
The U.S. has the highest incarceration rate in the world, costing $182 billion per year, partly because its antiquated data systems often fail to identify people who should be released. A tech nonprofit is trying to change that.
A new non-profit called Recidiviz is using data technology to reduce the size of the U.S. criminal justice system. The bi-coastal company (SF and NYC) is currently working with 11 states to improve their systems and, so far, has helped remove nearly 69,000 people — ones left floundering in jail or on parole when they should have been released.
“The root cause is fragmentation,” says Clementine Jacoby, 31, a software engineer who worked at Google before co-founding Recidiviz in 2019. In the 1970s and 80s, the U.S. built a series of disconnected data systems, and this patchwork is still being used by criminal justice authorities today. It requires parole officers to manually calculate release dates, leading to errors in many cases. “[They] have done everything they need to do to earn their release, but they're still stuck in the system,” Jacoby says.
Recidiviz has built a platform that connects the different databases, with the goal of identifying people who are already qualified for release but remain behind bars or on supervision. “Think of Recidiviz like Google Maps,” says Jacoby, who worked on Maps when she was at the tech giant. Google Maps takes in data from different sources – satellite images, street maps, local business data — and organizes it into one easy view. “Recidiviz does something similar with criminal justice data,” Jacoby explains, “making it easy to identify people eligible to come home or to move to less intensive levels of supervision.”
People like Jacoby’s uncle. His experience with incarceration is what inspired her passion for criminal justice reform in the first place.
The problems are vast
The U.S. has the highest incarceration rate in the world — 2 million people according to the watchdog group, Prison Policy Initiative — at a cost of $182 billion a year. The numbers could be a lot lower if not for an array of problems including inaccurate sentencing calculations, flawed algorithms and parole violations laws.
Sentencing miscalculations
To determine eligibility for release, the current system requires corrections officers to check 21 different requirements spread across five different databases for each of the 90 to 100 people under their supervision. These manual calculations are time prohibitive, says Jacoby, and fall victim to human error.
In addition, Recidiviz found that policies aimed at helping to reduce the prison population don’t always work correctly. A key example is time off for good behavior laws that allow inmates to earn one day off for every 30 days of good behavior. Some states' data systems are built to calculate time off as one day per month of good behavior, rather than per day. Over the course of a decade-long sentence, Jacoby says these miscalculations can lead to a huge discrepancy in the calculated release data and the actual release date.
Algorithms
Commercial algorithm-based software systems for risk assessment continue to be widely used in the criminal justice system, even though a 2018 study published in Science Advances exposed their limitations. After the study went viral, it took three years for the Justice Department to issue a report on their own flawed algorithms used to reduce the federal prison population as part of the 2018 First Step Act. The program, it was determined, overestimated the risk of putting inmates of color into early-release programs.
Despite its name, Recidiviz does not build these types of algorithms for predicting recidivism, or whether someone will commit another crime after being released from prison. Rather, Jacoby says the company’s "descriptive analytics” approach is specifically intended to weed out incarceration inequalities and avoid algorithmic pitfalls.
Parole violation laws
Research shows that 350,000 people a year — about a quarter of the total prison population — are sent back not because they’ve committed another crime, but because they’ve broken a specific rule of their probation. “Things that wouldn't send you or I to prison, but would send someone on parole,” such as crossing county lines or being in the presence of alcohol when they shouldn’t be, are inflating the prison population, says Jacoby.
It’s personal for the co-founder and CEO
“I grew up with an uncle who went into the prison system,” Jacoby says. At 19, he was sentenced to ten years in prison for a non-violent crime. A few months after being released from jail, he was sent back for a non-violent parole violation.
“For my family, the fact that one in four prison admissions are driven not by a crime but by someone who's broken a rule on probation and parole was really profound because that happened to my uncle,” Jacoby says. The experience led her to begin studying criminal justice in high school, then college. She continued her dive into how the criminal justice system works as part of her Passion Project while at Google, a program that allows employees to spend 20 percent of their time on pro-bono work. Two colleagues whose family members had also been stuck in the system joined her.
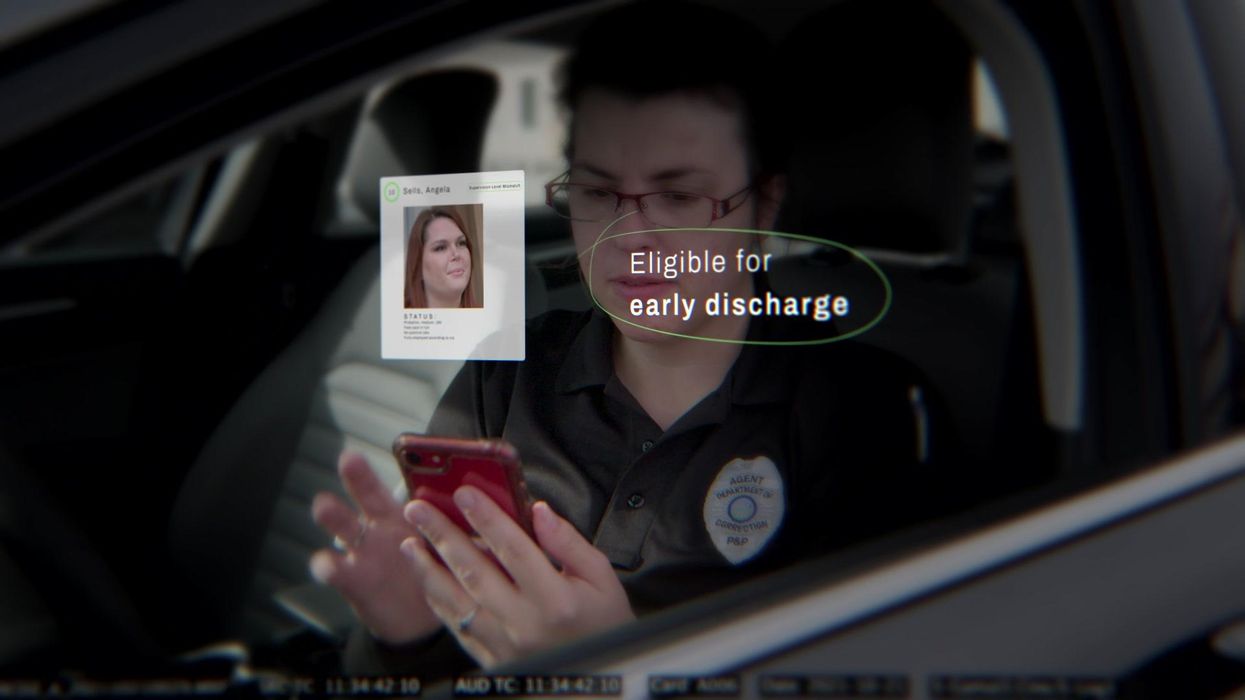
As part of the project, Jacoby interviewed hundreds of people involved in the criminal justice system. “Those on the right, those on the left, agreed that bad data was slowing down reform,” she says. Their research brought them to North Dakota where they began to understand the root of the problem. The corrections department is making “huge, consequential decisions every day [without] … the data,” Jacoby says. In a new video by Recidiviz not yet released, Jacoby recounts her exchange with the state’s director of corrections who told her, “‘It’s not that we have the data and we just don’t know how to make it public; we don’t have the information you think we have.'"
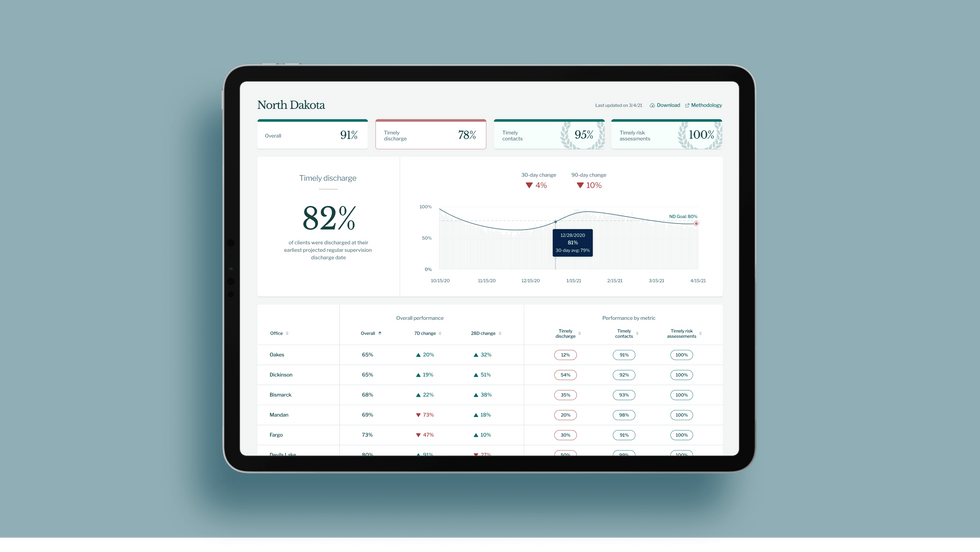
A mock-up (with fake data) of the types of dashboards and insights that Recidiviz provides to state governments.
Recidiviz
As a software engineer, Jacoby says the comment made no sense to her — until she witnessed it first-hand. “We spent a lot of time driving around in cars with corrections directors and parole officers watching them use these incredibly taxing, frankly terrible, old data systems,” Jacoby says.
As they weeded through thousands of files — some computerized, some on paper — they unearthed the consequences of bad data: Hundreds of people in prison well past their release date and thousands more whose release from parole was delayed because of minor paperwork issues. They found individuals stuck in parole because they hadn’t checked one last item off their eligibility list — like simply failing to provide their parole officer with a paystub. And, even when parolees advocated for themselves, the archaic system made it difficult for their parole officers to confirm their eligibility, so they remained in the system. Jacoby and her team also unpacked specific policies that drive racial disparities — such as fines and fees.
The Solution
It’s more than a trivial technical challenge to bring the incomplete, fragmented data onto a 21st century data platform. It takes months for Recidiviz to sift through a state’s information systems to connect databases “with the goal of tracking a person all the way through their journey and find out what’s working for 18- to 25-year-old men, what’s working for new mothers,” explains Jacoby in the video.
TED Talk: How bad data traps people in the U.S. justice system

TED Fellow Clementine Jacoby's TED Talk went live on Jan. 13. It describes how we can fix bad data in the criminal justice system, "bringing thousands of people home, reducing costs and improving public safety along the way."
Clementine Jacoby • TED2022
Ojmarrh Mitchell, an associate professor in the School of Criminology and Criminal Justice at Arizona State University, who is not involved with the company, says what Recidiviz is doing is “remarkable.” His perspective goes beyond academic analysis. In his pre-academic years, Mitchell was a probation officer, working within the framework of the “well known, but invisible” information sharing issues that plague criminal justice departments. The flexibility of Recidiviz’s approach is what makes it especially innovative, he says. “They identify the specific gaps in each jurisdiction and tailor a solution for that jurisdiction.”
On the downside, the process used by Recidiviz is “a bit opaque,” Mitchell says, with few details available on how Recidiviz designs its tools and tracks outcomes. By sharing more information about how its actions lead to progress in a given jurisdiction, Recidiviz could help reformers in other places figure out which programs have the best potential to work well.
The eleven states in which Recidiviz is working include California, Colorado, Maine, Michigan, Missouri, Pennsylvania and Tennessee. And a pilot program launched last year in Idaho, if scaled nationally, with could reduce the number of people in the criminal justice system by a quarter of a million people, Jacoby says. As part of the pilot, rather than relying on manual calculations, Recidiviz is equipping leaders and the probation officers with actionable information with a few clicks of an app that Recidiviz built.
Mitchell is disappointed that there’s even the need for Recidiviz. “This is a problem that government agencies have a responsibility to address,” he says. “But they haven’t.” For one company to come along and fill such a large gap is “remarkable.”

Ordinary people are living better with chronic conditions thanks to a recent explosion of developments in medical implants.
The demand for transplantable organs dwarfs their availability. There are currently over 100,000 people on the transplant waiting list in the U.S., compared to 40,000 transplants completed in 2021. But even this doesn’t reflect the number of people in dire straits who don’t qualify for a transplant because of things like frailty, smoking status and their low odds of surviving the surgery.
My journey to becoming a cyborg came about because of a lifelong medical condition characterized by pathologically low motility of the digestive system, called gastroparesis. Ever since I was in my teens, I’ve had chronic problems with severe nausea. Flareups can be totally incapacitating and last anywhere from hours to months, interspersed with periods of relief. The cycle is totally unpredictable, and for decades my condition went both un- and misdiagnosed by doctors who were not even aware that the condition existed. Over the years I was labeled with whatever fashionable but totally inappropriate medical label existed at the time, and not infrequently, hypochondria.
Living with the gastric pacer is easy. In fact, most of the time, I don’t even know it’s there.
One of the biggest turning points in my life came when a surgeon at the George Washington University Hospital, Dr. Frederick Brody, ordered a gastric emptying test that revealed gastroparesis. This was in 2009, and an implantable device, called a gastric pacer, had been approved by the FDA for compassionate use, meaning that no other treatments were available. The small device is like a pacemaker that’s implanted beneath the skin of the abdomen and is attached to the stomach through electrodes that carry electrical pulses that stimulate the stomach, making it contract as it’s supposed to.
Dr. Brody implanted the electrical wires and the device, and, once my stomach started to respond to the pulses, I got the most significant nausea relief I’d had in decades of futile treatments. It sounds cliché to say that my debt to Dr. Brody is immeasurable, but the pacer has given me more years of relative normalcy than I previously could have dreamed of.
I should emphasize that the pacer is not a cure. I still take a lot of medicine and have to maintain a soft, primarily vegetarian diet, and the condition has progressed with age. I have ups and downs, and can still have periods of severe illness, but there’s no doubt I would be far worse off without the electrical stimulation provided by the pacer.
Living with the gastric pacer is easy. In fact, most of the time, I don’t even know it’s there. It entails periodic visits with a surgeon who can adjust the strength of the electrical pulses using a wireless device, so when symptoms are worse, he or she can amp up the juice. If the pulses are too strong, they can cause annoying contractions in the abdominal muscles, but this is easily fixed with a simple wireless adjustment. The battery runs down after a few years, and when this happens the whole device has to be replaced in what is considered minor surgery.
Such devices could fill gaps in treating other organ failures. By far most of the people on transplant waiting lists are waiting for kidneys. Despite the fact that live donations are possible, there’s still a dire shortage of organs. A bright spot on the horizon is The Kidney Project, a program spearheaded by bioengineer Shuvo Roy at the University of California, San Francisco, which is developing a fully implantable artificial kidney. The device combines living cells with artificial materials and relies not on a battery, but on the patient’s own blood pressure to keep it functioning.
Several years into this project, a prototype of the kidney, about the size of a smart phone, has been successfully tested in pigs. The device seems to provide many of the functions of a biological kidney (unlike dialysis, which replaces only one main function) and reliably produces urine. One of its most critical components is a special artificial membrane, called a hemofilter, that filters out toxins and waste products from the blood without leaking important molecules like albumin. Since it allows for total mobility, the artificial kidney will provide patients with a higher quality of life than those on dialysis, and is in some important ways, even better than a biological transplant.
The beauty of the device is that, even though it contains kidney cells sourced, as of now, from cadavers or pigs, the cells are treated so that they can’t be rejected and the device doesn’t require the highly problematic immunosuppressant drugs a biological organ requires. “Anti-rejection drugs,” says Roy, “make you susceptible to all kinds of infections and damage the transplanted organ, causing steady deterioration. Eventually they kill the kidney. A biological transplant has about a 10-year limit,” after which the kidney fails and the body rejects it.
Eventually, says Roy, the cells used in the artificial kidney will be sourced from the patient himself, the ultimate genetic match. The patient’s adult stem cells can be used to produce some or all of the 25 to 30 specialized cells of a biological kidney that provide all the functions of a natural organ. People formerly on dialysis could drastically improve their functionality and quality of life without being tethered to a machine for hours at a time, three days a week.
As exciting as this project is, it suffers from a common theme in early biomedical research—keeping a steady stream of funding that will move the project from the lab, into human clinical trials and eventually to the bedside. “It’s the issue,” says Roy. “Potential investors want to see more data indicating that it works, but you need funding to create data. It’s a Catch-22 that puts you in a kind of no-man’s land of funding.” The constant pursuit of funding introduces a variable that makes it hard to predict when the kidney will make it to market, despite the enormous need for such a technology.
Another critical variable is if and when insurance companies will decide to cover transplants with the artificial kidney, so that it becomes affordable for the average person. But Roy thinks that this hurdle, too, will be crossed. Insurance companies stand to save a great deal of money compared to what they ordinarily spend on transplant patients. The cost of yearly maintenance will be a fraction of that associated with the tens of thousands of dollars for immunosuppressant drugs and the attendant complications associated with a biological transplant.
One estimate that the multidisciplinary team of researchers involved with The Kidney Project are still trying to establish is how long the artificial kidney will last once transplanted into the body. Animal trials so far have been looking at how the kidney works for 30 days, and will soon extend that study to 90 days. Additional studies will extend much farther into the future, but first the kidneys have to be implanted into people who can be followed over many years to answer this question. But unlike the gastric pacer and other implants, there won’t be a need for periodic surgeries to replace a depleted battery, and the stark improvements in quality of life compared to dialysis add a special dimension to the value of whatever time the kidney lasts.
Another life-saving implant could address a major scourge of the modern world—heart disease. Despite significant advances in recent decades, including the cardiac implants mentioned above, cardiovascular disease still causes one in three deaths across the world. One of the most promising developments in recent years is the Total Artificial Heart, a pneumatically driven device that can be used in patients with biventricular heart failure, affecting both sides of the heart, when a biological organ is not available.
The TAH is implanted in the chest cavity and has two tubes that snake down the body, come out through the abdomen and attach to a 13.5-pound external driver that the patient carries around in a backpack. It was first developed as a bridge to transplant, a temporary alternative while the patient waited for a biological heart to replace it. However, SynCardia Systems, LLC, the Tucson-based company that makes it, is now investigating whether the heart can be used on a long-term basis.
There’s good reason to think that this will be the case. I spoke with Daniel Teo, one of the board members of SynCardia, who said that so far, one patient lived with the TAH for six years and nine months, before he died of other causes. Another patient, still alive, has lived with the device for over five years and another one has lived with it for over four years. About 2,000 of these transplants have been done in patients waiting for biological hearts so far, and most have lived mobile, even active lives. One TAH recipient hiked for 600 miles, and another ran the 4.2-mile Pat Tillman Run, both while on the artificial heart. This is a far cry from their activities before surgery, while living with advanced heart failure.

Randy Shepard, a recipient of the Total Artificial Heart, teaches archery to his son.
Randy Shepard
If removing and replacing one’s biological heart with a synthetic device sounds scary, it is. But then so is replacing one’s heart with biological one. “The TAH is very emotionally loaded for most people,” says Teo. “People sometimes hold back because of philosophical, existential questions and other nonmedical reasons.” He also cites cultural reasons why some people could be hesitant to accept an artificial heart, saying that some religions could frown upon it, just as they forbid other medical interventions.
The first TAHs that were approved were 70 cubic centimeters in size and fit into the chest cavities of men and larger women, but there’s now a smaller, 50 cc size meant for women and adolescents. The FDA first cleared the 70 cc heart as a bridge to transplant in 2004, and the 50 cc model received approval in 2014. SynCardia’s focus now is on seeking FDA approval to use the heart on a long-term basis. There are other improvements in the works.
One issue being refined deals with the external driver that holds the pneumatic device for moving the blood through a patient’s body. The two tubes connecting the driver to the heart entail openings in the skin that could get infected, and carrying the backpack is less than ideal. The driver also makes an audible sound that some people find disturbing. The next generation TAH will be quieter and involve wearing a smaller, lighter device on a belt rather than carrying the backpack. SynCardia is also working toward a fully implantable heart that wouldn’t require any external components and would contain an energy source that can be recharged wirelessly.
Teo says the jury is out as to whether artificial hearts will ever obviate the need for biological organs, but the world’s number one killer isn’t going away any time soon. “The heart is one of the strongest organs,” he says, “but it’s not made to last forever. If you live long enough, the heart will eventually fail, and heart failure leads to the failure of other organs like the kidney, the lungs and the liver.” As long as this remains the case and as long as the current direction of research continues, artificial organs are likely to play an ever larger part of our everyday lives.
Oh, wait. Maybe we cyborgs will take over the world after all.
