenza A and two lineages of influenza B, known as the Victoria lineage and the Yamagata lineage. But this year, the seasonal flu shot won’t include the Yamagata strain, because the Yamagata strain is no longer circulating among humans.
How Yamagata Disappeared

Flu surveillance data from the Global Initiative on Sharing All Influenza Data (GISAID) shows that the Yamagata lineage of flu type B has not been sequenced since April 2020.
Nature
Experts believe that the Yamagata lineage had already been in decline before the pandemic hit, likely because the strain was naturally less capable of infecting large numbers of people compared to the other strains. When the COVID-19 pandemic hit, the resulting safety precautions such as social distancing, isolating, hand-washing, and masking were enough to drive the virus into extinction completely.
Because the strain hasn’t been circulating since 2020, the FDA elected to remove the Yamagata strain from the seasonal flu vaccine. This will mark the first time since 2012 that the annual flu shot will be trivalent (three-component) rather than quadrivalent (four-component).
Should I still get the flu shot?
The flu shot will protect against fewer strains this year—but that doesn’t mean we should skip it. Influenza places a substantial health burden on the United States every year, responsible for hundreds of thousands of hospitalizations and tens of thousands of deaths. The flu shot has been shown to prevent millions of illnesses each year (more than six million during the 2022-2023 season). And while it’s still possible to catch the flu after getting the flu shot, studies show that people are far less likely to be hospitalized or die when they’re vaccinated.
Another unexpected benefit of dropping the Yamagata strain from the seasonal vaccine? This will possibly make production of the flu vaccine faster, and enable manufacturers to make more vaccines, helping countries who have a flu vaccine shortage and potentially saving millions more lives.

Founder Lewis Hornby and his grandmother Pat, sampling Jelly Drops—an edible gummy containing water and life-saving electrolytes.
When Lewis Hornby visited his grandmother at her nursing home afterward, he learned that dehydration especially affects people with dementia, as they often don’t feel thirst cues at all, or may not recognize how to use cups correctly. But while dementia patients often don’t remember to drink water, it seemed to Hornby that they had less problem remembering to eat, particularly candy.
 Where people with dementia often forget to drink water, they're more likely to pick up a colorful snack, Hornby found. alzheimers.org.uk
Where people with dementia often forget to drink water, they're more likely to pick up a colorful snack, Hornby found. alzheimers.org.uk
Hornby wanted to create a solution for elderly people who struggled keeping their fluid intake up. He spent the next eighteen months researching and designing a solution and securing funding for his project. In 2019, Hornby won a sizable grant from the Alzheimer’s Society, a UK-based care and research charity for people with dementia and their caregivers. Together, through the charity’s Accelerator Program, they created a bite-sized, sugar-free, edible jelly drop that looked and tasted like candy. The candy, called Jelly Drops, contained 95% water and electrolytes—important minerals that are often lost during dehydration. The final product launched in 2020—and was an immediate success. The drops were able to provide extra hydration to the elderly, as well as help keep dementia patients safe, since dehydration commonly leads to confusion, hospitalization, and sometimes even death.
Not only did Jelly Drops quickly become a favorite snack among dementia patients in the UK, but they were able to provide an additional boost of hydration to hospital workers during the pandemic. In NHS coronavirus hospital wards, patients infected with the virus were regularly given Jelly Drops to keep their fluid levels normal—and staff members snacked on them as well, since long shifts and personal protective equipment (PPE) they were required to wear often left them feeling parched.
In April 2022, Jelly Drops launched in the United States. The company continues to donate 1% of its profits to help fund Alzheimer’s research.