

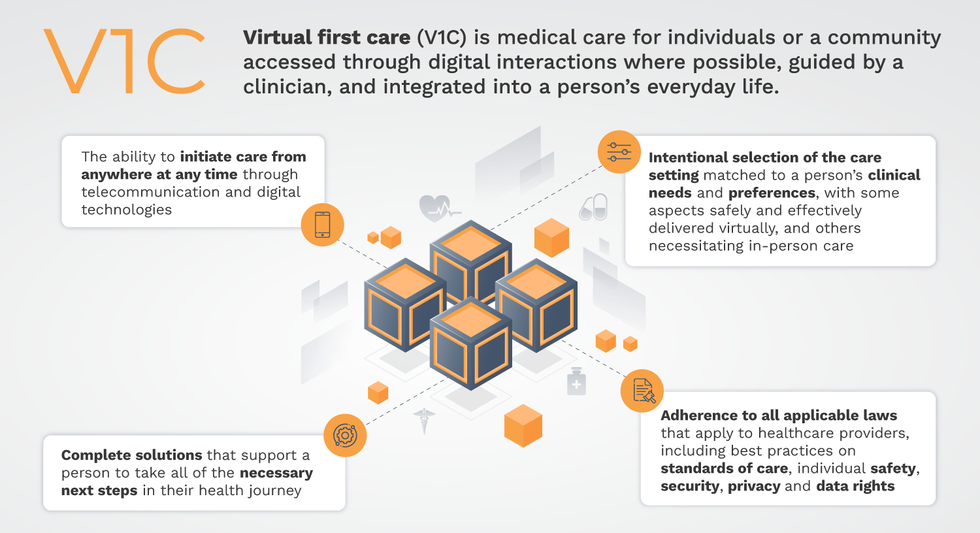
Virtual-first care, or V1C, could increase the quality of healthcare and make it more patient-centric by letting patients combine in-person visits with virtual options such as video for seeing their care providers.
That’s the idea behind virtual-first care (V1C), a new care model centered on convenient, customized, high-quality care that integrates a full suite of services tailored directly to patients’ clinical needs and preferences. This package includes asynchronous communication such as texting; video and other live virtual modes; and in-person options.
V1C goes beyond what you might think of as standard “telehealth” by using evidence-based protocols and tools that include traditional and digital therapeutics and testing, personalized care plans, dynamic patient monitoring, and team-based approaches to care. This could include spit kits mailed for laboratory tests and complementing clinical care with health coaching. V1C also replaces some in-person exams with ongoing monitoring, using sensors for more ‘whole person’ care.
Amidst all this momentum, we have the opportunity to rethink the goals of healthcare innovation, but that means bringing together key stakeholders to demonstrate that sustainable V1C can redefine healthcare.
Established V1C healthcare providers such as Omada, Headspace, and Heartbeat Health, as well as emerging market entrants like Oshi, Visana, and Wellinks, work with a variety of patients who have complicated long-term conditions such as diabetes, heart failure, gastrointestinal illness, endometriosis, and COPD. V1C is comprehensive in ways that are lacking in digital health and its other predecessors: it has the potential to integrate multiple data streams, incorporate more frequent touches and check-ins over time, and manage a much wider range of chronic health conditions, improving lives and reducing disease burden now and in the future.
Recognizing the pandemic-driven interest in virtual care, significant energy and resources are already flowing fast toward V1C. Some of the world’s largest innovators jumped into V1C early on: Verily, Alphabet’s Life Sciences Company, launched Onduo in 2016 to disrupt the diabetes healthcare market, and is now well positioned to scale its solutions. Major insurers like Aetna and United now offer virtual-first plans to members, responding as organizations expand virtual options for employees. Amidst all this momentum, we have the opportunity to rethink the goals of healthcare innovation, but that means bringing together key stakeholders to demonstrate that sustainable V1C can redefine healthcare.
That was the immediate impetus for IMPACT, a consortium of V1C companies, investors, payers and patients founded last year to ensure access to high-quality, evidence-based V1C. Developed by our team at the Digital Medicine Society (DiMe) in collaboration with the American Telemedicine Association (ATA), IMPACT has begun to explore key issues that include giving patients more integrated experiences when accessing both virtual and brick-and-mortar care.
Digital Medicine Society
V1C is not, nor should it be, virtual-only care. In this new era of hybrid healthcare, success will be defined by how well providers help patients navigate the transitions. How do we smoothly hand a patient off from an onsite primary care physician to, say, a virtual cardiologist? How do we get information from a brick-and-mortar to a digital portal? How do you manage dataflow while still staying HIPAA compliant? There are many complex regulatory implications for these new models, as well as an evolving landscape in terms of privacy, security and interoperability. It will be no small task for groups like IMPACT to determine the best path forward.
None of these factors matter unless the industry can recruit and retain clinicians. Our field is facing an unprecedented workforce crisis. Traditional healthcare is making clinicians miserable, and COVID has only accelerated the trend of overworked, disenchanted healthcare workers leaving in droves. Clinicians want more interactions with patients, and fewer with computer screens – call it “More face time, less FaceTime.” No new model will succeed unless the industry can more efficiently deploy its talent – arguably its most scarce and precious resource. V1C can help with alleviating the increasing burden and frustration borne by individual physicians in today’s status quo.
In healthcare, new technological approaches inevitably provoke no shortage of skepticism. Past lessons from Silicon Valley-driven fixes have led to understandable cynicism. But V1C is a different breed of animal. By building healthcare around the patient, not the clinic, V1C can make healthcare work better for patients, payers and providers. We’re at a fork in the road: we can revert back to a broken sick-care system, or dig in and do the hard work of figuring out how this future-forward healthcare system gets financed, organized and executed. As a field, we must find the courage and summon the energy to embrace this moment, and make it a moment of change.

Sparklers produce a beautiful display of light and heat by burning metal dust, which contains iron. The recent work of Canadian and Dutch researchers suggests we can use iron as a cheap, carbon-free fuel.
Iron as a fuel
Iron is abundantly available and cheap. More importantly, the byproduct of burning iron is rust (iron oxide), a solid material that is easy to collect and recycle. Neither burning iron nor converting its oxide back produces any carbon in the process.
Iron oxide is potentially renewable by reacting with electricity or hydrogen to become iron again.
Iron has a high energy density: it requires almost the same volume as gasoline to produce the same amount of energy. However, iron has poor specific energy: it’s a lot heavier than gas to produce the same amount of energy. (Think of picking up a jug of gasoline, and then imagine trying to pick up a similar sized chunk of iron.) Therefore, its weight is prohibitive for many applications. Burning iron to run a car isn’t very practical if the iron fuel weighs as much as the car itself.
In its powdered form, however, iron offers more promise as a high-density energy carrier or storage system. Iron-burning furnaces could provide direct heat for industry, home heating, or to generate electricity.
Plus, iron oxide is potentially renewable by reacting with electricity or hydrogen to become iron again (as long as you’ve got a source of clean electricity or green hydrogen). When there’s excess electricity available from renewables like solar and wind, for example, rust could be converted back into iron powder, and then burned on demand to release that energy again.
However, these methods of recycling rust are very energy intensive and inefficient, currently, so improvements to the efficiency of burning iron itself may be crucial to making such a circular system viable.
The science of discrete burning
Powdered particles have a high surface area to volume ratio, which means it is easier to ignite them. This is true for metals as well.
Under the right circumstances, powdered iron can burn in a manner known as discrete burning. In its most ideal form, the flame completely consumes one particle before the heat radiating from it combusts other particles in its vicinity. By studying this process, researchers can better understand and model how iron combusts, allowing them to design better iron-burning furnaces.
Discrete burning is difficult to achieve on Earth. Perfect discrete burning requires a specific particle density and oxygen concentration. When the particles are too close and compacted, the fire jumps to neighboring particles before fully consuming a particle, resulting in a more chaotic and less controlled burn.
Presently, the rate at which powdered iron particles burn or how they release heat in different conditions is poorly understood. This hinders the development of technologies to efficiently utilize iron as a large-scale fuel.
Burning metal in microgravity
In April, the European Space Agency (ESA) launched a suborbital “sounding” rocket, carrying three experimental setups. As the rocket traced its parabolic trajectory through the atmosphere, the experiments got a few minutes in free fall, simulating microgravity.
One of the experiments on this mission studied how iron powder burns in the absence of gravity.
In microgravity, particles float in a more uniformly distributed cloud. This allows researchers to model the flow of iron particles and how a flame propagates through a cloud of iron particles in different oxygen concentrations.
Existing fossil fuel power plants could potentially be retrofitted to run on iron fuel.
Insights into how flames propagate through iron powder under different conditions could help design much more efficient iron-burning furnaces.
Clean and carbon-free energy on Earth
Various businesses are looking at ways to incorporate iron fuels into their processes. In particular, it could serve as a cleaner way to supply industrial heat by burning iron to heat water.
For example, Dutch brewery Swinkels Family Brewers, in collaboration with the Eindhoven University of Technology, switched to iron fuel as the heat source to power its brewing process, accounting for 15 million glasses of beer annually. Dutch startup RIFT is running proof-of-concept iron fuel power plants in Helmond and Arnhem.
As researchers continue to improve the efficiency of burning iron, its applicability will extend to other use cases as well. But is the infrastructure in place for this transition?
Often, the transition to new energy sources is slowed by the need to create new infrastructure to utilize them. Fortunately, this isn’t the case with switching from fossil fuels to iron. Since the ideal temperature to burn iron is similar to that for hydrocarbons, existing fossil fuel power plants could potentially be retrofitted to run on iron fuel.
This article originally appeared on Freethink, home of the brightest minds and biggest ideas of all time.


Leaps.org talks with Dr. Tom Oxley, founding CEO of Synchron, a company that's taking a unique - and less invasive - approach to "brain-computer interfaces" for patients with ALS and other mobility challenges.
Listen on Apple | Listen on Spotify | Listen on Stitcher | Listen on Amazon | Listen on Google
In our conversation, Dr. Oxley talks about “Bluetooth brain”; the critical role of AI in the present and future of BCIs; how BCIs compare to voice command technology; regulatory frameworks for revolutionary technologies; specific people with paralysis who’ve been able to regain some independence thanks to the Stentrode; what it means to be a neurointerventionist; how to scale BCIs for more people to use them; the risks of BCIs malfunctioning; organic implants; and how BCIs help us understand the brain, among other topics.
Dr. Oxley received his PhD in neuro engineering from the University of Melbourne in Australia. He is the founding CEO of Synchron and an associate professor and the head of the vascular bionics laboratory at the University of Melbourne. He’s also a clinical instructor in the Deepartment of Neurosurgery at Mount Sinai Hospital. Dr. Oxley has completed more than 1,600 endovascular neurosurgical procedures on patients, including people with aneurysms and strokes, and has authored over 100 peer reviewed articles.
Links:
Synchron website - https://synchron.com/
Assessment of Safety of a Fully Implanted Endovascular Brain-Computer Interface for Severe Paralysis in 4 Patients (paper co-authored by Tom Oxley) - https://jamanetwork.com/journals/jamaneurology/art...
More research related to Synchron's work - https://synchron.com/research
Tom Oxley on LinkedIn - https://www.linkedin.com/in/tomoxl
Tom Oxley on Twitter - https://twitter.com/tomoxl?lang=en
Tom Oxley TED - https://www.ted.com/talks/tom_oxley_a_brain_implant_that_turns_your_thoughts_into_text?language=en
Tom Oxley website - https://tomoxl.com/
Novel brain implant helps paralyzed woman speak using digital avatar - https://engineering.berkeley.edu/news/2023/08/novel-brain-implant-helps-paralyzed-woman-speak-using-a-digital-avatar/
Edward Chang lab - https://changlab.ucsf.edu/
BCIs convert brain activity into text at 62 words per minute - https://med.stanford.edu/neurosurgery/news/2023/he...
Leaps.org: The Mind-Blowing Promise of Neural Implants - https://leaps.org/the-mind-blowing-promise-of-neural-implants/

Tom Oxley