
Technology’s Role in Feeding a Soaring Population Raises This Dilemma

When farmer Terry Wanzek walks out in his fields, he sometimes sees a grove of trees, which reminds him of his grandfather, who planted those trees. Or he looks out over the pond, which deer, ducks and pheasant use for water, and he knows that his grandfather made a decision to drain land and put the pond in that exact spot.
Growing more with fewer resources is becoming increasingly urgent as the Earth's population is expected to hit 9.1 billion by 2050.
"There is a connection that goes beyond running a business and making a profit," says Wanzek, a fourth-generation North Dakota farmer who raises spring wheat, corn, soybeans, barley, dry edible beans and sunflowers. "There is a connection to family, to your ancestors and there is a connection to your posterity and your kids."
Wanzek's corn and soybeans are genetically modified (GM) crops, which means that they have been altered at the DNA level to create desirable traits. This intervention, he says, allows him to start growing earlier and to produce more food per acre.
Growing more with fewer resources is becoming increasingly urgent as the Earth's population is expected to hit 9.1 billion by 2050, with nearly all of the rise coming from developing countries, according to the Food and Agriculture Organization of the United Nations. This population will be urban, which means they'll likely be eating fewer grains and other staple crops, and more vegetables, fruits, meat, dairy, and fish.
Whether those foods will be touched in some way by technology remains a high-stakes question. As for GM foods, the American public is somewhat skeptical: in a recent survey, about one-third of Americans report that they are actively avoiding GMOs or seek out non-GMO labels when shopping and purchasing foods. These consumers fear unsafe food and don't want biotechnologists to tamper with nature. This disconnect—between those who consume food and those who produce it—is only set to intensify as major agricultural companies work to develop further high-tech farming solutions to meet the needs of the growing population.
"I don't think we have a choice going forward. The world isn't getting smaller. We have to come up with a means of using less."
In the future, it may be possible to feed the world. But what if the world doesn't want the food?
A Short History
Genetically modified food is not new. The first such plant (the Flavr Savr tomato) was approved for human consumption and brought to market in 1994, but people didn't like the taste. Today, nine genetically modified food crops are commercially available in the United States (corn, soybean, squash, papaya, alfalfa, sugar beets, canola, potato and apples). Most were modified to increase resistance to disease or pests, or tolerance to a specific herbicide. Such crops have in fact been found to increase yields, with a recent study showing grain yield was up to 24.5 percent higher in genetically engineered corn.
Despite some consumer skepticism, many farmers don't have a problem with GM crops, says Jennie Schmidt, a farmer and registered dietician in Maryland. She says with a laugh that her farm is a "grocery store farm - we grow the ingredients you buy in products at the grocery store." Schmidt's father-in-law, who started the farm, watched the adoption of hybrid corn improve seeds in the 1930s and 1940s.
"It wasn't a difficult leap to see how well these hybrid corn seeds have done over the decades," she says. "So when the GMOs came out, it was a quicker adoption curve, because as farmers they had already been exposed to the first generation and this was just the next step."
Schmidt, for one, is excited about the gene-editing tool CRISPR and other ways biotechnologists can create food like apples or potatoes with a particular enzyme turned off so they don't go brown during oxidation. Other foods in the pipeline include disease-resistant citrus, low-gluten wheat, fungus-resistant bananas, and anti-browning mushrooms.
"We need to not judge our agriculture by yield per acre but nutrition per acre."
"I don't think we have a choice going forward," says Schmidt. "The world isn't getting smaller. We have to come up with a means of using less."
A Different Way Forward?
But others remain convinced that there are better ways to feed the planet. Andrew Kimball, executive director of the Center for Food Safety, a non-profit that promotes organic and sustainable agriculture, says the public has been sold a lie with biotech. "GMO technology is not proven as a food producer," he says. "It's just not being done anywhere at a large scale. Ninety-nine percent of GMOs are corn and soy, and they allow chemical companies to sell more chemicals. But that doesn't increase food or decrease hunger." Instead, Kimball advocates for a pivot from commodity agriculture to farms with crop diversity and animals.
Kimball also suggests a way to use land more appropriately: stop growing so much biofuel. Right now, in the U.S., more than 55 percent of our crop farmland is in corn and soy. About 40 percent of that goes into cars through ethanol, 40 percent is fed to animals and a good bit of the rest goes into high-fructose corn syrup. That leaves only a small amount to feed people, says Kimball. "If you want to feed the world, not just the U.S., you want to make sure to use that land to feed people," he says. "We need to not judge our agriculture by yield per acre but nutrition per acre."
Robert Streiffer, a bioethicist at the University of Wisconsin at Madison, agrees that GMOs haven't really helped alleviate hunger. Glyphosate resistance, one of the traits that is most commonly used in genetically engineered crops, doesn't improve yield or allow crops to be grown in areas where they weren't able to be grown before. "Insect resistance through the insertion of a Bt gene can improve yield, but is mostly used for cotton (which is not a food crop) and corn which goes to feed cattle, a very inefficient method of feeding the hungry, to say the least," he says. Important research is being done in crops such as cassava, which could help relieve global hunger. But in his opinion, these researchers lack the profit potential needed to motivate large private funding sources, so they require more public-sector funding.
"A substantial portion of public opposition is as much about the lack of any perceived benefits for the consumers as it is for outright fear of health or environmental dangers."
"Public opposition to biotech foods is certainly a factor, but I expect this will slowly decline as labels indicating the presence of GE (genetically engineered) ingredients become more common, and as we continue to amass reassuring data on the comparative environmental safety of GE crops," says Streiffer. "A substantial portion of public opposition is as much about the lack of any perceived benefits for the consumers as it is for outright fear of health or environmental dangers."
One sign that the public may be willing to embrace some non-natural foods is the recent interest in cultured meat, which is grown in a lab from animal cells but doesn't require raising or killing animals. A study published last year in PLOS One found that 65 percent of 673 surveyed U.S. individuals would probably or definitely try cultured meat, while only 8.5 percent said they definitely would not. In the future, lab-grown food may become another way to create more food with fewer resources.
Danielle Nierenberg, president of the Food Tank, a nonprofit organization focused on building a global community of safe and healthy food, points to an even more immediate problem: food waste. Globally, about a third of food is thrown out or goes bad before it has a chance to be eaten. She says simply fixing roads and infrastructure in developing countries would go a long way toward ensuring that food reaches the hungry. Focusing on helping small farmers (who grow 70 percent of food around the globe), especially female farmers, would go a long way, she says.
Innovation on the Farm
In addition to good roads, those farmers need fertilizer. Nitrogen-based fertilizers may get a boost in the future from technologies that release nutrients slowly over time, like slow-release medicines based on nanotechnology. In field trials on rice in Sri Lanka, one such nanotech fertilizer increased crop yields by 10 percent, even though it delivered only half the amount of urea compared with traditional fertilizer, according to a study last year.
"I'm not afraid of the food I grow. We live in the same environment, and I feel completely safe."
One startup, the San-Francisco-based Biome Makers, is profiling microbial DNA to give farmers an idea of what their soil needs to better support crops. Joyn Bio, another new startup based in Boston and West Sacramento, is looking to engineer microbes that could reduce farming's reliance on nitrogen fertilizer, which is expensive and harms the environment. (Full disclosure: Joyn Bio and this magazine are funded by the same company, Leaps by Bayer, though leapsmag is editorially independent. Also, Bayer recently acquired Monsanto, the leading producer of genetically engineered seeds and the herbicide Roundup.)
Terry Wanzek, the farmer in North Dakota, says he'd be willing to try any new technology as long as it helps his bottom line – and increases sustainability. "I'm not afraid of the food I grow," he says of his genetically modified produce. "We eat the same food, we live in the same environment, and I feel completely safe."
Only time will tell if people several decades from now feel the same way. But no matter how their food is produced, one thing is certain: those people will need to eat.

Last month, a paper published in Cell by Harvard biologist David Sinclair explored root cause of aging, as well as examining whether this process can be controlled. We talked with Dr. Sinclair about this new research.
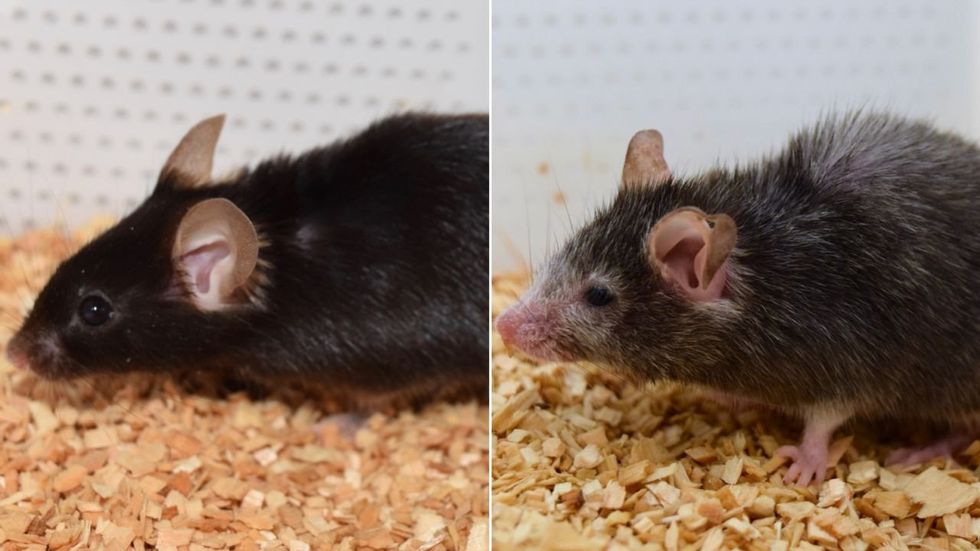
What causes aging? In a paper published last month, Dr. David Sinclair, Professor in the Department of Genetics at Harvard Medical School, reports that he and his co-authors have found the answer. Harnessing this knowledge, Dr. Sinclair was able to reverse this process, making mice younger, according to the study published in the journal Cell.
I talked with Dr. Sinclair about his new study for the latest episode of Making Sense of Science. Turning back the clock on mouse age through what’s called epigenetic reprogramming – and understanding why animals get older in the first place – are key steps toward finding therapies for healthier aging in humans. We also talked about questions that have been raised about the research.
Show links:
Dr. Sinclair's paper, published last month in Cell.
Recent pre-print paper - not yet peer reviewed - showing that mice treated with Yamanaka factors lived longer than the control group.
Dr. Sinclair's podcast.
Previous research on aging and DNA mutations.
Dr. Sinclair's book, Lifespan.

Harvard Medical School
Breakthrough therapies are breaking patients' banks. Key changes could improve access, experts say.

Single-treatment therapies are revolutionizing medicine. But insurers and patients wonder whether they can afford treatment and, if they can, whether the high costs are worthwhile.
CSL Behring’s new gene therapy for hemophilia, Hemgenix, costs $3.5 million for one treatment, but helps the body create substances that allow blood to clot. It appears to be a cure, eliminating the need for other treatments for many years at least.
Likewise, Novartis’s Kymriah mobilizes the body’s immune system to fight B-cell lymphoma, but at a cost $475,000. For patients who respond, it seems to offer years of life without the cancer progressing.
These single-treatment therapies are at the forefront of a new, bold era of medicine. Unfortunately, they also come with new, bold prices that leave insurers and patients wondering whether they can afford treatment and, if they can, whether the high costs are worthwhile.
“Most pharmaceutical leaders are there to improve and save people’s lives,” says Jeremy Levin, chairman and CEO of Ovid Therapeutics, and immediate past chairman of the Biotechnology Innovation Organization. If the therapeutics they develop are too expensive for payers to authorize, patients aren’t helped.
“The right to receive care and the right of pharmaceuticals developers to profit should never be at odds,” Levin stresses. And yet, sometimes they are.
Leigh Turner, executive director of the bioethics program, University of California, Irvine, notes this same tension between drug developers that are “seeking to maximize profits by charging as much as the market will bear for cell and gene therapy products and other medical interventions, and payers trying to control costs while also attempting to provide access to medical products with promising safety and efficacy profiles.”
Why Payers Balk
Health insurers can become skittish around extremely high prices, yet these therapies often accompany significant overall savings. For perspective, the estimated annual treatment cost for hemophilia exceeds $300,000. With Hemgenix, payers would break even after about 12 years.
But, in 12 years, will the patient still have that insurer? Therein lies the rub. U.S. payers, are used to a “pay-as-you-go” model, in which the lifetime costs of therapies typically are shared by multiple payers over many years, as patients change jobs. Single treatment therapeutics eliminate that cost-sharing ability.
"As long as formularies are based on profits to middlemen…Americans’ healthcare costs will continue to skyrocket,” says Patricia Goldsmith, the CEO of CancerCare.
“There is a phenomenally complex, bureaucratic reimbursement system that has grown, layer upon layer, during several decades,” Levin says. As medicine has innovated, payment systems haven’t kept up.
Therefore, biopharma companies begin working with insurance companies and their pharmacy benefit managers (PBMs), which act on an insurer’s behalf to decide which drugs to cover and by how much, early in the drug approval process. Their goal is to make sophisticated new drugs available while still earning a return on their investment.
New Payment Models
Pay-for-performance is one increasingly popular strategy, Turner says. “These models typically link payments to evidence generation and clinically significant outcomes.”
A biotech company called bluebird bio, for example, offers value-based pricing for Zynteglo, a $2.8 million possible cure for the rare blood disorder known as beta thalassaemia. It generally eliminates patients’ need for blood transfusions. The company is so sure it works that it will refund 80 percent of the cost of the therapy if patients need blood transfusions related to that condition within five years of being treated with Zynteglo.
In his February 2023 State of the Union speech, President Biden proposed three pilot programs to reduce drug costs. One of them, the Cell and Gene Therapy Access Model calls on the federal Centers for Medicare & Medicaid Services to establish outcomes-based agreements with manufacturers for certain cell and gene therapies.
A mortgage-style payment system is another, albeit rare, approach. Amortized payments spread the cost of treatments over decades, and let people change employers without losing their healthcare benefits.
Only about 14 percent of all drugs that enter clinical trials are approved by the FDA. Pharma companies, therefore, have an exigent need to earn a profit.
The new payment models that are being discussed aren’t solutions to high prices, says Bill Kramer, senior advisor for health policy at Purchaser Business Group on Health (PBGH), a nonprofit that seeks to lower health care costs. He points out that innovative pricing models, although well-intended, may distract from the real problem of high prices. They are attempts to “soften the blow. The best thing would be to charge a reasonable price to begin with,” he says.
Instead, he proposes making better use of research on cost and clinical effectiveness. The Institute for Clinical and Economic Review (ICER) conducts such research in the U.S., determining whether the benefits of specific drugs justify their proposed prices. ICER is an independent non-profit research institute. Its reports typically assess the degrees of improvement new therapies offer and suggest prices that would reflect that. “Publicizing that data is very important,” Kramer says. “Their results aren’t used to the extent they could and should be.” Pharmaceutical companies tend to price their therapies higher than ICER’s recommendations.
Drug Development Costs Soar
Drug developers have long pointed to the onerous costs of drug development as a reason for high prices.
A 2020 study found the average cost to bring a drug to market exceeded $1.1 billion, while other studies have estimated overall costs as high as $2.6 billion. The development timeframe is about 10 years. That’s because modern therapeutics target precise mechanisms to create better outcomes, but also have high failure rates. Only about 14 percent of all drugs that enter clinical trials are approved by the FDA. Pharma companies, therefore, have an exigent need to earn a profit.
Skewed Incentives Increase Costs
Pricing isn’t solely at the discretion of pharma companies, though. “What patients end up paying has much more to do with their PBMs than the actual price of the drug,” Patricia Goldsmith, CEO, CancerCare, says. Transparency is vital.
PBMs control patients’ access to therapies at three levels, through price negotiations, pricing tiers and pharmacy management.
When negotiating with drug manufacturers, Goldsmith says, “PBMs exchange a preferred spot on a formulary (the insurer’s or healthcare provider’s list of acceptable drugs) for cash-base rebates.” Unfortunately, 25 percent of the time, those rebates are not passed to insurers, according to the PBGH report.
Then, PBMs use pricing tiers to steer patients and physicians to certain drugs. For example, Kramer says, “Sometimes PBMs put a high-cost brand name drug in a preferred tier and a lower-cost competitor in a less preferred, higher-cost tier.” As the PBGH report elaborates, “(PBMs) are incentivized to include the highest-priced drugs…since both manufacturing rebates, as well as the administrative fees they charge…are calculated as a percentage of the drug’s price.
Finally, by steering patients to certain pharmacies, PBMs coordinate patients’ access to treatments, control patients’ out-of-pocket costs and receive management fees from the pharmacies.
Therefore, Goldsmith says, “As long as formularies are based on profits to middlemen…Americans’ healthcare costs will continue to skyrocket.”
Transparency into drug pricing will help curb costs, as will new payment strategies. What will make the most impact, however, may well be the development of a new reimbursement system designed to handle dramatic, breakthrough drugs. As Kramer says, “We need a better system to identify drugs that offer dramatic improvements in clinical care.”