It all relates back to a profound question: How do we know what we know?
Many of these treatments fall by the wayside as evidence accumulates regarding actual efficacy. At that point, other treatments become standard of care once their benefit is proven in rigorously designed trials.
However, about seven months into the pandemic, we're still seeing political resurrection of a treatment that has been systematically studied and demonstrated in well-designed randomized controlled trials to not have benefit.
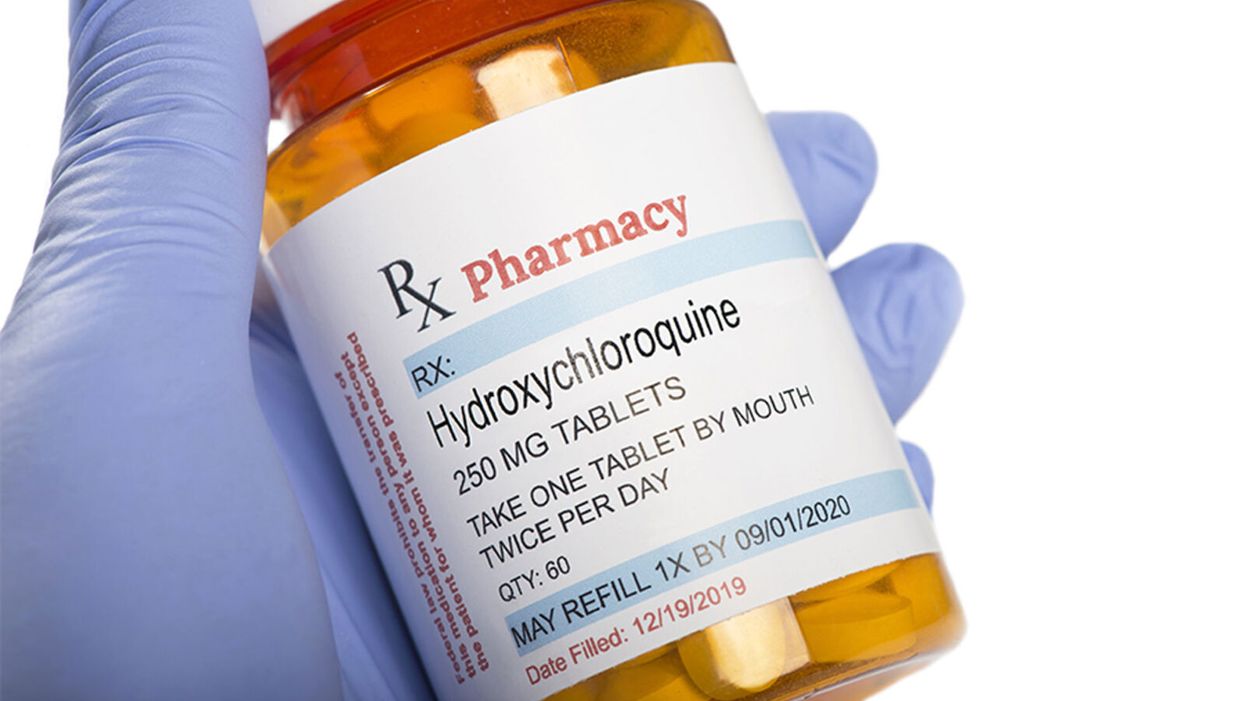
The hydroxychloroquine (and by extension chloroquine) story is a complicated one that was difficult to follow even before it became infused with politics. It is a simple fact that these drugs, long approved by the Food and Drug Administration (FDA), work in Petri dishes against various viruses including coronaviruses. This set of facts provided biological plausibility to support formally studying their use in the clinical treatment and prevention of COVID-19. As evidence from these studies accumulates, it is a cognitive requirement to integrate that knowledge and not to evade it. This also means evaluating the rigor of the studies.
In recent days we have seen groups yet again promoting the use of hydroxychloroquine in, what is to me, a baffling disregard of the multiple recent studies that have shown no benefit. Indeed, though FDA-approved for other indications like autoimmune conditions and preventing malaria, the emergency use authorization for COVID-19 has been rescinded (which means the government cannot stockpile it). Still, however, many patients continue to ask for the drug, compelled by political commentary, viral videos, and anecdotal data. Yet most doctors (like myself) are refusing to write the prescriptions outside of a clinical trial – a position endorsed by professional medical organizations such as the American College of Physicians and the Infectious Diseases Society of America. Why this disconnect?
It all relates back to a profound question: How do we know what we know? In science, we use the scientific method – the process of observing reality, coming up with a hypothesis about what might be true, and testing that hypothesis as thoroughly as possible until we discover the objective truth.
The confusion we're seeing now stems from an inability to distinguish between anecdotes reported by physicians (observational data) and an actual evidence base. This is understandable among the general public but when done by a healthcare professional, it reveals a disdain for reason, logic, and the scientific method.
The Difference Between Observational Data and Randomized Controlled Trials
The power of informal observation is crucial. It is part of the scientific method but primarily as a basis for generating hypotheses that we can test. How do we conduct medical tests? The gold standard is the double-blind, randomized, placebo-controlled trial. This means that neither the researchers nor the volunteers know who is getting a drug and who is getting a sugar pill. Then both groups of the trial, called arms, can be compared to determine whether the people who got the drug fared better. This study design prevents biases and the placebo effect from confounding the data and undermining the veracity of the results.
For example, a seemingly beneficial effect might be seen in an observational study with no blinding and no control group. In such a case, all patients are openly given the drug and their doctors observe how they do. A prime example is the 36-patient single-arm study from France that generated a tremendous amount of interest after President Trump tweeted about it. But this kind of a study by its nature cannot answer the critical question: Was the positive effect because of hydroxychloroquine or just the natural course of the illness? In other words, would someone have recovered in a similar fashion regardless of the drug? What is the role of the placebo effect?
These are reasons why it is crucial to give a placebo to a control group that is as similar in every respect as possible to those receiving the intervention. Then we attempt to find out by comparing the two groups: What is the side effect profile of the drug? Are the groups large enough to detect a relatively rare safety concern? How long were the patients followed for? Was something else responsible for making the patients get better, such as the use of steroids (as likely was the case in the Henry Ford study)?
Looking at the two major hydroxychloroquine trials, it is apparent that, when studied using the best tools of clinical trials, no benefit is likely to occur.
All of these considerations amount to just a fraction of the questions that can be answered more definitively in a well-designed large randomized controlled trial than in observational studies. Indeed, an observational study from New York failed to show any benefit in hospitalized patients, showing how unclear and disparate the results can be with these types of studies. A New York retrospective study (which examined patient outcomes after they were already treated) had similar results and included the use of azithromycin.
When evaluating a study, it is also important to note whether conflicts of interest exist, as well as the quality of the peer review and the data itself. In the case of the French study, for example, the paper was published in a journal in which one of the authors was editor-in-chief, and it was accepted for publication after 24 hours. Patients who fared poorly on hydroxychloroquine were also left out of the study altogether, skewing the results.
What Randomized Controlled Trials Have Shown
Looking at the two major hydroxychloroquine trials, it is apparent that, when studied using the best tools of clinical trials, no benefit is likely to occur. The most important of these studies to announce results was part of the Recovery trial, which was designed to test multiple interventions in the treatment of COVID-19. This trial, which has yet to be formally published, was a randomized controlled trial that involved over 1500 hospitalized patients being administered hydroxychloroquine compared to over 3000 who did not receive the medication. Clinical testing requires large numbers of patients to have the power to demonstrate statistical significance -- the threshold at which any apparent benefit is more than you would expect by random chance alone.
In this study, hydroxychloroquine provided no mortality benefit or even a benefit in hospital length of stay. In fact, the opposite occurred. Hydroxychloroquine patients were more likely to stay in the hospital longer and were more likely to require mechanical ventilation. Additionally, smaller randomized trials conducted in China have not shown benefit either.
Another major study involved the use of hydroxychloroquine to prevent illness in people who were exposed to COVID-19. These results, published in The New England Journal of Medicine, included over 800 patients who were studied in a randomized double-blind controlled trial and also failed to show any benefit.
But what about adding the antibiotic azithromycin in conjunction with hydroxychloroquine? A three-arm randomized controlled study involving over 500 patients hospitalized with mild to moderate COVID-19 was conducted. Its results, also published in The New England Journal of Medicine, failed to show any benefit – with or without azithromycin – and demonstrated evidence of harm. Those who received these treatments had elevations of their liver function tests and heart rhythm abnormalities. These findings hold despite the retraction of an observational study showing similar results.
Additionally, when used in combination with remdesivir – an experimental antiviral – hydroxychloroquine has been shown to be associated with worse outcomes and more side effects.
But what about in mildly ill patients not requiring hospitalization? There was no benefit found in a randomized double-blind placebo-controlled trial of 400 patients, the majority of whom were given the drug within one day of symptoms.
Some randomized controlled studies have yet to report their findings on hydroxychloroquine in non-hospitalized patients, with the use of zinc (which has some evidence in the treatment of the common cold, another ailment that can be caused by coronaviruses). And studies have yet to come out regarding whether hydroxychloroquine can prevent people from getting sick before they are even exposed. But the preponderance of the evidence from studies designed specifically to find benefit for treating COVID-19 does not support its use outside of a research setting.
Today – even with some studies (including those with zinc) still ongoing – if a patient asked me to prescribe them hydroxychloroquine for any severity or stage of illness, with or without zinc, with or without azithromycin, I would refrain. I would explain that, based on the evidence from clinical trials that has been amassed, there is no reason to believe that it will alter the course of illness for the better.
Failing to recognize the reality of the situation runs the risk of crowding out other more promising treatments and creating animosity where none should exist.
What has been occurring is a continual shifting of goalposts with each negative hydroxychloroquine study. Those in favor of the drug protest that a trial did not include azithromycin or zinc or wasn't given at the right time to the right patients. While there may be biological plausibility to treating illness early or combining treatments with zinc, it can only be definitively shown in a randomized, controlled prospective study.
The bottom line: A study that only looks at past outcomes in one group of patients – even when well conducted – is at most hypothesis generating and cannot be used as the sole basis for a new treatment paradigm.
Some may argue that there is no time to wait for definitive studies, but no treatment is benign. The risk/benefit ratio is not the same for every possible use of the drug. For example, hydroxychloroquine has a long record of use in rheumatoid arthritis and systemic lupus (whose patients are facing shortages because of COVID-19 related demand). But the risk of side effects for many of these patients is worth taking because of the substantial benefit the drug provides in treating those conditions.
In COVID-19, however, the disease apparently causes cardiac abnormalities in a great deal of many mild cases, a situation that should prompt caution when using any drugs that have known effects on the cardiac system -- drugs like hydroxychloroquine and azithromycin.
My Own Experience
It is not the case that every physician was biased against this drug from the start. Indeed, most of us wanted it to be shown to be beneficial, as it was a generic drug that was widely available and very familiar. In fact, early in the pandemic I prescribed it to hospitalized patients on two occasions per a hospital protocol. However, it is impossible for me as a sole clinician to know whether it worked, was neutral, or was harmful. In recent days, however, I have found the hydroxychloroquine talk to have polluted the atmosphere. One recent patient was initially refusing remdesivir, a drug proven in large randomized trials to have effectiveness, because he had confused it with hydroxychloroquine.
Moving On to Other COVID Treatments: What a Treatment Should Do
The story of hydroxychloroquine illustrates a fruitless search for what we are actually looking for in a COVID-19 treatment. In short, we are looking for a medication that can decrease symptoms, decrease complications, hasten recovery, decrease hospitalizations, decrease contagiousness, decrease deaths, and prevent infection. While it is unlikely to find a single antiviral that can accomplish all of these, fulfilling even just one is important.
For example, remdesivir hastens recovery and dexamethasone decreases mortality. Definitive results of the use of convalescent plasma and immunomodulating drugs such as siltuxamab, baricitinib, and anakinra (for use in the cytokine storms characteristic of severe disease) are still pending, as are the trials with monoclonal antibodies.
While it was crucial that the medical and scientific community definitively answer the questions surrounding the use of chloroquine and hydroxychloroquine in the treatment of COVID-19, it is time to face the facts and accept that its use for the treatment of this disease is not likely to be beneficial. Failing to recognize the reality of the situation runs the risk of crowding out other more promising treatments and creating animosity where none should exist.