
The U.S. has the highest incarceration rate in the world, costing $182 billion per year, partly because its antiquated data systems often fail to identify people who should be released. A tech nonprofit is trying to change that.
Stand Together
A new non-profit called Recidiviz is using data technology to reduce the size of the U.S. criminal justice system. The bi-coastal company (SF and NYC) is currently working with 11 states to improve their systems and, so far, has helped remove nearly 69,000 people — ones left floundering in jail or on parole when they should have been released.
“The root cause is fragmentation,” says Clementine Jacoby, 31, a software engineer who worked at Google before co-founding Recidiviz in 2019. In the 1970s and 80s, the U.S. built a series of disconnected data systems, and this patchwork is still being used by criminal justice authorities today. It requires parole officers to manually calculate release dates, leading to errors in many cases. “[They] have done everything they need to do to earn their release, but they're still stuck in the system,” Jacoby says.
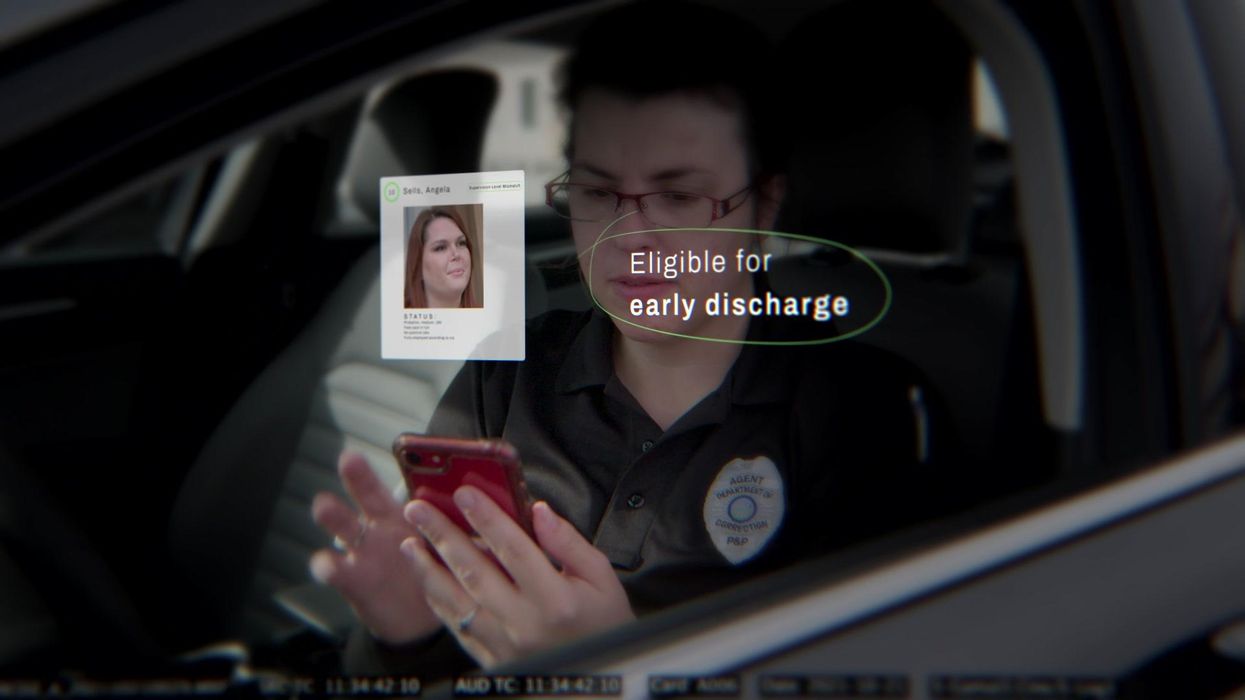
Recidiviz has built a platform that connects the different databases, with the goal of identifying people who are already qualified for release but remain behind bars or on supervision. “Think of Recidiviz like Google Maps,” says Jacoby, who worked on Maps when she was at the tech giant. Google Maps takes in data from different sources – satellite images, street maps, local business data — and organizes it into one easy view. “Recidiviz does something similar with criminal justice data,” Jacoby explains, “making it easy to identify people eligible to come home or to move to less intensive levels of supervision.”
People like Jacoby’s uncle. His experience with incarceration is what inspired her passion for criminal justice reform in the first place.
The problems are vast
The U.S. has the highest incarceration rate in the world — 2 million people according to the watchdog group, Prison Policy Initiative — at a cost of $182 billion a year. The numbers could be a lot lower if not for an array of problems including inaccurate sentencing calculations, flawed algorithms and parole violations laws.
Sentencing miscalculations
To determine eligibility for release, the current system requires corrections officers to check 21 different requirements spread across five different databases for each of the 90 to 100 people under their supervision. These manual calculations are time prohibitive, says Jacoby, and fall victim to human error.
In addition, Recidiviz found that policies aimed at helping to reduce the prison population don’t always work correctly. A key example is time off for good behavior laws that allow inmates to earn one day off for every 30 days of good behavior. Some states' data systems are built to calculate time off as one day per month of good behavior, rather than per day. Over the course of a decade-long sentence, Jacoby says these miscalculations can lead to a huge discrepancy in the calculated release data and the actual release date.
Algorithms
Commercial algorithm-based software systems for risk assessment continue to be widely used in the criminal justice system, even though a 2018 study published in Science Advances exposed their limitations. After the study went viral, it took three years for the Justice Department to issue a report on their own flawed algorithms used to reduce the federal prison population as part of the 2018 First Step Act. The program, it was determined, overestimated the risk of putting inmates of color into early-release programs.
Despite its name, Recidiviz does not build these types of algorithms for predicting recidivism, or whether someone will commit another crime after being released from prison. Rather, Jacoby says the company’s "descriptive analytics” approach is specifically intended to weed out incarceration inequalities and avoid algorithmic pitfalls.
Parole violation laws
Research shows that 350,000 people a year — about a quarter of the total prison population — are sent back not because they’ve committed another crime, but because they’ve broken a specific rule of their probation. “Things that wouldn't send you or I to prison, but would send someone on parole,” such as crossing county lines or being in the presence of alcohol when they shouldn’t be, are inflating the prison population, says Jacoby.
It’s personal for the co-founder and CEO
“I grew up with an uncle who went into the prison system,” Jacoby says. At 19, he was sentenced to ten years in prison for a non-violent crime. A few months after being released from jail, he was sent back for a non-violent parole violation.
“For my family, the fact that one in four prison admissions are driven not by a crime but by someone who's broken a rule on probation and parole was really profound because that happened to my uncle,” Jacoby says. The experience led her to begin studying criminal justice in high school, then college. She continued her dive into how the criminal justice system works as part of her Passion Project while at Google, a program that allows employees to spend 20 percent of their time on pro-bono work. Two colleagues whose family members had also been stuck in the system joined her.
As part of the project, Jacoby interviewed hundreds of people involved in the criminal justice system. “Those on the right, those on the left, agreed that bad data was slowing down reform,” she says. Their research brought them to North Dakota where they began to understand the root of the problem. The corrections department is making “huge, consequential decisions every day [without] … the data,” Jacoby says. In a new video by Recidiviz not yet released, Jacoby recounts her exchange with the state’s director of corrections who told her, “‘It’s not that we have the data and we just don’t know how to make it public; we don’t have the information you think we have.'"
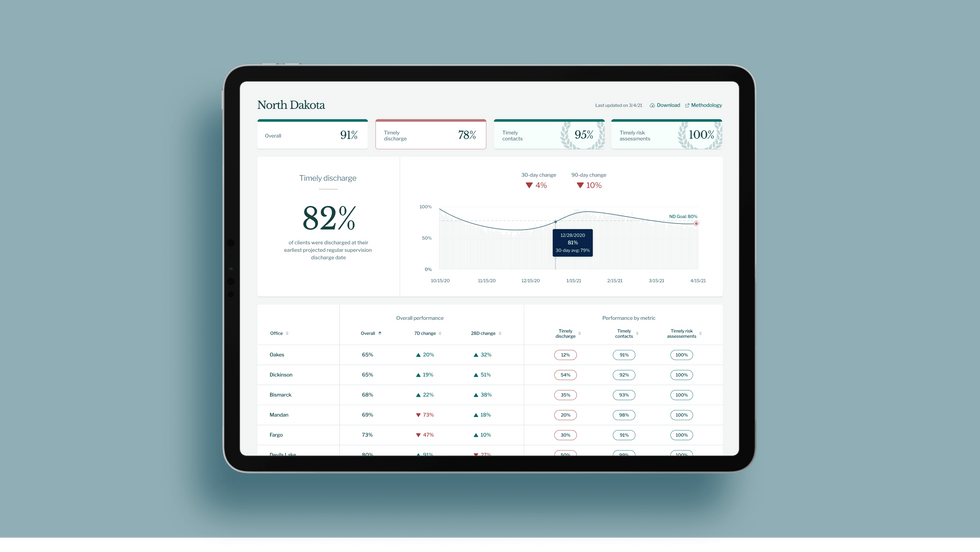
A mock-up (with fake data) of the types of dashboards and insights that Recidiviz provides to state governments.
Recidiviz
As a software engineer, Jacoby says the comment made no sense to her — until she witnessed it first-hand. “We spent a lot of time driving around in cars with corrections directors and parole officers watching them use these incredibly taxing, frankly terrible, old data systems,” Jacoby says.
As they weeded through thousands of files — some computerized, some on paper — they unearthed the consequences of bad data: Hundreds of people in prison well past their release date and thousands more whose release from parole was delayed because of minor paperwork issues. They found individuals stuck in parole because they hadn’t checked one last item off their eligibility list — like simply failing to provide their parole officer with a paystub. And, even when parolees advocated for themselves, the archaic system made it difficult for their parole officers to confirm their eligibility, so they remained in the system. Jacoby and her team also unpacked specific policies that drive racial disparities — such as fines and fees.
The Solution
It’s more than a trivial technical challenge to bring the incomplete, fragmented data onto a 21st century data platform. It takes months for Recidiviz to sift through a state’s information systems to connect databases “with the goal of tracking a person all the way through their journey and find out what’s working for 18- to 25-year-old men, what’s working for new mothers,” explains Jacoby in the video.
TED Talk: How bad data traps people in the U.S. justice system

TED Fellow Clementine Jacoby's TED Talk went live on Jan. 13. It describes how we can fix bad data in the criminal justice system, "bringing thousands of people home, reducing costs and improving public safety along the way."
Clementine Jacoby • TED2022
Ojmarrh Mitchell, an associate professor in the School of Criminology and Criminal Justice at Arizona State University, who is not involved with the company, says what Recidiviz is doing is “remarkable.” His perspective goes beyond academic analysis. In his pre-academic years, Mitchell was a probation officer, working within the framework of the “well known, but invisible” information sharing issues that plague criminal justice departments. The flexibility of Recidiviz’s approach is what makes it especially innovative, he says. “They identify the specific gaps in each jurisdiction and tailor a solution for that jurisdiction.”
On the downside, the process used by Recidiviz is “a bit opaque,” Mitchell says, with few details available on how Recidiviz designs its tools and tracks outcomes. By sharing more information about how its actions lead to progress in a given jurisdiction, Recidiviz could help reformers in other places figure out which programs have the best potential to work well.
The eleven states in which Recidiviz is working include California, Colorado, Maine, Michigan, Missouri, Pennsylvania and Tennessee. And a pilot program launched last year in Idaho, if scaled nationally, with could reduce the number of people in the criminal justice system by a quarter of a million people, Jacoby says. As part of the pilot, rather than relying on manual calculations, Recidiviz is equipping leaders and the probation officers with actionable information with a few clicks of an app that Recidiviz built.
Mitchell is disappointed that there’s even the need for Recidiviz. “This is a problem that government agencies have a responsibility to address,” he says. “But they haven’t.” For one company to come along and fill such a large gap is “remarkable.”


Scientists are studying cancer genomes to more precisely diagnose their patients' diseases - offering hope for targeted drug treatments.
Photo by National Cancer Institute on Unsplash
Next, he recalls, he felt ushered into “the jaws of the medical system very quickly.” He spent a couple of days meeting with a team of doctors at Beth Israel Deaconess Medical Center in nearby Boston. One of them was from a medical field he hadn’t even known existed, a pulmonary interventionist, who would perform a biopsy on the mass in his lung.
“Knowing there was a medicine for my particular type of cancer was like a weight lifted off my shoulders."
A week later he and his wife Allison returned to meet with the oncologist, radiologist, pulmonary interventionist – his medical team. They confirmed his initial diagnosis: Stage 4 metastatic lung cancer that had spread to several parts of his body. “We just sat there, stunned,” he says. “I felt like I was getting hit by a wrecking ball over and over.”
An onslaught of medical terminology about what they had identified flowed over the shocked couple, but then the medical team switched gears, he recalls. They offered hope. “They told me, ‘Hey, you’re not a smoker, so that’s good,’” Reiner says. “‘There’s a good chance that what’s driving this disease for you is actually a genetic mutation, and we have ways to understand more about what that could be through some simple testing.’”
They told him about Foundation Medicine, a company launched in neighboring Cambridge, MA, in 2009 that develops, manufactures, and sells genomic profiling assays. These are tests that, according to the company’s website, “can analyze a broad panel of genes to detect the four main classes of genomic alterations known to drive cancer growth.” With these insights, certain patients can be matched with therapies targeted specifically for the genetic driver(s) of their cancer. The company maintains one of the largest cancer genomic databases in the world, with more than 500,000 patient samples profiled, and they have more than 65 biopharma partners.
According to Foundation Medicine, they are the only company that has FDA-approved tests for both tissue- and blood-based comprehensive genomic profiling tests. One other company has an FDA-approved biopsy test, and several other companies offer tissue-based genomic profiling. Additionally, several major cancer centers like Memorial Sloan Kettering in New York and Anderson Cancer Center in Texas have their own such testing platforms.
Currently, genomic profiling is more accessible for patients with advanced cancer, due to broader insurance coverage in later stages of disease.
“Right now, the vast majority of patients either have cancers for which we don’t have treatments or they have genetic alterations that are not known,” says Jorge Garcia, MD, Division Chief, Solid Tumor Oncology, UH Cleveland Medical Center, which has its own CGP testing platform. “However, a significant proportion of patients with advanced cancer have alterations that we can tap for therapeutic purposes.”
Foundation Medicine estimates that in 2017, just over 5 percent of advanced solid cancer patients in the U.S. received CGP testing. In 2021, they estimate that number is between 25 to 30 percent of advanced solid cancer patients in the U.S., which doesn’t include patients who are tested with small (less than 50 genes) panels. Their panel tests for more than 300 cancer-related genes.

“The good news is the platforms we are developing are better and more comprehensive, and they’re going to continue to be larger data sets,” Dr. Garcia adds.
In Reiner’s case, his team ordered comprehensive genetic profiling on both his tissue and blood, from Foundation Medicine.
At this point, Reiner still wasn’t sure what genetic mutations were or how they factored into cancer or what comprehensive genomic profiling entailed. That day, though, his team ushered the Reiners into the world of precision oncology that placed him on much more sure footing to learn about and fight the specific lung cancer that had been troubling him for more than a year.
What genetic alterations were driving his cancer? Foundation Medicine’s tests were about to find out.
At the core of these tests is next generation sequencing, a DNA sequencing technology. Since 2009, this has revolutionized genomic research, according to the National Center for Biotechnology Information, because it allows an entire human genome to be sequenced within one day. Cancer genomics posits that cancer is caused by mutations and is a disease of the genome. Now, cancer genomes can be systemically studied in their entirety. For cancer patients such as Reiner, NGS can provide a more precise diagnosis and classification of the disease, more accurate prognosis, and potentially the identification of targeted drug treatments. Ultimately, the technology can provide the basis of personalized cancer management.
The detailed reports supply patients and their oncologists with extensive information about the patient’s genomic profile and potential treatment options that they can discuss together. Reiner trusted his doctors that this approach was worth the two- or three-week wait to receive the Foundation Medicine report and the specifically targeted treatment, rather than immediately jump into a round of chemotherapy. He is especially grateful now, he says, because the report delivered a great deal of relief from his previously exhausting and growing anxiety about having cancer.
Reiner and his team learned his lung cancer contained the epidermal growth factor receptor (EGFR) mutation. That biomarker enabled his oncologist to prescribe Tagrisso (osimertinib), a medication developed to directly target that genetic mutation.
“Knowing there was a medicine for my particular type of cancer was like a weight lifted off my shoulders,” he says. “It only took a week or two before my cough finally started subsiding. This pill goes right after the particular piece of genetic material in the tumor that’s causing its growth.”
Dr. Jerry Mitchell, director field medical oncology, Foundation Medicine, in Columbus, Ohio, explains that genomic profiling is generating substantial impacts today. “This is a technology that is the standard of care across many advanced malignancies that takes patients from chemotherapy-only options to very targeted options or immunotherapy options,” he says. “You can also look at complex biomarkers, and these are not specific genetic changes but different genes across the tumor to get a biomarker.”
According to Dr. Mitchell, Foundation Medicine’s technology can test more than 324 different cancer-related genes in a single test. Thus, a growing number of patients are benefitting from comprehensive genetic profiling, due to the rapidly growing number of targeted therapies. While not all of the cancers are treatable yet, the company uses that information to partner with researchers to find new potential therapies for patient groups that may have rare mutations.
Since his tumor’s diagnosis, Reiner has undergone chemotherapy and a couple surgeries to treat the metastatic cancer in other parts of his body, but the drug Tagrisso has significantly reduced his lung tumor. Now, having learned so much during the past couple of years, he is grateful for precision oncology. He still reflects on the probability that, had the Tagrisso pill not been available in May 2019, he might have only survived for another six months or a year.
“Comprehensive Genomic Profiling is not some future state, but in both the U.S. and Europe, it is a very standard, accepted, and recommended first step to knowing how to treat your cancer,” says Dr. Mitchell, adding that he feels fortunate to be an oncologist in this era. “However, we know there are still people not getting this recommended testing, so we still have opportunities to find many more patients and impact them by knowing the molecular profile of their cancer.”