
Recent advancements in engineering mean that the first preclinical trials for an artificial kidney could happen as soon as 18 months from now
Like all those whose kidneys have failed, Scott Burton’s life revolves around dialysis. For nearly two decades, Burton has been hooked up (or, since 2020, has hooked himself up at home) to a dialysis machine that performs the job his kidneys normally would. The process is arduous, time-consuming, and expensive. Except for a brief window before his body rejected a kidney transplant, Burton has depended on machines to take the place of his kidneys since he was 12-years-old. His whole life, the 39-year-old says, revolves around dialysis.
“Whenever I try to plan anything, I also have to plan my dialysis,” says Burton says, who works as a freelance videographer and editor. “It’s a full-time job in itself.”
Many of those on dialysis are in line for a kidney transplant that would allow them to trade thrice-weekly dialysis and strict dietary limits for a lifetime of immunosuppressants. Burton’s previous transplant means that his body will likely reject another donated kidney unless it matches perfectly—something he’s not counting on. It’s why he’s enthusiastic about the development of artificial kidneys, small wearable or implantable devices that would do the job of a healthy kidney while giving users like Burton more flexibility for traveling, working, and more.
Still, the devices aren’t ready for testing in humans—yet. But recent advancements in engineering mean that the first preclinical trials for an artificial kidney could happen as soon as 18 months from now, according to Jonathan Himmelfarb, a nephrologist at the University of Washington.
“It would liberate people with kidney failure,” Himmelfarb says.
An engineering marvel
Compared to the heart or the brain, the kidney doesn’t get as much respect from the medical profession, but its job is far more complex. “It does hundreds of different things,” says UCLA’s Ira Kurtz.
Kurtz would know. He’s worked as a nephrologist for 37 years, devoting his career to helping those with kidney disease. While his colleagues in cardiology and endocrinology have seen major advances in the development of artificial hearts and insulin pumps, little has changed for patients on hemodialysis. The machines remain bulky and require large volumes of a liquid called dialysate to remove toxins from a patient’s blood, along with gallons of purified water. A kidney transplant is the next best thing to someone’s own, functioning organ, but with over 600,000 Americans on dialysis and only about 100,000 kidney transplants each year, most of those in kidney failure are stuck on dialysis.
Part of the lack of progress in artificial kidney design is the sheer complexity of the kidney’s job. Each of the 45 different cell types in the kidney do something different.
Part of the lack of progress in artificial kidney design is the sheer complexity of the kidney’s job. To build an artificial heart, Kurtz says, you basically need to engineer a pump. An artificial pancreas needs to balance blood sugar levels with insulin secretion. While neither of these tasks is simple, they are fairly straightforward. The kidney, on the other hand, does more than get rid of waste products like urea and other toxins. Each of the 45 different cell types in the kidney do something different, helping to regulate electrolytes like sodium, potassium, and phosphorous; maintaining blood pressure and water balance; guiding the body’s hormonal and inflammatory responses; and aiding in the formation of red blood cells.
There's been little progress for patients during Ira Kurtz's 37 years as a nephrologist. Artificial kidneys would change that.
UCLA
Dialysis primarily filters waste, and does so well enough to keep someone alive, but it isn’t a true artificial kidney because it doesn’t perform the kidney’s other jobs, according to Kurtz, such as sensing levels of toxins, wastes, and electrolytes in the blood. Due to the size and water requirements of existing dialysis machines, the equipment isn’t portable. Physicians write a prescription for a certain duration of dialysis and assess how well it’s working with semi-regular blood tests. The process of dialysis itself, however, is conducted blind. Doctors can’t tell how much dialysis a patient needs based on kidney values at the time of treatment, says Meera Harhay, a nephrologist at Drexel University in Philadelphia.
But it’s the impact of dialysis on their day-to-day lives that creates the most problems for patients. Only one-quarter of those on dialysis are able to remain employed (compared to 85% of similar-aged adults), and many report a low quality of life. Having more flexibility in life would make a major different to her patients, Harhay says.
“Almost half their week is taken up by the burden of their treatment. It really eats away at their freedom and their ability to do things that add value to their life,” she says.
Art imitates life
The challenge for artificial kidney designers was how to compress the kidney’s natural functions into a portable, wearable, or implantable device that wouldn’t need constant access to gallons of purified and sterilized water. The other universal challenge they faced was ensuring that any part of the artificial kidney that would come in contact with blood was kept germ-free to prevent infection.
As part of last year’s KidneyX Prize, a partnership between the U.S. Department of Health and Human Services and the American Society of Nephrology, inventors were challenged to create prototypes for artificial kidneys. Himmelfarb’s team at the University of Washington’s Center for Dialysis Innovation won the prize by focusing on miniaturizing existing technologies to create a portable dialysis machine. The backpack sized AKTIV device (Ambulatory Kidney to Increase Vitality) will recycle dialysate in a closed loop system that removes urea from blood and uses light-based chemical reactions to convert the urea to nitrogen and carbon dioxide, which allows the dialysate to be recirculated.
Himmelfarb says that the AKTIV can be used when at home, work, or traveling, which will give users more flexibility and freedom. “If you had a 30-pound device that you could put in the overhead bins when traveling, you could go visit your grandkids,” he says.
Kurtz’s team at UCLA partnered with the U.S. Kidney Research Corporation and Arkansas University to develop a dialysate-free desktop device (about the size of a small printer) as the first phase of a progression that will he hopes will lead to something small and implantable. Part of the reason for the artificial kidney’s size, Kurtz says, is the number of functions his team are cramming into it. Not only will it filter urea from blood, but it will also use electricity to help regulate electrolyte levels in a process called electrodeionization. Kurtz emphasizes that these additional functions are what makes his design a true artificial kidney instead of just a small dialysis machine.
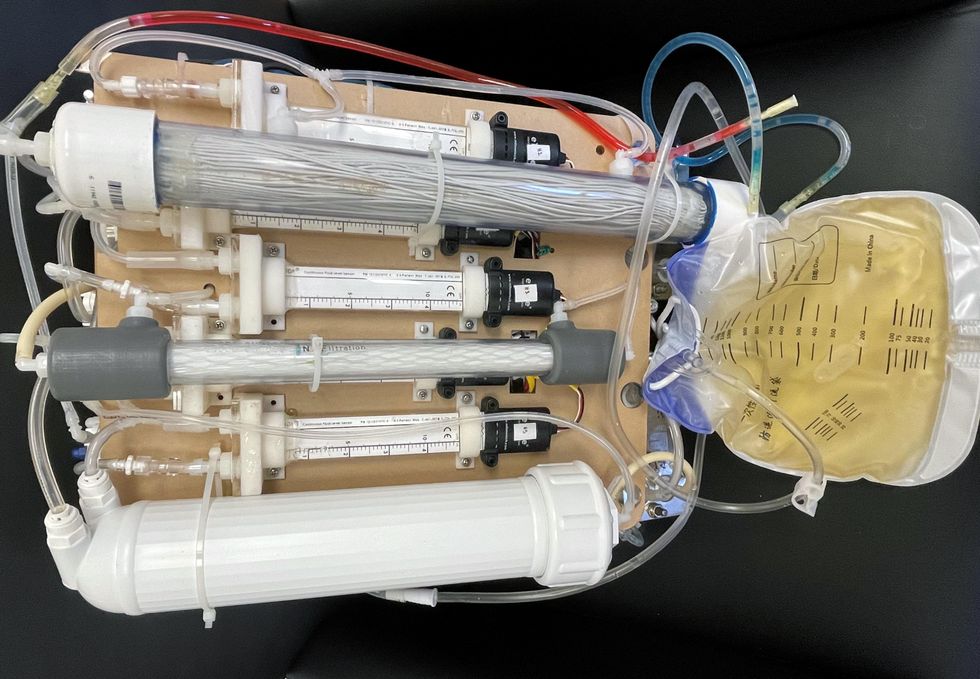
One version of an artificial kidney.
UCLA
“It doesn't have just a static function. It has a bank of sensors that measure chemicals in the blood and feeds that information back to the device,” Kurtz says.
Other startups are getting in on the game. Nephria Bio, a spinout from the South Korean-based EOFlow, is working to develop a wearable dialysis device, akin to an insulin pump, that uses miniature cartridges with nanomaterial filters to clean blood (Harhay is a scientific advisor to Nephria). Ian Welsford, Nephria’s co-founder and CTO, says that the device’s design means that it can also be used to treat acute kidney injuries in resource-limited settings. These potentials have garnered interest and investment in artificial kidneys from the U.S. Department of Defense.
For his part, Burton is most interested in an implantable device, as that would give him the most freedom. Even having a regular outpatient procedure to change batteries or filters would be a minor inconvenience to him.
“Being plugged into a machine, that’s not mimicking life,” he says.


Sonja Bauman, 39, and Mariela Florez, 83, taking one of their regular walks in Plantation, Fla. The pair met through an online platform called Papa that provides "family on demand." (Photo by Sonja Bauman)
In 2020, Papa connected Bauman, the 39-year-old Floridian, with another woman in her mid-70s who lives alone and has very limited mobility. Bauman began driving her to doctor’s appointments and helping her with chores around the house. “When I’m not there, she doesn’t leave her apartment,” said Bauman. The two have gone to the gym together, and they walk slowly through the neighborhood, chatting so it feels less like exercise.
Parker was driven to start Papa by the problem of social isolation among seniors, exacerbated by the pandemic, but he believes users of all ages can benefit. “Many of our Pals feel more comfortable opening up with older members than their same-aged friends,” he said.
Other platforms aim for similar, in-person connections. Generation Tech unites teens with seniors for technology training. And Mon Ami, which provides case management software for aging and disability service providers, has an app that connects isolated older people with college-age volunteers.
Making new connections through video
Several new sites match you with strangers for real-time video chatting on various topics, such as finding common ground on political issues. Other video platforms focus on intergenerational connections.
S. Jay Olshansky, a gerontology professor at the University of Illinois-Chicago, recalls the first time he saw Hyunseung Lee, an 11-year-old from Seoul, through his computer screen. The kid was shy, but Olshansky, 67, encouraged him to ask questions. “Turns out, he was thirsting for this kind of interaction.”
They’d connected through Eldera, a platform that pairs mentors age 60 and up with mentees, using an algorithm, for video conversations. “The time and wisdom of older adults is the most important natural resource we can give future generations,” said Dana Griffin, Eldera's CEO. “Connecting through a screen is the opposite of social media.”
In weekly meetings, Olshansky noticed Lee’s unique interest in math. “There’s something special in you,” Olshansky told him. “How do we bring it to the surface?” He suggested Lee write a book on his favorite subject, and the preteen ran with it, cranking out 70 pages in two weeks. Lee has published his love letter to theorems on Amazon.

Hyunseung Lee, age 11, of Korea, and U.S. college professor Jay Olshanksy, 67, discuss math, strategy and Hyunsung's budding career as a book author during their video chats through a platform called Eldera. (Photo by Dana Palmer/Eldera)
Lee’s parents told Olshansky that their son has become more assertive — a recurring theme, Griffin said. “Confidence is the number one thing parents tell us about.” Since Eldera’s inception last year, the number of mentors has grown exponentially. Even so, Griffin said the waitlist for mentors typically numbers 200 kids.
Another site, Big and Mini, hosts video interactions between seniors and young adults; about 10,000 active users have joined since 2019, said co-founder Aditi Merchant.
Users often bring the benefits of their video interactions to their real-world relationships. Olshansky views Lee as an older version of his grandkids. “Eldera teaches me how to interact with them.” Lee, high on confidence, began instructing his classmates in math. Griffin noted that a group of Eldera mentors in Memphis, who met initially on Eldera, now take walks together in-person to trade ideas for helping each other’s Eldera kids solve problems in their schools and communities.
“We’ve evolved into a community for older adults who want to give back to the world,” said Griffin. Other new tools for connection take the form of virtual reality apps.
Connecting in virtual reality
During pandemic isolation, record numbers of people bought devices for virtual and augmented reality. Such gadgets can convince you that you’re hanging out with friends, even if they’re in another hemisphere. Lifelike simulations from miles away could be especially useful for meaningful interactions between people of different generations, since they’re often geographically segregated.
VR’s benefits require further study, but users report less social isolation and depression, according to MIT research. The immersive, 3-D experience is more compelling than FaceTime or Zoom. “It’s like the difference between a phone call and video call,” said Rick Robinson, Vice President of AARP’s Innovation Labs.
“When VR is designed right, the medium disappears,” said Jeremy Bailenson of Stanford.
Dana Pierce, a 56-year-old government employee in Indiana, got Meta's VR headset in May, 2021, thinking she’d enjoy it more than a new laptop. After many virtual group tours of exotic destinations, she has no regrets. Her adventures occur on Alcove, an app made by Robinson’s Innovation Labs. He co-created it with VR-company Rendever and sought input from people over age 50 to tailor it to their interests. “I’m an introvert,” said Pierce. “I’ve been more socially active since getting my headset than I am in real life.”
Tagging along with her to places like Paris are avatars representing real people around the world. She’s gotten to know VR users in their 70s, 80s and 90s, as well as younger people and some her own age. One is a new friend she plays chess with in relaxing nature settings. Another is her oldest son. He lives 90 minutes away but, earlier this year, Pierce welcomed him and his girlfriend to her virtual house on Alcove. They chatted in the living room decorated with family photos uploaded by Pierce. Then they took out a boat to go VR fishing — because why not — until 2 a.m.
“When VR is designed right, the medium disappears,” said Jeremy Bailenson, a communications professor who directs Stanford’s Virtual Human Interaction Lab. He’s teaching a class of 175 students entirely in VR. After months of covid isolation, the first time the class met, “there was a big catharsis. It really feels like you’re in a big crowd.” Like-minded people meet in VR for events such as comedy shows and creative writing meetups, while the Swedish pop group ABBA has performed this year as digital versions of themselves (“ABBA-tars”) during a virtual concert tour.
Karen Fingerman, a psychologist and director of the Texas Aging and Longevity Center at the University of Texas-Austin, supports the idea of VR for social connection, though she added that some people need it more than others. Hospitals and assisted-living facilities are using products such as Penumbra’s REAL I-Series and MyndVR to bring VR excursions to isolated patients and seniors. “If you’re in a bed or facility, this gives you something to talk about,” said Gita Barry, Penumbra’s executive vice president.
Pierce uses it on most days. She may see another adult son, who lives with her, less often as a result. But VR helps her manage real-world stressors, more than escaping them. After a long workday, she visits her back porch on Alcove, which overlooks a pond. “It’s my little retreat,” she said. “VR improves my mood. It’s added a lot to my life.”
Some seniors are using more than one technology. Olshansky and Lee discuss strategy while playing Internet chess. And Olshansky recently began using VR. He sees his sister, who lives far away, in a virtual beach house. “It’d be a great way to interact with Hyunseung,” he said. “I should get him a headset.”
A version of this article first appeared in The Washington Post on December 3, 2021.