
In an initial study, Canary analyzed speech recordings with AI and identified early stage Alzheimer’s with 96 percent accuracy.
Dave Arnold retired in his 60s and began spending time volunteering in local schools. But then he started misplacing items, forgetting appointments and losing his sense of direction. Eventually he was diagnosed with early stage Alzheimer’s.
“Hearing the diagnosis made me very emotional and tearful,” he said. “I immediately thought of all my mom had experienced.” His mother suffered with the condition for years before passing away. Over the last year, Arnold has worked for the Alzheimer’s Association as one of its early stage advisors, sharing his insights to help others in the initial stages of the disease.
Arnold was diagnosed sooner than many others. It's important to find out early, when interventions can make the most difference. One promising avenue is looking at how people talk. Research has shown that Alzheimer’s affects a part of the brain that controls speech, resulting in small changes before people show other signs of the disease.
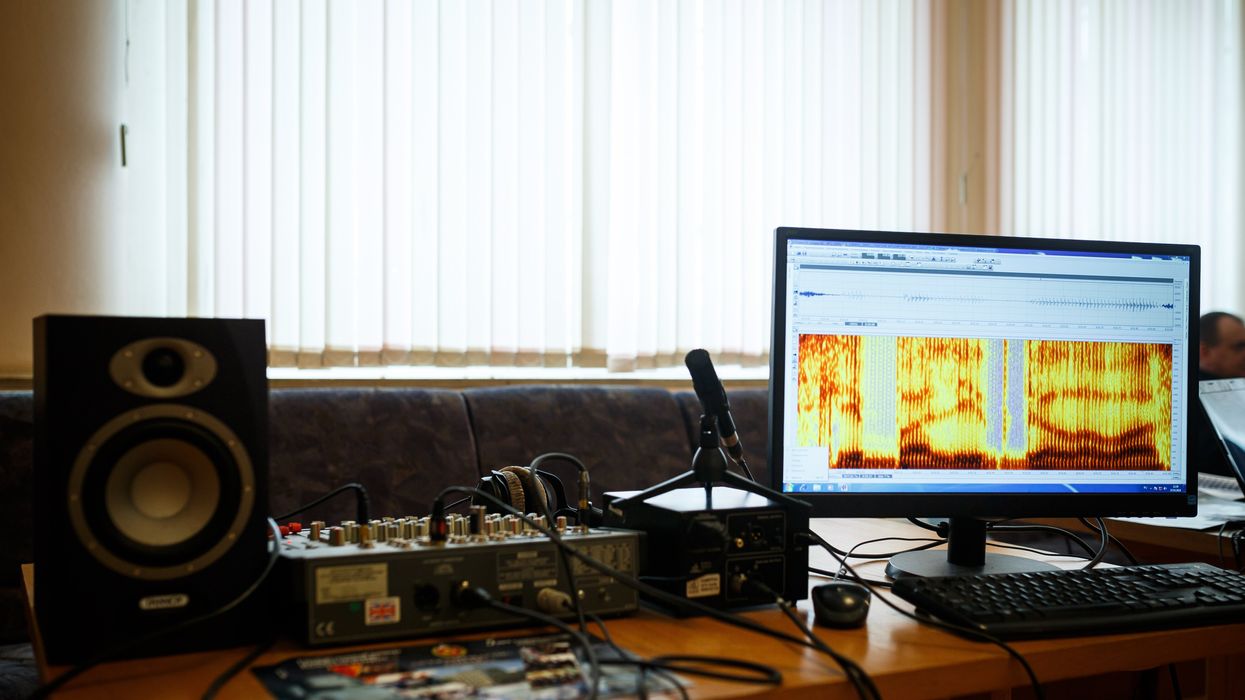
Now, Canary Speech, a company based in Utah, is using AI to examine elements like the pitch of a person’s voice and their pauses. In an initial study, Canary analyzed speech recordings with AI and identified early stage Alzheimer’s with 96 percent accuracy.
Developing the AI model
Canary Speech’s CEO, Henry O’Connell, met cofounder Jeff Adams about 40 years before they started the company. Back when they first crossed paths, they were both living in Bethesda, Maryland; O’Connell was a research fellow at the National Institutes of Health studying rare neurological diseases, while Adams was working to decode spy messages. Later on, Adams would specialize in building mathematical models to analyze speech and sound as a team leader in developing Amazon's Alexa.
It wasn't until 2015 that they decided to make use of the fit between their backgrounds. ““We established Canary Speech in 2017 to build a product that could be used in multiple languages in clinical environments,” O'Connell says.
The need is growing. About 55 million people worldwide currently live with Alzheimer’s, a number that is expected to double by 2050. Some scientists think the disease results from a buildup of plaque in the brain. It causes mild memory loss at first and, over time, this issue get worse while other symptoms, such as disorientation and hallucinations, can develop. Treatment to manage the disease is more effective in the earlier stages, but detection is difficult since mild symptoms are often attributed to the normal aging process.
O’Connell and Adams specialize in the complex ways that Alzheimer’s effects how people speak. Using AI, their mathematical model analyzes 15 million data points every minute, focusing on certain features of speech such as pitch, pauses and elongation of words. It also pays attention to how the vibrations of vocal cords change in different stages of the disease.
To create their model, the team used a type of machine learning called deep neural nets, which looks at multiple layers of data - in this case, the multiple features of a person’s speech patterns.
“Deep neural nets allow us to look at much, much larger data sets built out of millions of elements,” O’Connell explained. “Through machine learning and AI, we’ve identified features that are very sensitive to an Alzheimer’s patient versus [people without the disease] and also very sensitive to mild cognitive impairment, early stage and moderate Alzheimer's.” Based on their learnings, Canary is able to classify the disease stage very quickly, O’Connell said.
“When we’re listening to sublanguage elements, we’re really analyzing the direct result of changes in the brain in the physical body,” O’Connell said. “The brain controls your vocal cords: how fast they vibrate, the expansion of them, the contraction.” These factors, along with where people put their tongues when talking, function subconsciously and result in subtle changes in the sounds of speech.
Further testing is needed
In an initial trial, Canary analyzed speech recordings from phone calls to a large U.S. health insurer. They looked at the audio recordings of 651 policyholders who had early stage Alzheimer’s and 1018 who did not have the condition, aiming for a representative sample of age, gender and race. They used this data to create their first diagnostic model and found that it was 96 percent accurate in identifying Alzheimer’s.
Christian Herff, an assistant professor of neuroscience at Maastricht University in the Netherlands, praised this approach while adding that further testing is needed to assess its effectiveness.
“I think the general idea of identifying increased risk for cognitive impairment based on speech characteristics is very feasible, particularly when change in a user’s voice is monitored, for example, by recording speech every year,” Herff said. He noted that this can only be a first indication, not a full diagnosis. The accuracy still needs to be validated in studies that follows individuals over a period of time, he said.
Toby Walsh, a professor of artificial intelligence at the University of New South Wales, also thinks Canary’s tool has potential but highlights that Canary could diagnose some people who don’t really have the disease. “This is an interesting and promising application of AI,” he said, “but these tools need to be used carefully. Imagine the anxiety of being misdiagnosed with Alzheimer’s.”
As with many other AI tools, privacy and bias are additional issues to monitor closely, Walsh said.
Other languages
A related issue is that not everyone is fluent in English. Mahnaz Arvaneh, a senior lecturer in automatic control and systems engineering at the University of Sheffield, said this could be a blind spot.
“The system may not be very accurate for those who have English as their second language as their speaking patterns would be different, and any issue might be because of language deficiency rather than cognitive issues,” Arvaneh said.
The team is expanding to multiple languages starting with Japanese and Spanish. The elements of the model that make up the algorithm are very similar, but they need to be validated and retrained in a different language, which will require access to more data.
Recently, Canary analyzed the phone calls of 233 Japanese patients who had mild cognitive impairment and 704 healthy people. Using an English model they were able to identify the Japanese patients who had mild cognitive impairment with 78 percent accuracy. They also developed a model in Japanese that was 45 percent accurate, and they’re continuing to train it with more data.
The future
Canary is using their model to look at other diseases like Huntington’s and Parkinson’s. They’re also collaborating with pharmaceuticals to validate potential therapies for Alzheimer’s. By looking at speech patterns over time, Canary can get an indication of how well these drugs are working.

Dave Arnold and his wife dance at his nephew’s wedding in Rochester, New York, ten years ago, before his Alzheimer's diagnosis.
Dave Arnold
Ultimately, they want to integrate their tool into everyday life. “We want it to be used in a smartphone, or a teleconference call so that individuals could be examined in their home,” O’Connell said. “We could follow them over time and work with clinical teams and hospitals to improve the evaluation of patients and contribute towards an accurate diagnosis.”
Arnold, the patient with early stage Alzheimer’s, sees great promise. “The process of getting a diagnosis is already filled with so much anxiety,” he said. “Anything that can be done to make it easier and less stressful would be a good thing, as long as it’s proven accurate.”

Last month, a paper published in Cell by Harvard biologist David Sinclair explored root cause of aging, as well as examining whether this process can be controlled. We talked with Dr. Sinclair about this new research.
Show links:
Dr. Sinclair's paper, published last month in Cell.
Recent pre-print paper - not yet peer reviewed - showing that mice treated with Yamanaka factors lived longer than the control group.
Dr. Sinclair's podcast.
Previous research on aging and DNA mutations.
Dr. Sinclair's book, Lifespan.

Harvard Medical School
