
Recent advancements in engineering mean that the first preclinical trials for an artificial kidney could happen soon.
Like all those whose kidneys have failed, Scott Burton’s life revolves around dialysis. For nearly two decades, Burton has been hooked up (or, since 2020, has hooked himself up at home) to a dialysis machine that performs the job his kidneys normally would. The process is arduous, time-consuming, and expensive. Except for a brief window before his body rejected a kidney transplant, Burton has depended on machines to take the place of his kidneys since he was 12-years-old. His whole life, the 39-year-old says, revolves around dialysis.
“Whenever I try to plan anything, I also have to plan my dialysis,” says Burton says, who works as a freelance videographer and editor. “It’s a full-time job in itself.”
Many of those on dialysis are in line for a kidney transplant that would allow them to trade thrice-weekly dialysis and strict dietary limits for a lifetime of immunosuppressants. Burton’s previous transplant means that his body will likely reject another donated kidney unless it matches perfectly—something he’s not counting on. It’s why he’s enthusiastic about the development of artificial kidneys, small wearable or implantable devices that would do the job of a healthy kidney while giving users like Burton more flexibility for traveling, working, and more.
Still, the devices aren’t ready for testing in humans—yet. But recent advancements in engineering mean that the first preclinical trials for an artificial kidney could happen soon, according to Jonathan Himmelfarb, a nephrologist at the University of Washington.
“It would liberate people with kidney failure,” Himmelfarb says.
An engineering marvel
Compared to the heart or the brain, the kidney doesn’t get as much respect from the medical profession, but its job is far more complex. “It does hundreds of different things,” says UCLA’s Ira Kurtz.
Kurtz would know. He’s worked as a nephrologist for 37 years, devoting his career to helping those with kidney disease. While his colleagues in cardiology and endocrinology have seen major advances in the development of artificial hearts and insulin pumps, little has changed for patients on hemodialysis. The machines remain bulky and require large volumes of a liquid called dialysate to remove toxins from a patient’s blood, along with gallons of purified water. A kidney transplant is the next best thing to someone’s own, functioning organ, but with over 600,000 Americans on dialysis and only about 100,000 kidney transplants each year, most of those in kidney failure are stuck on dialysis.
Part of the lack of progress in artificial kidney design is the sheer complexity of the kidney’s job. Each of the 45 different cell types in the kidney do something different.
Part of the lack of progress in artificial kidney design is the sheer complexity of the kidney’s job. To build an artificial heart, Kurtz says, you basically need to engineer a pump. An artificial pancreas needs to balance blood sugar levels with insulin secretion. While neither of these tasks is simple, they are fairly straightforward. The kidney, on the other hand, does more than get rid of waste products like urea and other toxins. Each of the 45 different cell types in the kidney do something different, helping to regulate electrolytes like sodium, potassium, and phosphorous; maintaining blood pressure and water balance; guiding the body’s hormonal and inflammatory responses; and aiding in the formation of red blood cells.
There's been little progress for patients during Ira Kurtz's 37 years as a nephrologist. Artificial kidneys would change that.
UCLA
Dialysis primarily filters waste, and does so well enough to keep someone alive, but it isn’t a true artificial kidney because it doesn’t perform the kidney’s other jobs, according to Kurtz, such as sensing levels of toxins, wastes, and electrolytes in the blood. Due to the size and water requirements of existing dialysis machines, the equipment isn’t portable. Physicians write a prescription for a certain duration of dialysis and assess how well it’s working with semi-regular blood tests. The process of dialysis itself, however, is conducted blind. Doctors can’t tell how much dialysis a patient needs based on kidney values at the time of treatment, says Meera Harhay, a nephrologist at Drexel University in Philadelphia.
But it’s the impact of dialysis on their day-to-day lives that creates the most problems for patients. Only one-quarter of those on dialysis are able to remain employed (compared to 85% of similar-aged adults), and many report a low quality of life. Having more flexibility in life would make a major different to her patients, Harhay says.
“Almost half their week is taken up by the burden of their treatment. It really eats away at their freedom and their ability to do things that add value to their life,” she says.
Art imitates life
The challenge for artificial kidney designers was how to compress the kidney’s natural functions into a portable, wearable, or implantable device that wouldn’t need constant access to gallons of purified and sterilized water. The other universal challenge they faced was ensuring that any part of the artificial kidney that would come in contact with blood was kept germ-free to prevent infection.
As part of the 2021 KidneyX Prize, a partnership between the U.S. Department of Health and Human Services and the American Society of Nephrology, inventors were challenged to create prototypes for artificial kidneys. Himmelfarb’s team at the University of Washington’s Center for Dialysis Innovation won the prize by focusing on miniaturizing existing technologies to create a portable dialysis machine. The backpack sized AKTIV device (Ambulatory Kidney to Increase Vitality) will recycle dialysate in a closed loop system that removes urea from blood and uses light-based chemical reactions to convert the urea to nitrogen and carbon dioxide, which allows the dialysate to be recirculated.
Himmelfarb says that the AKTIV can be used when at home, work, or traveling, which will give users more flexibility and freedom. “If you had a 30-pound device that you could put in the overhead bins when traveling, you could go visit your grandkids,” he says.
Kurtz’s team at UCLA partnered with the U.S. Kidney Research Corporation and Arkansas University to develop a dialysate-free desktop device (about the size of a small printer) as the first phase of a progression that will he hopes will lead to something small and implantable. Part of the reason for the artificial kidney’s size, Kurtz says, is the number of functions his team are cramming into it. Not only will it filter urea from blood, but it will also use electricity to help regulate electrolyte levels in a process called electrodeionization. Kurtz emphasizes that these additional functions are what makes his design a true artificial kidney instead of just a small dialysis machine.
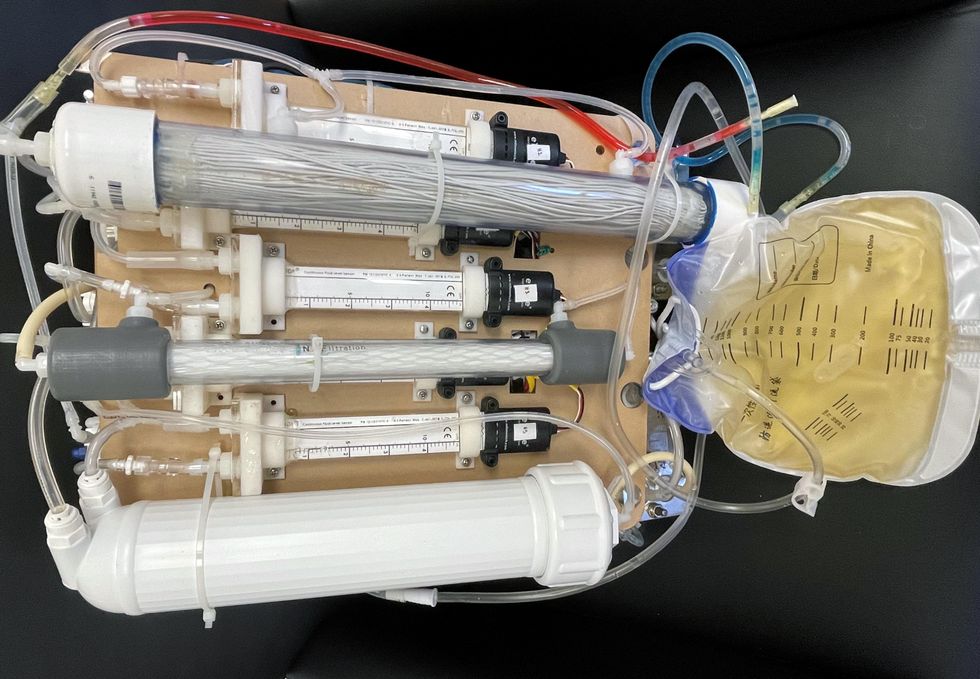
One version of an artificial kidney.
UCLA
“It doesn't have just a static function. It has a bank of sensors that measure chemicals in the blood and feeds that information back to the device,” Kurtz says.
Other startups are getting in on the game. Nephria Bio, a spinout from the South Korean-based EOFlow, is working to develop a wearable dialysis device, akin to an insulin pump, that uses miniature cartridges with nanomaterial filters to clean blood (Harhay is a scientific advisor to Nephria). Ian Welsford, Nephria’s co-founder and CTO, says that the device’s design means that it can also be used to treat acute kidney injuries in resource-limited settings. These potentials have garnered interest and investment in artificial kidneys from the U.S. Department of Defense.
For his part, Burton is most interested in an implantable device, as that would give him the most freedom. Even having a regular outpatient procedure to change batteries or filters would be a minor inconvenience to him.
“Being plugged into a machine, that’s not mimicking life,” he says.
This article was first published by Leaps.org on May 5, 2022.

Insects for sale at a market in Cambodia.
The 21st century wave of entomophagy, or insect eating, first surged in the early 2010s, promoted by a research centre in Wageningen, a university in the Netherlands, conferences organized by the Food and Agriculture Organization of the United Nations, and enthusiastic endorsements by culinary adventurers and celebrities from Europeanized cultures. Headlines announced that two billion people around the world already ate insects, and that if everyone adopted entomophagy we could reduce greenhouse gases, mitigate climate change, and reign in profligate land and water use associated with industrial livestock production.
Furthermore, eating insects was better for human health than eating beef. If we were going to feed the estimated nine billion people with whom we will share the earth in 2050, we would need to make some radical changes in our agriculture and food systems. As one author proclaimed, entomophagy presented us with a last great chance to save the planet.
In 2010, in Kunming, a friend had served me deep-fried bamboo worms. I ate them to be polite. They tasted like French fries, but with heads.
The more recent data suggests that the number of people who eat insects in various forms, though sizeable, may be closer to several hundreds of millions. I knew that from several decades of international veterinary work. Sometimes, for me, insect eating has been simply a way of acknowledging cultural diversity. In 2010, in Kunming, a friend had served me deep-fried bamboo worms. I ate them to be polite. They tasted like French fries, but with heads. My friend said he preferred them chewier. I never thought about them much after that. I certainly had not thought about them as ingredients for human health.
Is consuming insects good for human health? Researchers over the past decade have begun to tease that apart. Some think it might not be useful to use the all-encompassing term insect at all; we don’t lump cows, pigs, chickens into one culinary category. Which insects are we talking about? What are they fed? Were they farmed or foraged? Which stages of the insects are we eating? Do we eat them directly or roasted and ground up?
The overall research indicates that, in general, the usual farmed insects (crickets, locusts, mealworms, soldier fly larvae) have high levels of protein and other important nutrients. If insects are foraged by small groups in Laos, they provide excellent food supplements. Large scale foraging in response to global markets can be incredibly destructive, but soldier fly larvae fed on food waste and used as a substitute for ground up anchovies for farmed fish (as Enterra Feed in Canada does) improves ecological sustainability.
Entomophagy alone might not save the planet, but it does give us an unprecedented opportunity to rethink how we produce and harvest protein.

The author enjoys insects from the Dong Makkhai forest-products market, just outside of Vientiane, the capital of the Lao Peoples Democratic Republic.
David Waltner-Toews
Between 1961 and 2018, world chicken production increased from 4 billion to 20 billion, pork from 200 million to over 100 billion pigs, human populations doubled from 3.5 billion to more than 7 billion, and life expectancy (on average) from 52 to 72 years. These dramatic increases in food production are the result of narrowly focused scientific studies, identifying specific nutrients, antibiotics, vaccines and genetics. What has been missing is any sort of peripheral vision: what are the unintended consequences of our narrowly defined success?
If we look more broadly, we can see that this narrowly defined success led to industrial farming, which caused wealth, health and labor inequities; polluted the environment; and created grounds for disease outbreaks. Recent generations of Europeanized people inherited the ideas of eating cows, pigs and chickens, along with their products, so we were focused only on growing them as efficiently as possible. With insects, we have an exciting chance to start from scratch. Because, for Europeanized people, insect eating is so strange, we are given the chance to reimagine our whole food system in consultation with local experts in Asia and Africa (many of them villagers), and to bring together the best of both locally adapted food production and global distribution.
For this to happen, we will need to change the dietary habits of the big meat eaters. How can we get accustomed to eating bugs? There’s no one answer, but there are a few ways. In many cases, insects are ground up and added as protein supplements to foods like crackers or bars. In certain restaurants, the chefs want you to get used to seeing the bugs as you eat them. At Le Feston Nu in Paris, the Arlo Guthrie look-alike bartender poured me a beer and brought out five small plates, each featuring a different insect in a nest of figs, sun-dried tomatoes, raisins, and chopped dried tropical fruits: buffalo worms, crickets, large grasshoppers (all just crunchy and no strong flavour, maybe a little nutty), small black ants (sour bite), and fat grubs with a beak, which I later identified as palm weevil larvae, tasting a bit like dried figs.
Some entomophagy advertising has used esthetically pleasing presentations in classy restaurants. In London, at the Archipelago restaurant, I dined on Summer Nights (pan fried chermoula crickets, quinoa, spinach and dried fruit), Love-Bug Salad (baby greens with an accompanying dish of zingy, crunchy mealworms fried in olive oil, chilis, lemon grass, and garlic), Bushman’s Cavi-Err (caramel mealworms, bilinis, coconut cream and vodka jelly), and Medieaval Hive (brown butter ice cream, honey and butter caramel sauce and a baby bee drone).

The Archipelago restaurant in London serves up a Love-Bug Salad: baby greens with an accompanying dish of zingy, crunchy mealworms fried in olive oil, chilis, lemon grass, and garlic.
David Waltner-Toews
Some chefs, like Tokyo-based Shoichi Uchiyama, try to entice people with sidewalk cooking lessons. Uchiyama's menu included hornet larvae, silkworm pupae, and silkworms. The silkworm pupae were white and pink and yellow. We snipped off the ends and the larvae dropped out. My friend Zen Kawabata roasted them in a small pan over a camp stove in the street to get the "chaff" off. We made tea from the feces of worms that had fed on cherry blossoms—the tea smelled of the blossoms. One of Uchiyama-san’s assistants made noodles from buckwheat dough that included powdered whole bees.
At a book reading in a Tokyo bookstore, someone handed me a copy of the Japanese celebrity scandal magazine Friday, opened to an article celebrating the “charms of insect eating.” In a photo, scantily-clad girls were drinking vodka and nibbling giant water bugs dubbed as toe-biters, along with pickled and fried locusts and butterfly larvae. If celebrities embraced bug-eating, others might follow. When asked to prepare an article on entomophagy for the high fashion Sorbet Magazine, I started by describing a clip of Nicole Kidman delicately snacking on insects.
Taking a page from the success story of MacDonald’s, we might consider targeting children and school lunches. Kids don’t lug around the same dietary baggage as the grownups, and they can carry forward new eating habits for the long term. When I offered roasted crickets to my grandchildren, they scarfed them down. I asked my five-year-old granddaughter what she thought: she preferred the mealworms to the crickets – they didn’t have legs that caught in her teeth.
Entomo Farms in Ontario, the province where I live, was described in 2015 by Canadian Business magazine as North America’s largest supplier of edible insects for human consumption. When visiting, I popped some of their roasted crickets into my mouth. They were crunchy, a little nutty. Nothing to get squeamish over. Perhaps the human consumption is indeed growing—my wife, at least, has joined me in my entomophagy adventures. When we celebrated our wedding anniversary at the Public Bar and Restaurant in Brisbane, Australia, the “Kang Kong Worms” and “Salmon, Manuka Honey, and Black Ants” seemed almost normal. Of course, the champagne helped.

In this episode of Making Sense of Science, my guest is Raina Plowright, a leading researcher when it comes to how and why viruses sometimes jump from bats to humans.
Listen to the Episode
Listen on Apple | Listen on Spotify | Listen on Stitcher | Listen on Amazon | Listen on Google

Raina Plowright, a disease ecologist at Cornell University, is taking blood and urine samples from hundreds of animals and using GPS tags to follow their movement.
Kelly Gorham