
The Promise of Pills That Know When You Swallow Them

A woman prepares to swallow a digital pill that can track whether she has taken her medication.
Dr. Sara Browne, an associate professor of clinical medicine at the University of California, San Diego, is a specialist in infectious diseases and, less formally, "a global health person." She often travels to southern Africa to meet with colleagues working on the twin epidemics of HIV and tuberculosis.
"This technology, in my opinion, is an absolute slam dunk for tuberculosis."
Lately she has asked them to name the most pressing things she can help with as a researcher based in a wealthier country. "Over and over and over again," she says, "the only thing they wanted to know is whether their patients are taking the drugs."
Tuberculosis is one of world's deadliest diseases; every year there are 10 million new infections and more than a million deaths. When a patient with tuberculosis is prescribed medicine to combat the disease, adherence to the regimen is important not just for the individual's health, but also for the health of the community. Poor adherence can lead to lengthier and more costly treatment and, perhaps more importantly, to drug-resistant strains of the disease -- an increasing global threat.
Browne is testing a new method to help healthcare workers track their patients' adherence with greater precision—close to exact precision even. They're called digital pills, and they involve a patient swallowing medicine as they normally would, only the capsule contains a sensor that—when it contacts stomach acid—transmits a signal to a small device worn on or near the body. That device in turn sends a signal to the patient's phone or tablet and into a cloud-based database. The fact that the pill has been swallowed has therefore been recorded almost in real time, and notice is available to whoever has access to the database.
"This technology, in my opinion, is an absolute slam dunk for tuberculosis," Browne says. TB is much more prevalent in poorer regions of the world—in Sub-Saharan Africa, for example—than in richer places like the U.S., where Browne's studies thus far have taken place. But when someone is diagnosed in the U.S., because of the risk to others if it spreads, they will likely have to deal with "directly observed therapy" to ensure that they take their medicines correctly.
DOT, as it's called, requires the patient to meet with a healthcare worker several days a week, or every day, so that the medicine intake can be observed in person -- an expensive and time-consuming process. Still, the Centers for Disease Control and Prevention website says (emphasis theirs), "DOT should be used for ALL patients with TB disease, including children and adolescents. There is no way to accurately predict whether a patient will adhere to treatment without this assistance."
Digital pills can help with both the cost and time involved, and potentially improve adherence in places where DOT is impossibly expensive. With the sensors, you can monitor a patient's adherence without a healthcare worker physically being in the room. Patients can live their normal lives and if they miss a pill, they can receive a reminder by text or a phone call from the clinic or hospital. "They can get on with their lives," said Browne. "They don't need the healthcare system to interrupt them."
A 56-year-old patient who participated in one of Browne's studies when he was undergoing TB treatment says that before he started taking the digital pills, he would go to the clinic at least once every day, except weekends. Once he switched to digital pills, he could go to work and spend time with his wife and children instead of fighting traffic every day to get to the clinic. He just had to wear a small patch on his abdomen, which would send the signal to a tablet provided by Browne's team. When he returned from work, he could see the results—that he'd taken the pill—in a database accessed via the tablet. (He could also see his heart rate and respiratory rate.) "I could do my daily activities without interference," he said.
Dr. Peter Chai, a medical toxicologist and emergency medicine physician at Brigham and Women's Hospital in Boston, is studying digital pills in a slightly different context, to help fight the country's opioid overdose crisis. Doctors like Chai prescribe pain medicine, he says, but then immediately put the onus on the patient to decide when to take it. This lack of guidance can lead to abuse and addiction. Patients are often told to take the meds "as needed." Chai and his colleagues wondered, "What does that mean to patients? And are people taking more than they actually need? Because pain is such a subjective experience."
The patients "liked the fact that somebody was watching them."
They wanted to see what "take as needed" actually led to, so they designed a study with patients who had broken a bone and come to the hospital's emergency department to get it fixed. Those who were prescribed oxycodone—a pharmaceutical opioid for pain relief—got enough digital pills to last one week. They were supposed to take the pills as needed, or as many as three pills per day. When the pills were ingested, the sensor sent a signal to a card worn on a lanyard around the neck.
Chai and his colleagues were able to see exactly when the patients took the pills and how many, and to detect patterns of ingestion more precisely than ever before. They talked to the patients after the seven days were up, and Chai said most were happy to be taking digital pills. The patients saw it as a layer of protection from afar. "They liked the fact that somebody was watching them," Chai said.
Both doctors, Browne and Chai, are in early stages of studies with patients taking pre-exposure prophylaxis, medicines that can protect people with a high-risk of contracting HIV, such as injectable drug users. Without good adherence, patients leave themselves open to getting the virus. If a patient is supposed to take a pill at 2 p.m. but the digital pill sensor isn't triggered, the healthcare provider can have an automatic message sent as a reminder. Or a reminder to one of the patient's friends or loved ones.
"Like Swallowing Your Phone"?
Deven Desai, an associate professor of law and ethics at Georgia Tech, says that digital pills sound like a great idea for helping with patient adherence, a big issue that self-reporting doesn't fully solve. He likes the idea of a physician you trust having better information about whether you're taking your medication on time. "On the surface that's just cool," he says. "That's a good thing." But Desai, who formerly worked as academic research counsel at Google, said that some of the same questions that have come up in recent years with social media and the Internet in general also apply to digital pills.
"Think of it like your phone, but you swallowed it," he says. "At first it could be great, simple, very much about the user—in this case, the patient—and the data is going between you and your doctor and the medical people it ought to be going to. Wonderful. But over time, phones change. They become 'smarter.'" And when phones and other technologies become smarter, he says, the companies behind them tend to expand the type of data they collect, because they can. Desai says it will be crucial that prescribers be completely transparent about who is getting the patients' data and for what purpose.
"We're putting stuff in our body in good faith with our medical providers, and what if it turned out later that all of a sudden someone was data mining or putting in location trackers and we never knew about that?" Desai asks. "What science has to realize is if they don't start thinking about this, what could be a wonderful technology will get killed."
Leigh Turner, an associate professor at the University of Minnesota's Center for Bioethics, agrees with Desai that digital pills have great promise, and also that there are clear reasons to be concerned about their use. Turner compared the pills to credit cards and social media, in that the data from them can potentially be stolen or leaked. One question he would want answered before the pills were normalized: "What kind of protective measures are in place to make sure that personal information isn't spilling out and being acquired by others or used by others in unexpected and unwanted ways?"
If digital pills catch on, some experts worry that they may one day not be a voluntary technology.
Turner also wonders who will have access to the pills themselves. Only those who can afford both the medicine plus the smartphones that are currently required for their use? Or will people from all economic classes have access? If digital pills catch on, he also worries they may one day not be a voluntary technology.
"When it comes to digital pills, it's not something that's really being foisted on individuals. It's more something that people can be informed of and can choose to take or not to take," he says. "But down the road, I can imagine a scenario where we move away from purely voluntary agreements to it becoming more of an expectation."
He says it's easy to picture a scenario in which insurance companies demand that patient medicinal intake data be tracked and collected or else. Refuse to have your adherence tracked and you risk higher rates or even overall coverage. Maybe patients who don't take the digital pills suffer dire consequences financially or medically. "Maybe it becomes beneficial as much to health insurers and payers as it is to individual patients," Turner says.
In November 2017, the FDA approved the first-ever digital pill that includes a sensor, a drug called Abilify MyCite, made by Otsuka Pharmaceutical Company. The drug, which is yet to be released, is used to treat schizophrenia, bipolar disorder, and depression. With a built-in sensor developed by Proteus Digital Health, patients can give their doctors permission to see when exactly they are taking, or not taking, their meds. For patients with mental illness, the ability to help them stick to their prescribed regime can be life-saving.
But Turner wonders if Abilify is the best drug to be a forerunner for digital pills. Some people with schizophrenia might be suffering from paranoia, and perhaps giving them a pill developed by a large corporation that sends data from their body to be tracked by other people might not be the best idea. It could in fact exacerbate their sense of paranoia.
The Bottom Line: Protect the Data
We all have relatives who have pillboxes with separate compartments for each day of the week, or who carry pillboxes that beep when it's time to take the meds. But that's not always good enough for people with dementia, mental illness, drug addiction, or other life situations that make it difficult to remember to take their pills. Digital pills can play an important role in helping these people.
"The absolute principle here is that the data has to belong to the patient."
The one time the patient from Browne's study forgot to take his pills, he got a beeping reminder from his tablet that he'd missed a dose. "Taking a medication on a daily basis, sometimes we just forget, right?" he admits. "With our very accelerated lives nowadays, it helps us to remember that we have to take the medications. So patients are able to be on top of their own treatment."
Browne is convinced that digital pills can help people in developing countries with high rates of TB and HIV, though like Turner and Desai she cautions that patients' data must be protected. "I think it can be a tremendous technology for patient empowerment and I also think if properly used it can help the medical system to support patients that need it," she said. "But the absolute principle here is that the data has to belong to the patient."
Scientists search for a universal coronavirus vaccine
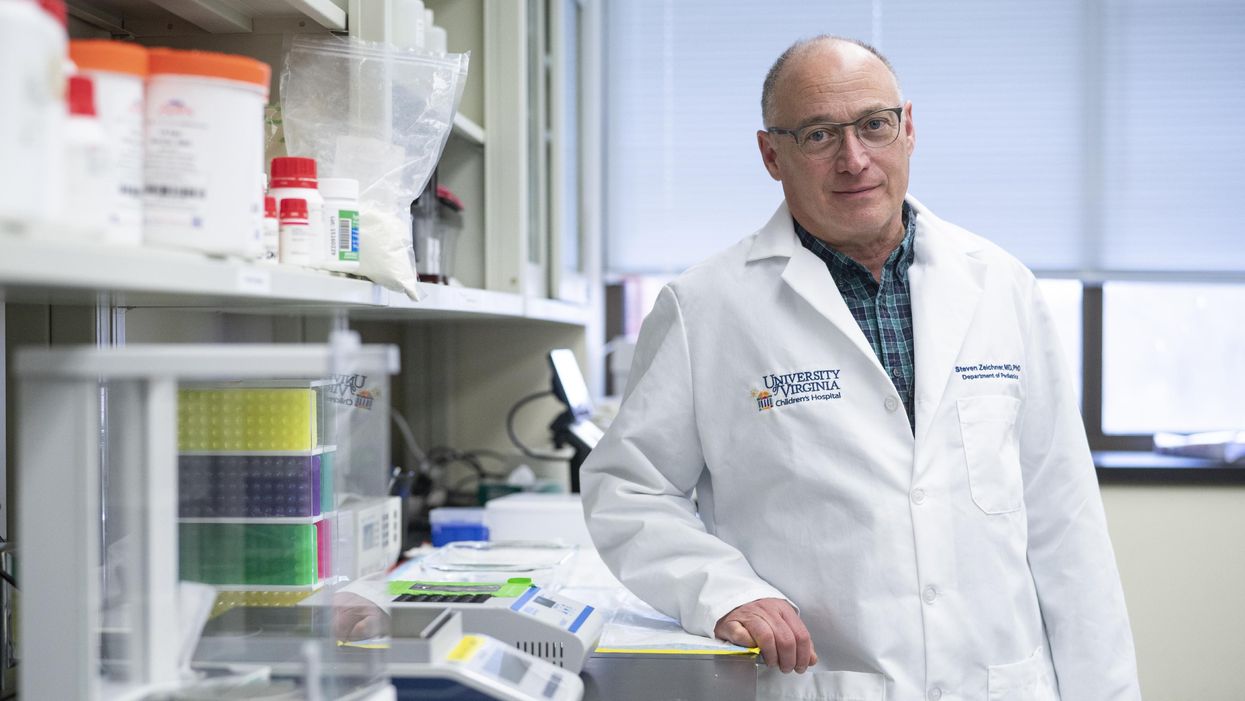
Stephen Zeichner, an infectious disease specialist at the University of Virginia Medical Center, has made progress with an early stage universal coronavirus vaccine.
The Covid-19 pandemic had barely begun when VBI Vaccines, a biopharmaceutical company based in Cambridge, Massachusetts, initiated their search for a universal coronavirus vaccine.
It was March 2020, and while most pharmaceutical companies were scrambling to initiate vaccine programs which specifically targeted the SARS-CoV-2 virus, VBI’s executives were already keen to look at the broader picture.
Having observed the SARS and MERS coronavirus outbreaks over the last two decades, Jeff Baxter, CEO of VBI Vaccines, was aware that SARS-CoV-2 is unlikely to be the last coronavirus to move from an animal host into humans. “It's absolutely apparent that the future is to create a vaccine which gives more broad protection against not only pre-existing coronaviruses, but those that will potentially make the leap into humans in future,” says Baxter.
It was a prescient decision. Over the last two years, more biotechs and pharma companies have joined the search to find a vaccine which might be able to protect against all coronaviruses, along with dozens of academic research groups. Last September, the US National Institutes of Health dedicated $36 million specifically to pan-coronavirus vaccine research, while the global Coalition for Epidemic Preparedness Innovations (CEPI) has earmarked $200 million towards the effort.
Until October 2021, the very concept of whether it might be
theoretically possible to vaccinate against multiple coronaviruses remained an open question. But then a groundbreaking study renewed optimism.
The emergence of new variants of Covid-19 over the past year, particularly the highly mutated Omicron variant, has added greater impetus to find broader spectrum vaccines. But until October 2021, the very concept of whether it might be theoretically possible to vaccinate against multiple coronaviruses remained an open question. After all, scientists have spent decades trying to develop a similar vaccine for influenza with little success.
But then a groundbreaking study from renowned virologist Linfa Wang, who runs the emerging infectious diseases program at Duke-National University of Singapore Medical School, provided renewed optimism.
Wang found that eight SARS survivors who had been injected with the Pfizer/BioNTech Covid-19 vaccine had neutralising antibodies in their blood against SARS, the Alpha, Beta and Delta variants of SARS-CoV-2, and five other coronaviruses which reside in bats and pangolins. He concluded that the combination of past coronavirus infection, and immunization with a messenger RNA vaccine, had resulted in a wider spectrum of protection than might have been expected.
“This is a significant study because it showed that pre-existing immunity to one coronavirus could help with the elicitation of cross-reactive antibodies when immunizing with a second coronavirus,” says Kevin Saunders, Director of Research at the Duke Human Vaccine Institute in North Carolina, which is developing a universal coronavirus vaccine. “It provides a strategy to perhaps broaden the immune response against coronaviruses.”
In the next few months, some of the first data is set to emerge looking at whether this kind of antibody response could be elicited by a single universal coronavirus vaccine. In April 2021, scientists at the Walter Reed Army Institute of Research in Silver Spring, Maryland, launched a Phase I clinical trial of their vaccine, with a spokesman saying that it was successful, and the full results will be announced soon.
The Walter Reed researchers have already released preclinical data, testing the vaccine in non-human primates where it was found to have immunising capabilities against a range of Covid-19 variants as well as the original SARS virus. If the Phase I trial displays similar efficacy, a larger Phase II trial will begin later this year.
Two different approaches
Broadly speaking, scientists are taking two contrasting approaches to the task of finding a universal coronavirus vaccine. The Walter Reed Army Institute of Research, VBI Vaccines – who plan to launch their own clinical trial in the summer – and the Duke Human Vaccine Institute – who are launching a Phase I trial in early 2023 – are using a soccer-ball shaped ferritin nanoparticle studded with different coronavirus protein fragments.
VBI Vaccines is looking to elicit broader immune responses by combining SARS, SARS-CoV-2 and MERS spike proteins on the same nanoparticle. Dave Anderson, chief scientific officer at VBI Vaccines, explains that the idea is that by showing the immune system these three spike proteins at the same time, it can help train it to identify and respond to subtle differences between coronavirus strains.
The Duke Human Vaccine Institute is utilising the same method, but rather than including the entire spike proteins from different coronaviruses, they are only including the receptor binding domain (RBD) fragment from each spike protein. “We designed our vaccine to focus the immune system on a site of vulnerability for the virus, which is the receptor binding domain,” says Saunders. “Since the RBD is small, arraying multiple RBDs on a nanoparticle is a straight-forward approach. The goal is to generate immunity to many different subgenuses of viruses so that there will be cross-reactivity with new or unknown coronaviruses.”
But the other strategy is to create a vaccine which contains regions of the viral protein structure which are conserved between all coronavirus strains. This is something which scientists have tried to do for a universal influenza vaccine, but it is thought to be more feasible for coronaviruses because they mutate at a slower rate and are more constrained in the ways that they can evolve.
DIOSynVax, a biotech based in Cambridge, United Kingdom, announced in a press release earlier this month that they are partnering with CEPI to use their computational predictive modelling techniques to identify common structures between all of the SARS coronaviruses which do not mutate, and thus present good vaccine targets.
Stephen Zeichner, an infectious disease specialist at the University of Virginia Medical Center, has created an early stage vaccine using the fusion peptide region – another part of the coronavirus spike protein that aids the virus’s entry into host cells – which so far appears to be highly conserved between all coronaviruses.
So far Zeichner has trialled this version of the vaccine in pigs, where it provided protection against a different coronavirus called porcine epidemic diarrhea virus, which he described as very promising as this virus is from a different family called alphacoronaviruses, while SARS-CoV-2 is a betacoronavirus.
“If a betacoronavirus fusion peptide vaccine designed from SARS-CoV-2 can protect pigs against clinical disease from an alphacoronavirus, then that suggests that an analogous vaccine would enable broad protection against many, many different coronaviruses,” he says.
The road ahead
But while some of the early stage results are promising, researchers are fully aware of the scale of the challenge ahead of them. Although CEPI have declared an aim of having a licensed universal coronavirus vaccine available by 2024-2025, Zeichner says that such timelines are ambitious in the extreme.
“I was incredibly impressed at the speed at which the mRNA coronavirus vaccines were developed for SARS-CoV-2,” he says. “That was faster than just about anybody anticipated. On the other hand, I think a universal coronavirus vaccine is more equivalent to the challenge of developing an HIV vaccine and we're 35 years into that effort without success. We know a lot more now than before, and maybe it will be easier than we think. But I think the route to a universal vaccine is harder than an individual vaccine, so I wouldn’t want to put money on a timeline prediction.”
The major challenge for scientists is essentially designing a vaccine for a future threat which is not even here yet. As such, there are no guidelines on what safety data would be required to license such a vaccine, and how researchers can demonstrate that it truly provides efficacy against all coronaviruses, even those which have not yet jumped to humans.
The teams working on this problem have already devised some ingenious ways of approaching the challenge. VBI Vaccines have taken the genetic sequences of different coronaviruses found in bats and pangolins, from publicly available databases, and inserted them into what virologists call a pseudotype virus – one which has been engineered so it does not have enough genetic material to replicate.
This has allowed them to test the neutralising antibodies that their vaccine produces against these coronaviruses in test tubes, under safe lab conditions. “We have literally just been ordering the sequences, and making synthetic viruses that we can use to test the antibody responses,” says Anderson.
However, some scientists feel that going straight to a universal coronavirus vaccine is likely to be too complex. Instead they say that we should aim for vaccines which are a little more specific. Pamela Bjorkman, a structural biologist at the California Institute of Technology, suggests that pan-coronavirus vaccines which protect against SARS-like betacoronaviruses such as SARS or SARS-CoV-2, or MERS-like betacoronaviruses, may be more realistic.
“I think a vaccine to protect against all coronaviruses is likely impossible since there are so many varieties,” she says. “Perhaps trying to narrow down the scope is advisable.”
But if the mission to develop a universal coronavirus vaccine does succeed, it will be one of the most remarkable feats in the annals of medical science. In January, US chief medical advisor Anthony Fauci urged for greater efforts to be devoted towards this goal, one which scientists feel would be the biological equivalent of the race to develop the first atomic bomb
“The development of an effective universal coronavirus vaccine would be equally groundbreaking, as it would have global applicability and utility,” says Saunders. “Coronaviruses have caused multiple deadly outbreaks, and it is likely that another outbreak will occur. Having a vaccine that prevents death from a future outbreak would be a tremendous achievement in global health.”
He agrees that it will require creativity on a remarkable scale: “The universal coronavirus vaccine will also require ingenuity and perseverance comparable to that needed for the Manhattan project.”
This month, Matt Fuchs becomes the new Editor-in-Chief of Leaps.org.
This month, Kira Peikoff passes the torch to me as editor-in-chief of Leaps.org. I’m excited to assume leadership of this important platform.
Leaps.org caught my eye back in 2018. I was in my late 30s and just starting to wake up to the reality that the people I care most about were getting older and more vulnerable to health problems. At the same time, three critical shifts were becoming impossible to ignore. First, the average age in the U.S. is getting older, a trend known as the “gray tsunami.” Second, healthcare expenses are escalating and becoming unsustainable. And third, our sedentary, stress-filled lifestyles are leading to devastating consequences.
These trends pointed to a future filled with disease, suffering and economic collapse. But whenever I visited Leaps.org, my outlook turned from gloomy to solution-oriented. I became just as fascinated in a fourth trend, one that stands to revolutionize our world: rapid, mind-bending innovations in health and medicine.
Brain atlases, genome sequencing and editing, AI, protein mapping, synthetic biology, 3-D printing—these technologies are yielding new opportunities for health, longevity and human thriving. COVID-19 has caused many setbacks, but it has accelerated scientific breakthroughs. History suggests we will see even more innovation—in digital health and virtual first care, for example—after the pandemic.
In 2020, I began covering these developments with articles for Leaps.org about clocks that measure biological aging, gene therapies for cystic fibrosis, and other seemingly futuristic concepts that are transforming the present. I wrote about them partly because I think most people aren’t aware of them—and meaningful progress can’t happen without public engagement. A broader set of stakeholders and society at large, not just the experts, must inform these changes to ensure that they reflect our values and ethics. Everyone should get the chance to participate in the conversation—and they must have the opportunity to benefit equally from the innovations we decide to move forward with. By highlighting cutting-edge advances, Leaps.org is helping to realize this important goal.
Meanwhile, as I wrote freelance pieces on health and wellness for outlets such as the Washington Post and Time Magazine, I kept seeing an intersect between the breakthroughs in research labs and our expanding knowledge about the science of well-being. Take, for example, emerging technologies designed to stop illnesses in their tracks and new research on the benefits of taking in natural daylight. These two areas, lab innovations and healthy lifestyles, both shift the focus from disease treatment to disease prevention and optimal health. It’s the only sensible, financially feasible way forward.
When Kira suggested that I consider a leadership role with Leaps.org, it struck me how much the platform’s ideals have informed my own perspectives. The frontpage gore of mainstream media outlets can feel like a daily dose of pessimism, with cynicism sometimes dressed up as wisdom. Leaps.org’s world view is rooted in something very different: rational optimism about the present moment and the possibility of human flourishing.
That’s why I’m proud to lead this platform, including our podcast, Making Sense of Science, and hope you’ll keep coming to Leaps.org to learn and join the conversation about scientific gamechangers through our sponsored events, our popular Instagram account and other social channels. Think critically about the breakthroughs and their ethical challenges. Help usher in the health and prosperity that could be ours if we stay open-minded to it.
Yours truly,
Matt Fuchs
Editor-in-Chief