


The White House in Washington, D.C.
















Randy W. Schekman, Ph.D.
2013 Nobel Laureate in Physiology or Medicine

George F. Smoot, Ph.D.
2006 Nobel Laureate in Physics

Thomas C. Südhof, M.D.
2013 Nobel Laureate for Physiology or Medicine
Warren M. Washington, Ph.D.
2009 National Medal of Science Laureate

Carl Wieman, Ph.D.
2001 Nobel Laureate in Physics
Dear Mr. President:
Peter Agre, M.D.
- Bloomberg Distinguished Professor and Director
- Johns Hopkins Malaria Research Institute
- 2003 Nobel Laureate in Chemistry
David Baker, Ph.D.
- Henrietta and Aubrey Davis Endowed Professor in Biochemistry
- University of Washington
- Investigator, Howard Hughes Medical Institute
- 2021 Breakthrough Prize in Life Sciences Laureate
I encourage you most strongly to ramp up support for basic science research in the U.S.! Discoveries can have impact far beyond the original questions being investigated, as highlighted by the recent Nobel prizes for CRISPR/Cas9. In my own research area, investigation of the fundamental principles of protein folding led to our ability to use computers to rapidly design promising vaccine, therapeutic, and diagnostic candidates in the midst of the pandemic. I also encourage you to support work on general pandemic preparedness, as with increasing population density, new pathogen outbreaks are likely to continue, and having effective countermeasures in place would greatly reduce human suffering and economic damage.
- - - - - - - - -
Cori Bargmann, Ph.D.

- Torsten W. Wiesel Professor
- Rockefeller University
- Head of Science, Chan Zuckerberg Initiative
- 2013 Breakthrough Prize in Life Sciences Laureate
Find all the pathogens!
To prevent and manage infectious disease, the next administration should deploy the power of large-scale molecular analysis to build a new, shared infrastructure for public health.
Currently, we identify infectious agents—viruses, bacteria, parasites, fungi—one by one at the local level. Is norovirus causing gastrointestinal distress in preschool children? Does a hospital harbor antibiotic-resistant bacteria like MRSA? Is a nursing home incubating Candida auris, a fungal superbug? We shouldn't be asking these questions one at a time. Instead, deploying large-scale molecular analysis would allow an integrated public health system to monitor all infectious diseases in real time and share the data nationwide.
First, provide DNA sequencing capacity for all local and state public health systems. Rapid, inexpensive sequencing of infectious agents should be routine whenever an outbreak occurs in a workplace, hospital, school, or prison. It can be used to track spread between people, find contaminated environments, and identify sites where a swift intervention is needed. Routine sequencing of infectious agents enables a quick, effective, and targeted public health response.
Second, use molecular methods like PCR and sequencing to track disease-causing viruses, bacteria, parasites, or fungi nationwide. In a science-informed world, we should know exactly what's making us sick. This is not primarily a health-care issue: most of the time putting a name on the organism won't change treatment. It's a public health mission: to identify dangerous infectious agents early, while there's time to act. Most of the time a respiratory infection (for example) will harbor a common rhinovirus or influenza virus, but sometimes those will not be present. In those cases, the advanced DNA sequencing method called metagenomics can identify unexpected and even previously unknown organisms, like SARS-CoV-2 in 2019. By monitoring all infectious agents systematically, we can be aware of their prevalence, spread, and virulence, and we can be prepared before the next pandemic occurs.
Finally, we need a national public health data infrastructure to share all of this information—the sequence of the infectious agent, the location at which it was found, and the disease that it caused. A common, shared data system will let infectious disease experts find and stop the next outbreak that endangers us all.
- - - - - - - - -
Jacqueline K. Barton, Ph.D.

- John G. Kirkwood and Arthur A. Noyes Professor of Chemistry
- California Institute of Technology
- 2010 National Medal of Science Laureate
A critically important resource in America today is our scientific enterprise. We bring together the best and brightest and create new technologies, new medicines, new ways of living. Our scientific enterprise is critical to the health and growth of our economy, whether considering our energy industry, biotechnology, pharma, or computer technologies. And as we consider the great global challenges before us, climate change and global health, here, too, science holds the answers.
For more than fifty years, the U.S. has been the global center of scientific excellence. Our universities have provided the best in the world for research and exploration. And in contrast to universities elsewhere, our universities provide a structure that nurtures change. Assistant professors can start up their own labs, raise funds to support their new experiments, and discover quickly new ideas as to how the world works. Our industrial enterprise supports this same entrepreneurial approach to explore and develop. Small start-ups are incubators for transformative technologies. Moreover, collaboration, across disciplines and between industry and academe, allows a mixing of new ideas. And with federal support, both academic and industrial research can quickly yield new technologies and economic growth.
Science in the U.S. is therefore a unique and critical strength. Yet science is under attack. We have been able to attract the very best from across the globe to train here, to learn from the best and spread the word. This cross fertilization will not occur going forward if we squelch immigration and if we interfere with international collaboration. Moreover, research in our universities requires federal funding. Without support for basic research, where we are just learning the questions, let alone the answers, we can only make progress incrementally, and we cannot discover and develop new, transformative technologies.
U.S. science is a jewel. It needs your support.
- - - - - - - - -
Barry Barish, Ph.D.
- Linde Professor of Physics, Emeritus
- California Institute of Technology
- 2017 Nobel Laureate in Physics
I am writing to stress to the new administration that you will soon be faced with crucial policy issues that require good scientific input in formulating policy. At the top of list must be providing the leadership that will bring us out of the pandemic. In that regard, formulating consistent policy on social distancing, testing and tracing, and vaccines and distribution are all complex problems that need the best scientific inputs and advice.
A second issue of great importance to the world is nuclear proliferation. We must make viable agreements with other countries having nuclear capability, as well as agreements for Iran or other countries that could develop capability. Renewing the U.S. nuclear stockpile is a very complex domestic issue that again needs the best scientific guidance.
A third crucial issue is climate change. We have had unprecedented heat, melting ice caps, forest fires, polluted cities, etc. in the recent past. We must develop forward-looking and workable policy, working with the rest of the world and using the best advice of scientists.
Of course, there will be other major issues, where the advice of scientists will be crucial to decision making and formulating policies. The U.S. is a wonderful place to be a scientist and to do science. Please take advantage of our skills and knowledge as you face the challenges of the coming years.
- - - - - - - - -
May Berenbaum, Ph.D.

- Professor and Head of Entomology
- University of Illinois at Urbana–Champaign
- 2012 National Medal of Science Laureate
Congratulations on your election, during a moment in history when the health and well-being not only of the human population but also the biodiversity of the planet will almost certainly be affected by decisions you make while you're in office. For this reason, please depend on the knowledge that the scientific community can offer to inform your decision-making. In 1863, your predecessor Abraham Lincoln, recognizing the need for independent, objective advice for a nation embroiled in a civil war, created the National Academy of Sciences as a mechanism to obtain such advice. Scientists answered the call, advising the federal government on many scientific and technological issues, including consistency across weights and measures and accuracy of magnetic compass readings on iron-hulled warships. For over 150 years, the federal government has benefited from making decisions based on the best independent, objective scientific evidence available from a rapidly expanding community of scientists. Keep in mind, though, that scientific research comprises not just the knowledge produced, but also the process through which it's obtained, a process designed to be iterative, self-correcting, and objective. It's true that scientific views can change, sometimes rapidly—but such change is intrinsic to the process, as long as changes come not from whimsy or political stratagems, but from the collective accumulation of well-designed, unbiased, repeatable studies, particularly when new fields or unprecedented problems arise. The utility of relying on scientific advice in policy-making has been abundantly demonstrated, as have the often tragic consequences of rejecting a strong scientific consensus to suit political agendas (think of the deaths of millions resulting from the Soviet-era implementation of Trofim Lysenko's politically tinged agronomic theories). Like it or not, your legacy will depend on the extent to which you embrace both the process and the products of the scientific enterprise.
- - - - - - - - -
Martin Chalfie, Ph.D.
- University Professor of Biological Sciences
- Columbia University
- 2008 Nobel Laureate in Chemistry
I have never been prouder of the scientific enterprise than during the COVID-19 pandemic. Scientists, healthcare professionals, and others are devoting their knowledge and skills and often redirecting their research to solve the problems of SARS-CoV-2 and the destruction it is causing. These scientific efforts would not have been possible without our previous understanding of basic biological processes. This understanding is what allows people to sequence genomes, determine protein structures, develop novel ways of detecting and interfering with the virus, and understand how viruses take over cells and how the body responds to infection. As part of preparedness for the next health crisis, we must continue to build our scientific knowledge, because we do not know what we will need to know.
The astonishing response of the scientific community to this pandemic shows how much science can contribute and what it can accomplish. The question for the future is: how can we maintain our momentum? We can do so, first, by increasing the support for both fundamental and applied research, and we need to take a broad view of what to support. I received my Nobel Prize for my development of a method to watch cells work that was based on a jellyfish protein. Tens of thousands of research projects have utilized this protein to expand our understanding of basic biology and to study human disease. Second, we need to put more resources into educating future scientists. We must support and expand STEM programs in elementary and high schools, research opportunities for college students, and training programs for graduate students and postdoctoral researchers. And we must provide opportunities to increase diversity within the sciences, including encouraging and supporting the entry of underrepresented minorities and first-generation, low-income college students into careers in the sciences. Third, we should ensure that governmental decisions and administrative policies are based on strong scientific consensus and are not subjected to anti-science political pressure. We have a long tradition of the sciences and scientists helping our country. Indeed, in 1863 Abraham Lincoln helped found the U.S. National Academy of Sciences specifically to provide unbiased advice to the nation. To this day, the National Academies of Sciences, Engineering, and Medicine continue to do so. Their advice and that of the many conscientious and concerned scientists in our country should be heeded if we want to preserve our environment, improve the health of our population, and continue to reap the benefits that Science provides.
Finally, Mr. President, you have the important role of encouraging scientific excellence and recognizing scientific accomplishments, to spur others to make the discoveries so necessary for our future. For many years, the U.S. winners of the Nobel Prize have been invited to the White House and met with the President before going on to Sweden. Regrettably, these events have not occurred in the last four years. I encourage you to reinstate this very welcomed tradition. These meetings at the White House are the one time that the country, as represented by the President, thanks the Laureates for their achievements.
- - - - - - - - -
Joanne Chory, Ph.D.

- Professor and Director of the Plant Molecular and Cellular Biology Laboratory
- Howard H. and Maryam R. Newman Chair in Plant Biology
- Salk Institute for Biological Studies
- Investigator, Howard Hughes Medical Institute
- 2018 Breakthrough Prize in Life Sciences Laureate
Humanity is facing unprecedented challenges of a simultaneous and urgent nature rarely before seen in our history. A pandemic infection has brought the world's economy to its knees. Authoritarian assaults on democracy are increasing mistrust in governments and institutions. Global climate change is destabilizing lives and livelihoods. Now, more than ever, Americans and our allies are looking to the U.S. to lead the world through these monumental challenges.
Science and scholarship are the most powerful tools by which we may understand these challenges and how best to address them. The pursuit of truth, which is the bedrock of science and the linchpin of functioning democracy, must be our top priority for the next four years.
I urge you to commit to making evidence-based policy decisions, and to making science and foundational research your compass to help guide the world to a healthier, more stable future. It is not hyperbole to say humanity is at a crossroads, and that we face existential threats in the form of climate change and distrust of science.
Jonas Salk, who developed the first polio vaccine in response to the polio pandemics of the early 20th century before going on to found the Salk Institute for Biological Studies, once said, "Our greatest responsibility is to be good ancestors."
We owe future generations a healthy, habitable world.
- - - - - - - - -
Nina Fedoroff, Ph.D.

- Emeritus Evan Pugh Professor, Pennsylvania State University
- Senior Science Advisor, OFW Law
- 2006 National Medal of Science Laureate
I wish to draw your attention to a thorny issue whose impact on America will steadily grow in coming years as climate warming becomes ever more destructive to our food supply. I speak of the growing gap between what science can do to help agriculture and what's actually being done for farmers.
Spectacular advances in genetic knowledge and methods over the past half century have made it possible to adapt agriculture to a warming climate even while increasing agriculture's productivity and sustainability and reducing its environmental footprint.
But over the same half-century, public opinion has been systematically turned against the use of such modern methods of genetic modification (GM) by the organic food industry and public interest groups who have successfully vilified GM and created fear to increase their market share and raise money. A majority of consumers is now convinced that GM foods are bad or dangerous.
But the science says that GM foods are entirely safe for consumption by both people and animals. GM crops have now been grown commercially for a quarter of a century, boosting farmer incomes around the world, even while reducing pesticide use and greenhouse gas emissions. Unfortunately, current regulatory policy has all but precluded the rapid development of GM animals.
It is essential that the upcoming administration listen to the science and direct efforts toward relaxing excess regulatory constraints on GM. But more than that, it is essential that the government boldly promote GM approaches in agriculture to overcome the widespread disinformation promulgated by anti-GM groups. Public acceptance of GM foods is critical to their success in the marketplace.
Government investment can encourage private and public sector scientists to develop badly needed agricultural organisms biologically protected from the pathogens, pests, and stresses of the warming climate. But unequivocal government support of GM foods will be crucial to unleashing the scale of investment needed for farmers to stay ahead of the warming climate's growing downward pressure on their ability to feed the nation.
- - - - - - - - -
Andrew Z. Fire, Ph.D.

- Professor of Pathology and Genetics
- Stanford University School of Medicine
- 2006 Nobel Laureate for Physiology or Medicine
The next President of the United States can make the world a better place
But not alone. He or she will need to
Communicate with Americans
To know what is working in America
To know what needs to be fixed
To convey what people can do for their communities, their country, and their world
Communicate with scientists and experts
To understand what we have learned and what we can do
To understand the uncertainties in all science and technology
To understand what resources are needed to find and implement solutions
Engage beyond our borders
Because we share a fragile planet
The U.S. scientific community can make the world a better place
But not alone. We will need to
Listen to communities across the US to know where knowledge and solutions are needed.
Carefully and clearly convey facts and consequences in areas where we know.
Debate and unashamedly convey uncertainties and areas where we don't know.
Continue to engage with other scientists here and elsewhere to develop new approaches and understanding
Train a new generation of scientists to address current and future challenges
The American People can make the world a better place
But not alone. We will need to
Convey to leaders and scientists what is working and what needs to be fixed.
Educate ourselves in a broad range of science to make rational decisions
Participate in dialog toward designing solutions that improve life for everyone
Work together and listen with each other and with the world.
- - - - - - - - -
Joanna S. Fowler, Ph.D.

- Senior Scientist Emeritus
- Brookhaven National Laboratory
- 2008 National Medal of Science Laureate
Throughout our history, the United States has inspired and attracted students and scientists from around the world. They are typically motivated by the freedom to do creative work in our universities and research institutions unfettered by political interference. Immigrant scientists now make up 25% of our science and technology workforce and have contributed enormously to our economic growth and to the health and well-being of all Americans. They have also enhanced our prestige internationally, with immigrants to the United States winning 35% of the Nobel Prizes awarded to Americans in physics, chemistry, and medicine since 1901 and pointing to America's vision in embracing talent from around the world.
Unfortunately, recent anti-immigrant rhetoric and policies such as the travel ban and a recently issued proclamation that temporarily restricts many types of legal immigration (including students and scientists) have led many international students and scientists to reconsider building their careers in the United States.
It is urgent that our next President reassures the international community and our international students and scientists that (1) the United States will be an unwavering voice for bringing the power of science to the solution of global problems including the COVID-19 pandemic and climate change; (2) our policies and actions will be informed by science; and (3) international students and scientists who choose to come to the United States (as well as those already in our country) will be welcome and protected from political interference irrespective of their race or their country of origin.
- - - - - - - - -
Jeffrey Friedman, M.D., Ph.D.
- Marilyn M. Simpson Professor
- Rockefeller University
- 2020 Breakthrough Prize in Life Sciences Laureate
The COVID-19 pandemic has reaffirmed the critical role that science plays in peoples' lives. Stunning advances over the last 75 years made it possible to identify the infectious agent, develop robust new diagnostics, implement increasingly effective treatments (with more to come), and develop and test new vaccines all with startling rapidity. Compare this to the response to the Spanish Flu epidemic a century ago when it took years before the viral etiology was even confirmed. This remarkable progress provides a powerful reminder of why generous funding of science is crucial.
It is important to remember, however, that this stunning progress was made possible not just by scientists applying an ever-expanding body of knowledge to the current crisis but also by the innumerable scientists who laid the foundation that underpins that knowledge. This includes the scientists who, by following their own curiosity, showed that genes were made of DNA, defined how DNA after being copied into RNA provides the blueprint for making proteins in cells, and discovered that the genes in some viruses such as COVID are made of RNA rather than DNA. Still other scientists developed methods for isolating and studying genes and their functions in the laboratory.
In many cases, these enabling technologies depended on advances that had no obvious applications at the time, such as the discovery of restriction enzymes, proteins which cut DNA in specific places. This research was motivated not by practical considerations but by the curiosity of Nobel Prize winners Dan Nathans and Ham Smith who wanted to understand how bacteria protect themselves from the viruses (known as bacteriophage) that infect them. It was this advance, and many others like it, that helped to usher in the era of modern science that empowered the remarkable response to the current pandemic. So as we make the case to increase the funding of science, we need to ensure that the investments include not only the application of our current knowledge to our immediate needs, but also include investments in the curiosity-driven research that makes those applications possible.
- - - - - - - - -
Jerome I. Friedman, Ph.D.
- Institute Professor and Professor of Physics, Emeritus
- Massachusetts Institute of Technology
- 1990 Nobel Laureate in Physics
Investment in science and technology is an absolute necessity to develop the innovations that are needed to mitigate and reverse damage to the environment, protect our health, ensure future improvements in our standard of living, and stimulate economic growth. Applied research and invention play extremely important roles in innovation, but it should be emphasized that basic research has in general produced the major conceptual breakthroughs that have resulted in radically new technologies. For example, at a time in the past, electricity and magnetism were just laboratory curiosities. Now they are integral to the technologies of modern society. The study of the structure of the atom has led to the digital world in which we now live, and understanding the structure of DNA has revolutionized medicine. Such breakthroughs are needed to address and reduce the serious problems that afflict our world. To achieve our goals, we need to expand our base of fundamental knowledge to produce the new technologies that we desperately need. This will require a substantial increase in investment by the Federal Government in all types of research, and, because industry does not support basic research as it did in the past, the funding of basic research is especially dependent on the Federal Government. Funding for research is not a cost; it is an investment that will pay back rich dividends in the future, as it has done in the past.
- - - - - - - - -
Elaine Fuchs, Ph.D.

- Professor of Mammalian Cell Biology and Development
- Rockefeller University
- Investigator, Howard Hughes Medical Institute
- 2008 National Medal of Science Laureate
The COVID-19 pandemic exemplifies why our nation needs an effective, rapid response team of scientific experts to help contain the spread of infectious pathogens. In times of a pandemic, America must also mobilize government funds to enable another cadre of scientists to identify ways to disarm the microbes. However, such efforts will only succeed when the existing basic science foundation is strong. Our nation has long been the world's leader in biomedical research, and our accrued knowledge of viruses, their ability to infect epithelial cells, and the inflammatory responses that they elicit, gave our scientists the jumpstart necessary to rapidly develop vaccines and neutralizing antibodies against the SARS-CoV2 virus. With the ever-increasing barrage of unexpected health challenges that our changing climate imposes upon us, America must continue to strengthen and broaden our basic science foundation and to provide the training and support to prepare the next generations of scientists to participate in this endeavor.
As a basic scientist working at the interface between science and medicine, I've witnessed numerous examples in my career that illustrate how important basic science is for advancing new and improved treatments for human conditions. For example, mutations in a nuclear modification first described in algae causes a lethal brain cancer in children. Additionally, current cancer treatments often make patients sick because they harm both healthy and cancerous tissue, and the cancers often relapse after treatment. Determining which cancer cells are responsible for relapse and how they differ from the healthy stem cells that fuel normal tissue growth and repair, could lead to blueprints for designing therapeutics that effectively kill these resilient cancerous cells without harming the normal tissue.
Our government's long-standing support for basic science makes it easier than ever before to solve the scientific puzzles needed to disarm threats to our health and fitness. However, our bodies are continually exposed to new stresses, new microbes, new pollution. By keeping a high pace of basic science and discovery, and inspiring and training the best and brightest young minds from diverse backgrounds, we will stand the best chance of being prepared for whatever nature has in store for us in the future.
- - - - - - - - -
H. Robert Horvitz, Ph.D.
- David H. Koch Professor in Biology
- Massachusetts Institute of Technology
- Investigator, Howard Hughes Medical Institute
- 2002 Nobel Laureate in Physiology or Medicine
While resoundingly validating the investment in biomedical research that has been made over the past decades, the response of our nation to the COVID-19 pandemic has also cast a harsh light on us, including on aspects of our national scientific and biomedical enterprise, revealing gaps in understanding as well as in the efficient application and deployment of available knowledge and technology. As we enter a new Presidential term, American science needs to draw on its COVID-19 experiences, both the innovative and the painful, to face a changing world. Scientists have much to learn in the coming months from COVID-19 about emerging health challenges, about safeguarding our nation's physical health, and about sustaining American leadership in biomedical research. By leading our country over the next four years, you will have the opportunity to impact the health and safety of generations of Americans.
Past federal investment in biomedical research has been extraordinarily productive. Largely through research conducted or supported by the National Institutes of Health (NIH), the United States has led the way in pioneering crucial diagnostic procedures, novel treatments, life-changing cures, and innovative prevention strategies for a broad variety of disorders, including cancer and heart disease. This core of evidence-based science powered our response to the pandemic as NIH-supported scientists unraveled the basic biology of the SARS-CoV2 virus, drove unprecedentedly rapid diagnostic and vaccine development, and sharpened treatment protocols. Maintaining—and bolstering—that core is critical to our national health, economy, and security.
The NIH must now reaffirm its commitment to fundamental and bold biomedical research. That is why, along with 13 of my colleagues from across the nation, I am preparing a report that seeks to advise the next Administration about how best to capitalize on the enormous promise of 21st-century biology. Our NIH Vision and Pathways report will provide a perspective on and vision for biomedical research and health, as well as describe specific proposed changes that will focus and strengthen NIH to achieve that vision. Our suggestions encompass four areas concerning NIH structure and operations:
- Research: Driving Innovation and Discovery
- Training: Preparing the Next Generation
- Administration and Operations: Maximizing Opportunity
- Appointment of the NIH Director
Your administration can seize this opportunity to shape the NIH, a crown jewel of the federal government, in ways that will make it more impactful and efficient in improving the health and well-being of Americans and will ensure the leadership position of our country in the field of biomedicine for decades to come.
- - - - - - - - -
David Julius, Ph.D.

- Professor and Chair of Physiology
- University of California, San Francisco
- 2020 Breakthrough Prize in Life Sciences Laureate
A couple of Thanksgiving dinners ago, I got into a discussion with a relative who disparaged climate change as a hoax. I pointed out that he was the same person who prided our country for its legendary technical and scientific accomplishments, such as building the Panama Canal, landing on the moon, or conquering polio. Honestly, I was amazed at this contradiction: how can someone believe so fervently in the idea of "American Exceptionalism" yet now devalue and discount the advice of our scientific and engineering community? Can we really have it both ways?
Perhaps more than anything else, the next President of the United States must take on the goal of repairing and reestablishing respect for education, knowledge, professional expertise, and fact-based decision making. Otherwise, the foundation of our nation's legendary scientific and engineering excellence shall crumble. Scientists and engineers hail from all corners of our country and world—urban and rural, wealthy and poor, etc. What unites us is a passion for curiosity, discovery, creativity, and problem solving. Our next leader must challenge the canard that scientists constitute a class of intellectual and cultural elites separate from the rest of society.
With regard to biomedical research, I remain a believer in the power of basic, curiosity-driven research. Time and again, we find that transformational discoveries in science and medicine come from unexpected or unanticipated avenues of inquiry (think CRISPR gene-editing technology, discovery of innate immune pathways in flies, or snake venoms as the inspiration for anti-hypertensive drugs). Certainly there are moments—such as the current COVID-19 pandemic—to mobilize goal-directed efforts, but we must not forsake bedrock basic, curiosity-driven research programs, which will continue to yield discoveries that move biomedical research and technology forward so we can tackle known diseases or the next unforeseen global health challenge.
- - - - - - - - -
William G. Kaelin, Jr., M.D.

- Sidney Farber Professor of Medicine
- Dana-Farber Cancer Institute and Brigham and Women's Hospital
- Harvard Medical School
- Investigator, Howard Hughes Medical Institute
- 2019 Nobel Laureate in Physiology or Medicine
Winning the Nobel Prize last year has caused me to reflect on some of the ways government policies influenced my career. I was born in 1957, about six weeks after the Sputnik launch. Science and engineering were celebrated in the United States during my childhood, partly because of the ensuing space race and the Cold War. Bipartisan support for science education and scientific research was like mom and apple pie for most of my early years. I had the opportunity in 1974 to attend a National Science Foundation Student Science Training Program in Computers and Mathematics that absolutely transformed me as a student because it was the first time I was surrounded by students who were almost uniformly smarter than I was and the first time I encountered a curriculum that I found truly challenging and interesting. During my clinical training to become a doctor, I routinely encountered brilliant physician-scientists, many of whom had trained at the National Institutes of Health (NIH) during the Vietnam War era (the so-called "Yellow Berets"). When I pivoted from clinical medicine to laboratory research in the 1980s, my development was supported by NIH training and research grants. In 1994, the NIH budget was doubled with bipartisan support, just as my funding was growing perilous. It enabled me to pursue the work that led to my Nobel Prize.
Sadly, federal support for science has been flat for many years now. What is worse, some politicians, to accomplish their political agendas, use language that disparages science and scientists and act as though knowledge and truth are subjective. Adding further insult, the economic disruptions from COVID-19 are likely to decrease the hiring of newly minted scientists by academia. We run the risk of losing the next generation of researchers if we don't immediately take steps to convince young people that seeking truth and knowledge is a noble endeavor and that their careers will be valued and supported. I would pay particular attention to the support of basic, fundamental research. A formula that served us well dating back to the middle of the last century was to have the federal government support basic science and to have the private sector decide when the knowledge it generated was ripe for application. Basic science is the most vulnerable part of the entire research enterprise, partly because its timelines and deliverables are often unknowable (and hence shunned by investors), and yet it is basic science that over and over leads to the truly transformative discoveries that change the way we think about the world and improve our lives. It is also the formula that explains why Americans have won a disproportionate number of Nobel Prizes over the last century. This formula has not escaped the notice of some of our competitors. It would be tragic if we ourselves forgot it.
- - - - - - - - -
Judith P. Klinman, Ph.D.

- Professor of the Graduate School and Chancellor's Professor of Chemistry
- University of California, Berkeley
- 2012 National Medal of Science Laureate
During the 20th and early 21st centuries, American science experienced a "Golden Age." While this may have been taken for granted by many of us in the scientific community, it is impossible to ignore its decline during the last four years. The neglect and disengagement of government support for key agencies, and science in general, have been devastating on many levels, the most immediate being the excessive and unnecessary number of deaths from COVID-19. The current pandemic is unlikely to be a standalone event and is connected to the ongoing loss of natural habitats within the larger "Climate Change" crisis.
The divestment of government from knowledge-based engagement in global warming has become both immoral and irresponsible, and the time for remediation is rapidly running out. I believe it is imperative that the next administration work quickly on multiple fronts that include a complete and rapid refocus on sustainable energy, a continuing investment in research toward carbon capture, and the pursuit of best practices that will support a new infrastructure that enables the necessary behavioral changes of all citizens. Unless we work quickly and effectively, the younger generation that includes our children (both biological and academic) are, I fear, inheriting an uninhabitable Planet Earth.
- - - - - - - - -
J. Michael Kosterlitz, Ph.D.

- Harrison E. Farnsworth Professor of Physics
- Brown University
- 2016 Nobel Laureate in Physics
There are two parts to the development of a device like the cell phone. First, you need the theoretical scientists who pursue various avenues of knowledge out of curiosity. Then, you need the practical scientists who today are called engineers or, in medicine, doctors. They take theoretical knowledge developed by theorists, play with it, and, with a lot of luck, develop some useful device based on the existing theoretical understanding. It is important to realize that both parts are needed. The basic theoretical understanding comes first followed by the development of some practical device which is not possible without the underlying theory. Both types of science are necessary for a final outcome. To an average person, who neither knows nor cares about science, only the engineering part seems important because the connection is more immediate. However, for the successful development of some useful device, both are usually equally important. Without the basic knowledge developed by the scientist doing apparently useless curiosity-driven research, the basic understanding for the practical development would not be there, so the device would not be built. Both the theoretical and the practical skills are needed and both should be adequately funded. One cannot exist without the other, and results from one feed into the other.
For the next four years of your presidency, one of the most important considerations is the health of the population. As we have all seen during the coronavirus pandemic, the whole country suffers when the population does not have adequate access to effective health care. This should be central to your presidency because the economy of the country depends critically on a healthy population. The key to a vibrant economy is adequate government funding of the whole scientific effort in as many branches as possible. Of course, there will be some inevitable wastage but, to keep America competitive, funding by government and supplemented by private agencies of all the real sciences is vital. I do not have the conceit to make specific suggestions about which branch of science or engineering is more important than another. They all deserve some funding until such time that they are proved to be useless or wrong like the old discredited phlogiston theory of burning.
- - - - - - - - -
Adrian R. Krainer, Ph.D.

- St. Giles Foundation Professor
- Cold Spring Harbor Laboratory
- 2019 Breakthrough Prize in Life Sciences Laureate
Congratulations on your election. The next four years will pose major challenges, but we have the ability to address them effectively. I arrived in this country as a foreign student four decades ago, to begin my college education. I chose to study in the U.S. because I knew it was the top place in the world for biomedical research, and I was fortunate to have this opportunity. After graduate school, I accepted a job offer in academic research, I became a resident and then a citizen, and I never looked back. Together with my trainees—who came from the U.S. and 20 other countries—and our collaborators, we succeeded in developing an effective treatment for a devastating genetic disease, helping thousands of patients around the world live longer and more productive lives, and creating many jobs in the process. I know from this experience that government funding of basic research, e.g., through the NIH and NSF, plays an incredibly important role. This public investment ultimately improves the lives for all humanity, and along the way it results in job creation and attracts top talent from the U.S. and abroad. Other countries, notably China, have emulated us by making massive investments in education, science, technology, and infrastructure, with increasingly impressive results. To remain at the forefront, we must increase or at least sustain the pace of public investment in these key areas. Our institutions of higher learning continue to be a magnet for top talent from around the world. Some of these visitors eventually choose to stay, and we should welcome them; others will return home but maintain connections with, and good will toward, America. Science is a global endeavor, and challenges such as human diseases, pandemics, and climate change know no international boundaries. The U.S. must continue to lead the world in the search for effective solutions to these vexing problems.
- - - - - - - - -
John C. Mather, Ph.D.

- 2006 Nobel Laureate in Physics
We need to upgrade the EPA into the National Environmental Defense Agency (NEDA) with a charter to protect all Americans as a matter of national security, equal in importance to the Department of Defense and the Department of Homeland Security. Failure to address climate change would be a worldwide and permanent catastrophe, so the NEDA would take all necessary actions including measurement, analysis, fundamental research, technology development and commercialization, disaster planning, infrastructure support for mitigation, and international leadership. Congress should support this work because it means jobs for millions of Americans, and taxpayers should support it because it preserves their wealth. The health and prosperity of Americans for the next four years, and on for at least the next thousand, depend now and always on noticing what's happening and responding accordingly. But we've been caught unprepared for multiple disasters, and more are coming. Some could be mitigated with planning and organization at all levels from international and federal to personal, and some need inventions and discoveries we don't yet have. Though the time scale is uncertain, the sea is rising every year, with no end in sight. When the sea rises six feet, over ten million Americans will lose their homes and land. When the tropics become unbearably hot, more millions will migrate to America. If a foreign power were taking our land, we would act. If a foreign power were setting the American West ablaze, we would act. If our farms were dying, we would act. Shall we not act? We need responsibility, authority, and a plan. It might sound impossible, but so were electricity, moon rockets, and the internet not long ago. We can do this, and you as President can make it happen.
- - - - - - - - -

Dry, arid and remote farming regions are vulnerable to water shortages, but scientists are working on a promising new solution.
As scientists have searched for solutions, an alternative water supply has been hiding in plain sight: Water vapor in the atmosphere. It is abundant, available, and endlessly renewable, just waiting for the moment that technological innovation and necessity converged to make it fit for use. Now, new super-moisture-absorbent gels developed by Yu and a team of researchers can pull that moisture from the air and bring it into soil, potentially expanding the map of farmable land around the globe to dry and remote regions that suffer from water shortages.
"This opens up opportunities to turn those previously poor-quality or inhospitable lands to become useable and without need of centralized water and power supplies," Yu said.
A renewable source of freshwater
The hydrogels are a gelatin-like substance made from synthetic materials. The gels activate in cooler, humid overnight periods and draw water from the air. During a four-week experiment, Yu's team observed that soil with these gels provided enough water to support seed germination and plant growth without an additional liquid water supply. And the soil was able to maintain the moist environment for more than a month, according to Yu.
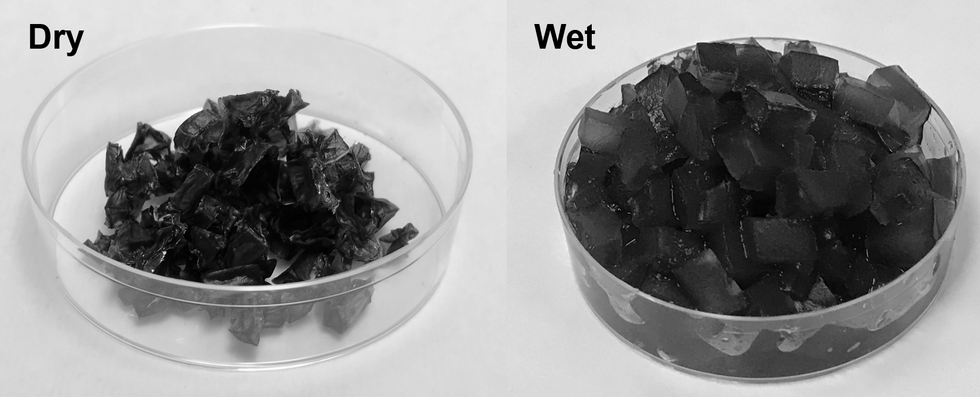
The super absorbent gels developed at the University of Texas at Austin.
Xingyi Zhou, UT Austin
"It is promising to liberate underdeveloped and drought areas from the long-distance water and power supplies for agricultural production," Yu said.
Crops also rely on fertilizer to maintain soil fertility and increase the production yield, but it is easily lost through leaching. Runoff increases agricultural costs and contributes to environmental pollution. The interaction between the gels and agrochemicals offer slow and controlled fertilizer release to maintain the balance between the root of the plant and the soil.
The possibilities are endless
Harvesting atmospheric water is exciting on multiple fronts. The super-moisture-absorbent gel can also be used for passively cooling solar panels. Solar radiation is the magic behind the process. Overnight, as temperatures cool, the gels absorb water hanging in the atmosphere. The moisture is stored inside the gels until the thermometer rises. Heat from the sun serves as the faucet that turns the gels on so they can release the stored water and cool down the panels. Effective cooling of the solar panels is important for sustainable long-term power generation.
In addition to agricultural uses and cooling for energy devices, atmospheric water harvesting technologies could even reach people's homes.
"They could be developed to enable easy access to drinking water through individual systems for household usage," Yu said.
Next steps
Yu and the team are now focused on affordability and developing practical applications for use. The goal is to optimize the gel materials to achieve higher levels of water uptake from the atmosphere.
"We are exploring different kinds of polymers and solar absorbers while exploring low-cost raw materials for production," Yu said.
The ability to transform atmospheric water vapor into a cheap and plentiful water source would be a game-changer. One day in the not-too-distant future, if climate change intensifies and droughts worsen, this innovation may become vital to our very survival.