
Who Qualifies as an “Expert” And How Can We Decide Who Is Trustworthy?

Discerning a real expert from a charlatan is crucial during the COVID-19 pandemic and beyond.
This article is part of the magazine, "The Future of Science In America: The Election Issue," co-published by LeapsMag, the Aspen Institute Science & Society Program, and GOOD.
Expertise is a slippery concept. Who has it, who claims it, and who attributes or yields it to whom is a culturally specific, sociological process. During the COVID-19 pandemic, we have witnessed a remarkable emergence of legitimate and not-so-legitimate scientists publicly claiming or being attributed to have academic expertise in precisely my field: infectious disease epidemiology. From any vantage point, it is clear that charlatans abound out there, garnering TV coverage and hundreds of thousands of Twitter followers based on loud opinions despite flimsy credentials. What is more interesting as an insider is the gradient of expertise beyond these obvious fakers.
A person's expertise is not a fixed attribute; it is a hierarchical trait defined relative to others. Despite my protestations, I am the go-to expert on every aspect of the pandemic to my family. To a reporter, I might do my best to answer a question about the immune response to SARS-CoV-2, noting that I'm not an immunologist. Among other academic scientists, my expertise is more well-defined as a subfield of epidemiology, and within that as a particular area within infectious disease epidemiology. There's a fractal quality to it; as you zoom in on a particular subject, a differentiation of expertise emerges among scientists who, from farther out, appear to be interchangeable.
We all have our scientific domain and are less knowledgeable outside it, of course, and we are often asked to comment on a broad range of topics. But many scientists without a track record in the field have become favorites among university administrators, senior faculty in unrelated fields, policymakers, and science journalists, using institutional prestige or social connections to promote themselves. This phenomenon leads to a distorted representation of science—and of academic scientists—in the public realm.
Trustworthy experts will direct you to others in their field who know more about particular topics, and will tend to be honest about what is and what isn't "in their lane."
Predictably, white male voices have been disproportionately amplified, and men are certainly over-represented in the category of those who use their connections to inappropriately claim expertise. Generally speaking, we are missing women, racial minorities, and global perspectives. This is not only important because it misrepresents who scientists are and reinforces outdated stereotypes that place white men in the Global North at the top of a credibility hierarchy. It also matters because it can promote bad science, and it passes over scientists who can lend nuance to the scientific discourse and give global perspectives on this quintessentially global crisis.
Also at work, in my opinion, are two biases within academia: the conflation of institutional prestige with individual expertise, and the bizarre hierarchy among scientists that attributes greater credibility to those in quantitative fields like physics. Regardless of mathematical expertise or institutional affiliation, lack of experience working with epidemiological data can lead to over-confidence in the deceptively simple mathematical models that we use to understand epidemics, as well as the inappropriate use of uncertain data to inform them. Prominent and vocal scientists from different quantitative fields have misapplied the methods of infectious disease epidemiology during the COVID-19 pandemic so far, creating enormous confusion among policymakers and the public. Early forecasts that predicted the epidemic would be over by now, for example, led to a sense that epidemiological models were all unreliable.
Meanwhile, legitimate scientific uncertainties and differences of opinion, as well as fundamentally different epidemic dynamics arising in diverse global contexts and in different demographic groups, appear in the press as an indistinguishable part of this general chaos. This leads many people to question whether the field has anything worthwhile to contribute, and muddies the facts about COVID-19 policies for reducing transmission that most experts agree on, like wearing masks and avoiding large indoor gatherings.
So how do we distinguish an expert from a charlatan? I believe a willingness to say "I don't know" and to openly describe uncertainties, nuances, and limitations of science are all good signs. Thoughtful engagement with questions and new ideas is also an indication of expertise, as opposed to arrogant bluster or a bullish insistence on a particular policy strategy regardless of context (which is almost always an attempt to hide a lack of depth of understanding). Trustworthy experts will direct you to others in their field who know more about particular topics, and will tend to be honest about what is and what isn't "in their lane." For example, some expertise is quite specific to a given subfield: epidemiologists who study non-infectious conditions or nutrition, for example, use different methods from those of infectious disease experts, because they generally don't need to account for the exponential growth that is inherent to a contagion process.
Academic scientists have a specific, technical contribution to make in containing the COVID-19 pandemic and in communicating research findings as they emerge. But the liminal space between scientists and the public is subject to the same undercurrents of sexism, racism, and opportunism that society and the academy have always suffered from. Although none of the proxies for expertise described above are fool-proof, they are at least indicative of integrity and humility—two traits the world is in dire need of at this moment in history.
[Editor's Note: To read other articles in this special magazine issue, visit the beautifully designed e-reader version.]
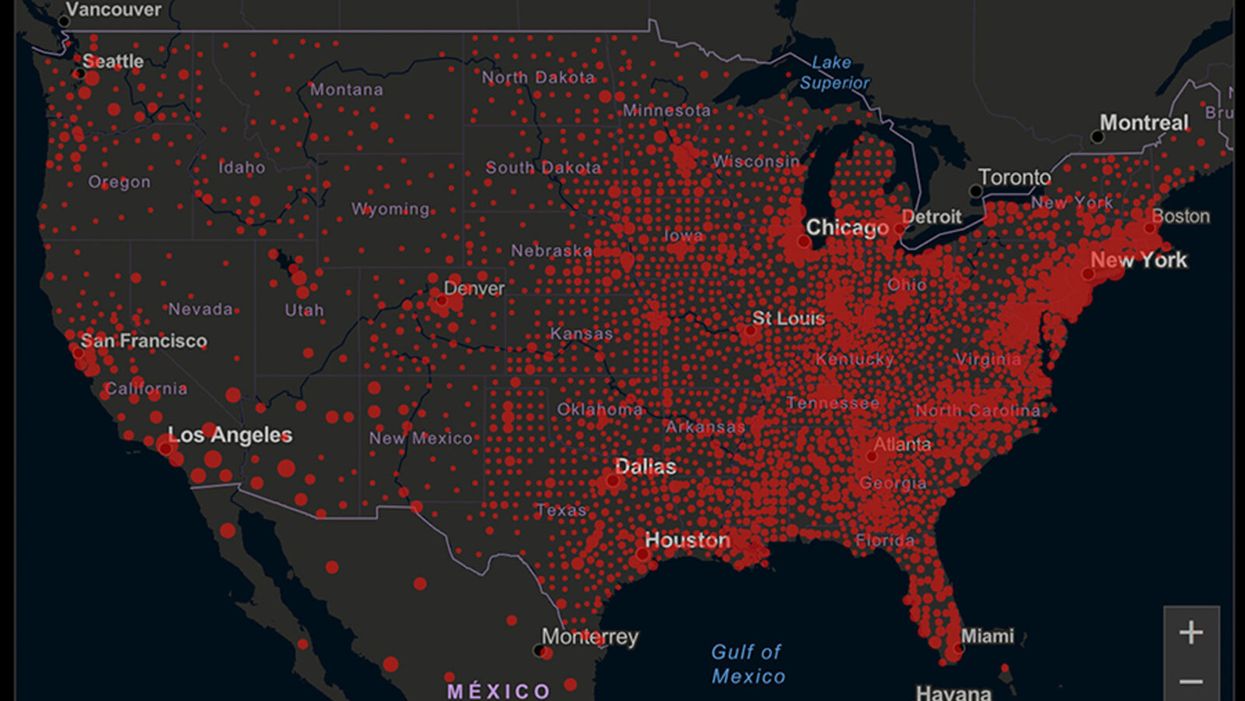
A map of cumulative known cases of COVID-19 in the U.S., as of June 12th, 2020.
Have you felt a bit like an armchair epidemiologist lately? Maybe you've been poring over coronavirus statistics on your county health department's website or on the pages of your local newspaper.
If the percentage of positive tests steadily stays under 8 percent, that's generally a good sign.
You're likely to find numbers and charts but little guidance about how to interpret them, let alone use them to make day-to-day decisions about pandemic safety precautions.
Enter the gurus. We asked several experts to provide guidance for laypeople about how to navigate the numbers. Here's a look at several common COVID-19 statistics along with tips about how to understand them.
Case Counts: Consider the Context
The number of confirmed COVID-19 cases in American counties is widely available. Local and state health departments should provide them online, or you can easily look them up at The New York Times' coronavirus database. However, you need to be cautious about interpreting them.
"Case counts are the obvious numbers to look at. But they're probably the hardest thing to sort out," said Dr. Jeff Martin, an epidemiologist at the University of California at San Francisco.
That's because case counts by themselves aren't a good window into how the coronavirus is affecting your community since they rely on testing. And testing itself varies widely from day to day and community to community.
"The more testing that's done, the more infections you'll pick up," explained Dr. F. Perry Wilson, a physician at Yale University. The numbers can also be thrown off when tests are limited to certain groups of people.
"If the tests are being mostly given to people with a high probability of having been infected -- for example, they have had symptoms or work in a high-risk setting -- then we expect lots of the tests to be positive. But that doesn't tell us what proportion of the general public is likely to have been infected," said Eleanor Murray, an epidemiologist at Boston University.
These Stats Are More Meaningful
According to Dr. Wilson, it's more useful to keep two other statistics in mind: the number of COVID tests that are being performed in your community and the percentage that turn up positive, showing that people have the disease. (These numbers may or may not be available locally. Check the websites of your community's health department and local news media outlets.)
If the number of people being tested is going up, but the percentage of positive tests is going down, Dr. Wilson said, that's a good sign. But if both numbers are going up – the number of people tested and the percentage of positive results – then "that's a sign that there are more infections burning in the community."
It's especially worrisome if the percentage of positive cases is growing compared to previous days or weeks, he said. According to him, that's a warning of a "high-risk situation."
Dr. George Rutherford, an epidemiologist at University of California at San Francisco, offered this tip: If the percentage of positive tests steadily stays under 8 percent, that's generally a good sign.
There's one more caveat about case counts. It takes an average of a week for someone to be infected with COVID-19, develop symptoms, and get tested, Dr. Rutherford said. It can take an additional several days for those test results to be reported to the county health department. This means that case numbers don't represent infections happening right now, but instead are a picture of the state of the pandemic more than a week ago.
Hospitalizations: Focus on Current Statistics
You should be able to find numbers about how many people in your community are currently hospitalized – or have been hospitalized – with diagnoses of COVID-19. But experts say these numbers aren't especially revealing unless you're able to see the number of new hospitalizations over time and track whether they're rising or falling. This number often isn't publicly available, however.
If new hospitalizations are increasing, "you may want to react by being more careful yourself."
And there's an important caveat: "The problem with hospitalizations is that they do lag," UC San Francisco's Dr. Martin said, since it takes time for someone to become ill enough to need to be hospitalized. "They tell you how much virus was being transmitted in your community 2 or 2.5 weeks ago."
Also, he said, people should be cautious about comparing new hospitalization rates between communities unless they're adjusted to account for the number of more-vulnerable older people.
Still, if new hospitalizations are increasing, he said, "you may want to react by being more careful yourself."
Deaths: They're an Even More Delayed Headline
Cable news networks obsessively track the number of coronavirus deaths nationwide, and death counts for every county in the country are available online. Local health departments and media websites may provide charts tracking the growth in deaths over time in your community.
But while death rates offer insight into the disease's horrific toll, they're not useful as an instant snapshot of the pandemic in your community because severely ill patients are typically sick for weeks. Instead, think of them as a delayed headline.
"These numbers don't tell you what's happening today. They tell you how much virus was being transmitted 3-4 weeks ago," Dr. Martin said.
'Reproduction Value': It May Be Revealing
You're not likely to find an available "reproduction value" for your community, but it is available for your state and may be useful.
A reproduction value, also known as R0 or R-naught, "tells us how many people on average we expect will be infected from a single case if we don't take any measures to intervene and if no one has been infected before," said Boston University's Murray.
As The New York Times explained, "R0 is messier than it might look. It is built on hard science, forensic investigation, complex mathematical models — and often a good deal of guesswork. It can vary radically from place to place and day to day, pushed up or down by local conditions and human behavior."
It may be impossible to find the R0 for your community. However, a website created by data specialists is providing updated estimates of a related number -- effective reproduction number, or Rt – for each state. (The R0 refers to how infectious the disease is in general and if precautions aren't taken. The Rt measures its infectiousness at a specific time – the "t" in Rt.) The site is at rt.live.
"The main thing to look at is whether the number is bigger than 1, meaning the outbreak is currently growing in your area, or smaller than 1, meaning the outbreak is currently decreasing in your area," Murray said. "It's also important to remember that this number depends on the prevention measures your community is taking. If the Rt is estimated to be 0.9 in your area and you are currently under lockdown, then to keep it below 1 you may need to remain under lockdown. Relaxing the lockdown could mean that Rt increases above 1 again."
"Whether they're on the upswing or downswing, no state is safe enough to ignore the precautions about mask wearing and social distancing."
Keep in mind that you can still become infected even if an outbreak in your community appears to be slowing. Low risk doesn't mean no risk.
Putting It All Together: Why the Numbers Matter
So you've reviewed COVID-19 statistics in your community. Now what?
Dr. Wilson suggests using the data to remind yourself that the coronavirus pandemic "is still out there. You need to take it seriously and continue precautions," he said. "Whether they're on the upswing or downswing, no state is safe enough to ignore the precautions about mask wearing and social distancing. 'My state is doing well, no one I know is sick, is it time to have a dinner party?' No."
He also recommends that laypeople avoid tracking COVID-19 statistics every day. "Check in once a week or twice a month to see how things are going," he suggested. "Don't stress too much. Just let it remind you to put that mask on before you get out of your car [and are around others]."
GOOD10: The Pandemic Issue explores big-picture ways that science innovation and communication can usher in a more equitable, more progress-oriented, and safer world.
This issue is a collaboration among GOOD, leapsmag, and the Aspen Institute Science & Society Program.
The GOOD10 format explores fundamental issues facing humanity through the lenses of ten forces pushing the needle toward progress: Places, Philanthropists, Celebrities, Whistleblowers, Companies, Media, Products, Politicians, Scientists, and Actions. Across these categories, we seek to present unexpected and encouraging paradigms emerging from this historic crisis.
This special issue is available as an e-reader version for both desktop and mobile. It is also available as a free downloadable PDF.
TABLE OF CONTENTS:
- PLACES:
55 Lessons Learned About Science Communication Around the World; Quarantining Our Way Into Outer Space - PLACES:
Quarantining Our Way Into Outer Space - PHILANTHROPISTS:
An Exclusive Interview with Wendy Schmidt about Science in the Pandemic Era - CELEBRITIES:
Neil deGrasse Tyson Wants Celebrities to Promote Scientists - WHISTLEBLOWERS:
The Science Sleuths Holding Fraudulent Research Accountable - COMPANIES:
The Biggest Challenge for a COVID-19 Vaccine: Making It Accessible and Affordable - MEDIA:
Isaac Asimov on the History of Infectious Disease—And How Humanity Learned To Fight Back - PRODUCTS:
Will COVID-19 Pave the Way For DIY Precision Medicine? - POLITICIANS:
Will the Pandemic Propel STEM Experts to Political Power? - SCIENTISTS:
Would a Broad-Spectrum Antiviral Drug Stop the Pandemic? - ACTIONS:
Pseudoscience is Rampant: How Not to Fall For It - ACTIONS:
How COVID-19 Could Usher In a New Age of Collective Drug Discovery
THE EVENT:
"The Pandemic Science Summit" focused on how science innovation is key to society's future stability as we emerge from the pandemic, featuring:

Christopher Bailey – Arts and Health Lead, World Health Organization

Elisabeth Bik, Ph.D. – Microbiologist and scientific integrity consultant

Margaret Hamburg, M.D. – Foreign Secretary, National Academy of Medicine; former Commissioner, U.S. Food and Drug Administration

Peggy Oti-Boateng, Ph.D. – Director, Division of Science Policy and Capacity- Building, UNESCO

George Yancopoulos, M.D., Ph.D. – President and Chief Scientific Officer, Regeneron Pharmaceuticals
Kira Peikoff was the editor-in-chief of Leaps.org from 2017 to 2021. As a journalist, her work has appeared in The New York Times, Newsweek, Nautilus, Popular Mechanics, The New York Academy of Sciences, and other outlets. She is also the author of four suspense novels that explore controversial issues arising from scientific innovation: Living Proof, No Time to Die, Die Again Tomorrow, and Mother Knows Best. Peikoff holds a B.A. in Journalism from New York University and an M.S. in Bioethics from Columbia University. She lives in New Jersey with her husband and two young sons. Follow her on Twitter @KiraPeikoff.