
Probiotic bacteria can be engineered to fight antibiotic-resistant superbugs by releasing chemicals that kill them.
In 1945, almost two decades after Alexander Fleming discovered penicillin, he warned that as antibiotics use grows, they may lose their efficiency. He was prescient—the first case of penicillin resistance was reported two years later. Back then, not many people paid attention to Fleming’s warning. After all, the “golden era” of the antibiotics age had just began. By the 1950s, three new antibiotics derived from soil bacteria — streptomycin, chloramphenicol, and tetracycline — could cure infectious diseases like tuberculosis, cholera, meningitis and typhoid fever, among others.
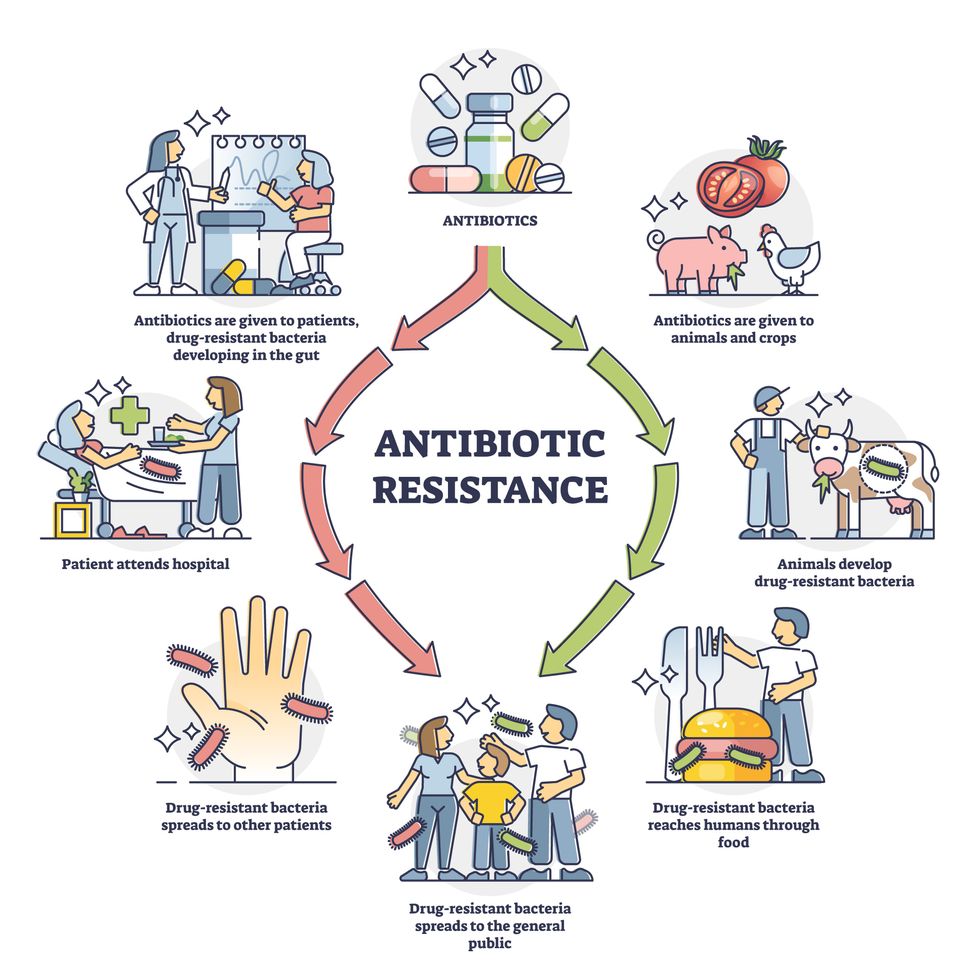
Today, these antibiotics and many of their successors developed through the 1980s are gradually losing their effectiveness. The extensive overuse and misuse of antibiotics led to the rise of drug resistance. The livestock sector buys around 80 percent of all antibiotics sold in the U.S. every year. Farmers feed cows and chickens low doses of antibiotics to prevent infections and fatten up the animals, which eventually causes resistant bacterial strains to evolve. If manure from cattle is used on fields, the soil and vegetables can get contaminated with antibiotic-resistant bacteria. Another major factor is doctors overprescribing antibiotics to humans, particularly in low-income countries. Between 2000 to 2018, the global rates of human antibiotic consumption shot up by 46 percent.
In recent years, researchers have been exploring a promising avenue: the use of synthetic biology to engineer new bacteria that may work better than antibiotics. The need continues to grow, as a Lancet study linked antibiotic resistance to over 1.27 million deaths worldwide in 2019, surpassing HIV/AIDS and malaria. The western sub-Saharan Africa region had the highest death rate (27.3 people per 100,000).
Researchers warn that if nothing changes, by 2050, antibiotic resistance could kill 10 million people annually.
To make it worse, our remedy pipelines are drying up. Out of the 18 biggest pharmaceutical companies, 15 abandoned antibiotic development by 2013. According to the AMR Action Fund, venture capital has remained indifferent towards biotech start-ups developing new antibiotics. In 2019, at least two antibiotic start-ups filed for bankruptcy. As of December 2020, there were 43 new antibiotics in clinical development. But because they are based on previously known molecules, scientists say they are inadequate for treating multidrug-resistant bacteria. Researchers warn that if nothing changes, by 2050, antibiotic resistance could kill 10 million people annually.
The rise of synthetic biology
To circumvent this dire future, scientists have been working on alternative solutions using synthetic biology tools, meaning genetically modifying good bacteria to fight the bad ones.
From the time life evolved on earth around 3.8 billion years ago, bacteria have engaged in biological warfare. They constantly strategize new methods to combat each other by synthesizing toxic proteins that kill competition.
For example, Escherichia coli produces bacteriocins or toxins to kill other strains of E.coli that attempt to colonize the same habitat. Microbes like E.coli (which are not all pathogenic) are also naturally present in the human microbiome. The human microbiome harbors up to 100 trillion symbiotic microbial cells. The majority of them are beneficial organisms residing in the gut at different compositions.
The chemicals that these “good bacteria” produce do not pose any health risks to us, but can be toxic to other bacteria, particularly to human pathogens. For the last three decades, scientists have been manipulating bacteria’s biological warfare tactics to our collective advantage.
In the late 1990s, researchers drew inspiration from electrical and computing engineering principles that involve constructing digital circuits to control devices. In certain ways, every cell in living organisms works like a tiny computer. The cell receives messages in the form of biochemical molecules that cling on to its surface. Those messages get processed within the cells through a series of complex molecular interactions.
Synthetic biologists can harness these living cells’ information processing skills and use them to construct genetic circuits that perform specific instructions—for example, secrete a toxin that kills pathogenic bacteria. “Any synthetic genetic circuit is merely a piece of information that hangs around in the bacteria’s cytoplasm,” explains José Rubén Morones-Ramírez, a professor at the Autonomous University of Nuevo León, Mexico. Then the ribosome, which synthesizes proteins in the cell, processes that new information, making the compounds scientists want bacteria to make. “The genetic circuit remains separated from the living cell’s DNA,” Morones-Ramírez explains. When the engineered bacteria replicates, the genetic circuit doesn’t become part of its genome.
Highly intelligent by bacterial standards, some multidrug resistant V. cholerae strains can also “collaborate” with other intestinal bacterial species to gain advantage and take hold of the gut.
In 2000, Boston-based researchers constructed an E.coli with a genetic switch that toggled between turning genes on and off two. Later, they built some safety checks into their bacteria. “To prevent unintentional or deleterious consequences, in 2009, we built a safety switch in the engineered bacteria’s genetic circuit that gets triggered after it gets exposed to a pathogen," says James Collins, a professor of biological engineering at MIT and faculty member at Harvard University’s Wyss Institute. “After getting rid of the pathogen, the engineered bacteria is designed to switch off and leave the patient's body.”
Overuse and misuse of antibiotics causes resistant strains to evolve
Adobe Stock
Seek and destroy
As the field of synthetic biology developed, scientists began using engineered bacteria to tackle superbugs. They first focused on Vibrio cholerae, which in the 19th and 20th century caused cholera pandemics in India, China, the Middle East, Europe, and Americas. Like many other bacteria, V. cholerae communicate with each other via quorum sensing, a process in which the microorganisms release different signaling molecules, to convey messages to its brethren. Highly intelligent by bacterial standards, some multidrug resistant V. cholerae strains can also “collaborate” with other intestinal bacterial species to gain advantage and take hold of the gut. When untreated, cholera has a mortality rate of 25 to 50 percent and outbreaks frequently occur in developing countries, especially during floods and droughts.
Sometimes, however, V. cholerae makes mistakes. In 2008, researchers at Cornell University observed that when quorum sensing V. cholerae accidentally released high concentrations of a signaling molecule called CAI-1, it had a counterproductive effect—the pathogen couldn’t colonize the gut.
So the group, led by John March, professor of biological and environmental engineering, developed a novel strategy to combat V. cholerae. They genetically engineered E.coli to eavesdrop on V. cholerae communication networks and equipped it with the ability to release the CAI-1 molecules. That interfered with V. cholerae progress. Two years later, the Cornell team showed that V. cholerae-infected mice treated with engineered E.coli had a 92 percent survival rate.
These findings inspired researchers to sic the good bacteria present in foods like yogurt and kimchi onto the drug-resistant ones.
Three years later in 2011, Singapore-based scientists engineered E.coli to detect and destroy Pseudomonas aeruginosa, an often drug-resistant pathogen that causes pneumonia, urinary tract infections, and sepsis. Once the genetically engineered E.coli found its target through its quorum sensing molecules, it then released a peptide, that could eradicate 99 percent of P. aeruginosa cells in a test-tube experiment. The team outlined their work in a Molecular Systems Biology study.
“At the time, we knew that we were entering new, uncharted territory,” says lead author Matthew Chang, an associate professor and synthetic biologist at the National University of Singapore and lead author of the study. “To date, we are still in the process of trying to understand how long these microbes stay in our bodies and how they might continue to evolve.”
More teams followed the same path. In a 2013 study, MIT researchers also genetically engineered E.coli to detect P. aeruginosa via the pathogen’s quorum-sensing molecules. It then destroyed the pathogen by secreting a lab-made toxin.
Probiotics that fight
A year later in 2014, a Nature study found that the abundance of Ruminococcus obeum, a probiotic bacteria naturally occurring in the human microbiome, interrupts and reduces V.cholerae’s colonization— by detecting the pathogen’s quorum sensing molecules. The natural accumulation of R. obeum in Bangladeshi adults helped them recover from cholera despite living in an area with frequent outbreaks.
The findings from 2008 to 2014 inspired Collins and his team to delve into how good bacteria present in foods like yogurt and kimchi can attack drug-resistant bacteria. In 2018, Collins and his team developed the engineered probiotic strategy. They tweaked a bacteria commonly found in yogurt called Lactococcus lactis to treat cholera.
Engineered bacteria can be trained to target pathogens when they are at their most vulnerable metabolic stage in the human gut. --José Rubén Morones-Ramírez.
More scientists followed with more experiments. So far, researchers have engineered various probiotic organisms to fight pathogenic bacteria like Staphylococcus aureus (leading cause of skin, tissue, bone, joint and blood infections) and Clostridium perfringens (which causes watery diarrhea) in test-tube and animal experiments. In 2020, Russian scientists engineered a probiotic called Pichia pastoris to produce an enzyme called lysostaphin that eradicated S. aureus in vitro. Another 2020 study from China used an engineered probiotic bacteria Lactobacilli casei as a vaccine to prevent C. perfringens infection in rabbits.
In a study last year, Ramírez’s group at the Autonomous University of Nuevo León, engineered E. coli to detect quorum-sensing molecules from Methicillin-resistant Staphylococcus aureus or MRSA, a notorious superbug. The E. coli then releases a bacteriocin that kills MRSA. “An antibiotic is just a molecule that is not intelligent,” says Ramírez. “On the other hand, engineered bacteria can be trained to target pathogens when they are at their most vulnerable metabolic stage in the human gut.”
Collins and Timothy Lu, an associate professor of biological engineering at MIT, found that engineered E. coli can help treat other conditions—such as phenylketonuria, a rare metabolic disorder, that causes the build-up of an amino acid phenylalanine. Their start-up Synlogic aims to commercialize the technology, and has completed a phase 2 clinical trial.
Circumventing the challenges
The bacteria-engineering technique is not without pitfalls. One major challenge is that beneficial gut bacteria produce their own quorum-sensing molecules that can be similar to those that pathogens secrete. If an engineered bacteria’s biosensor is not specific enough, it will be ineffective.
Another concern is whether engineered bacteria might mutate after entering the gut. “As with any technology, there are risks where bad actors could have the capability to engineer a microbe to act quite nastily,” says Collins of MIT. But Collins and Ramírez both insist that the chances of the engineered bacteria mutating on its own are virtually non-existent. “It is extremely unlikely for the engineered bacteria to mutate,” Ramírez says. “Coaxing a living cell to do anything on command is immensely challenging. Usually, the greater risk is that the engineered bacteria entirely lose its functionality.”
However, the biggest challenge is bringing the curative bacteria to consumers. Pharmaceutical companies aren’t interested in antibiotics or their alternatives because it’s less profitable than developing new medicines for non-infectious diseases. Unlike the more chronic conditions like diabetes or cancer that require long-term medications, infectious diseases are usually treated much quicker. Running clinical trials are expensive and antibiotic-alternatives aren’t lucrative enough.
“Unfortunately, new medications for antibiotic resistant infections have been pushed to the bottom of the field,” says Lu of MIT. “It's not because the technology does not work. This is more of a market issue. Because clinical trials cost hundreds of millions of dollars, the only solution is that governments will need to fund them.” Lu stresses that societies must lobby to change how the modern healthcare industry works. “The whole world needs better treatments for antibiotic resistance.”


In the U.S., hospitals generate an estimated 6,000 tons of waste per day. A few clinics are leading the way in transitioning to clean energy sources.
She decided to research alternatives for plastic in the medical sector and learned that cups could be reused and easily disinfected. All dentists routinely disinfect their tools anyway and, Stroetzel reasoned, it wouldn’t be too hard to extend that practice to cups.
It's a good example for how often plastic is used unnecessarily in medical practice, she says. The health care sector is the fifth biggest source of pollution and trash in industrialized countries. In the U.S., hospitals generate an estimated 6,000 tons of waste per day, including an average of 400 grams of plastic per patient per day, and this sector produces 8.5 percent of greenhouse gas emissions nationwide.
“Sustainable alternatives exist,” Stroetzel says, “but you have to painstakingly look for them; they are often not offered by the big manufacturers, and all of this takes way too much time [that] medical staff simply does not have during their hectic days.”
When Stroetzel spoke with medical staff in Germany, she found they were often frustrated by all of this waste, especially as they took care to avoid single-use plastic at home. Doctors in other countries share this frustration. In a recent poll, nine out of ten doctors in Germany said they’re aware of the urgency to find sustainable solutions in the health industry but don’t know how to achieve this goal.
After a year of researching more sustainable alternatives, Stroetzel founded a social enterprise startup called POP, short for Practice Without Plastic, together with IT expert Nicolai Niethe, to offer well-researched solutions. “Sustainable alternatives exist,” she says, “but you have to painstakingly look for them; they are often not offered by the big manufacturers, and all of this takes way too much time [that] medical staff simply does not have during their hectic days.”
In addition to reusable dentist cups, other good options for the heath care sector include washable N95 face masks and gloves made from nitrile, which waste less water and energy in their production. But Stroetzel admits that truly making a medical facility more sustainable is a complex task. “This includes negotiating with manufacturers who often package medical materials in double and triple layers of extra plastic.”
While initiatives such as Stroetzel’s provide much needed information, other experts reason that a wholesale rethinking of healthcare is needed. Voluntary action won’t be enough, and government should set the right example. Kari Nadeau, a Stanford physician who has spent 30 years researching the effects of environmental pollution on the immune system, and Kenneth Kizer, the former undersecretary for health in the U.S. Department of Veterans Affairs, wrote in JAMA last year that the medical industry and federal agencies that provide health care should be required to measure and make public their carbon footprints. “Government health systems do not disclose these data (and very rarely do private health care organizations), unlike more than 90% of the Standard & Poor’s top 500 companies and many nongovernment entities," they explained. "This could constitute a substantial step toward better equipping health professionals to confront climate change and other planetary health problems.”
Compared to the U.K., the U.S. healthcare industry lags behind in terms of measuring and managing its carbon footprint, and hospitals are the second highest energy user of any sector in the U.S.
Kizer and Nadeau look to the U.K. National Health Service (NHS), which created a Sustainable Development Unit in 2008 and began that year to conduct assessments of the NHS’s carbon footprint. The NHS also identified its biggest culprits: Of the 2019 footprint, with emissions totaling 25 megatons of carbon dioxide equivalent, 62 percent came from the supply chain, 24 percent from the direct delivery of care, 10 percent from staff commute and patient and visitor travel, and 4 percent from private health and care services commissioned by the NHS. From 1990 to 2019, the NHS has reduced its emission of carbon dioxide equivalents by 26 percent, mostly due to the switch to renewable energy for heat and power. Meanwhile, the NHS has encouraged health clinics in the U.K. to install wind generators or photovoltaics that convert light to electricity -- relatively quick ways to decarbonize buildings in the health sector.
Compared to the U.K., the U.S. healthcare industry lags behind in terms of measuring and managing its carbon footprint, and hospitals are the second highest energy user of any sector in the U.S. “We are already seeing patients with symptoms from climate change, such as worsened respiratory symptoms from increased wildfires and poor air quality in California,” write Thomas B. Newman, a pediatrist at the University of California, San Francisco, and UCSF clinical research coordinator Daisy Valdivieso. “Because of the enormous health threat posed by climate change, health professionals should mobilize support for climate mitigation and adaptation efforts.” They believe “the most direct place to start is to approach the low-lying fruit: reducing healthcare waste and overuse.”
In addition to resulting in waste, the plastic in hospitals ultimately harms patients, who may be even more vulnerable to the effects due to their health conditions. Microplastics have been detected in most humans, and on average, a human ingests five grams of microplastic per week. Newman and Valdivieso refer to the American Board of Internal Medicine's Choosing Wisely program as one of many initiatives that identify and publicize options for “safely doing less” as a strategy to reduce unnecessary healthcare practices, and in turn, reduce cost, resource use, and ultimately reduce medical harm.
A few U.S. clinics are pioneers in transitioning to clean energy sources. In Wisconsin, the nonprofit Gundersen Health network became the first hospital to cut its reliance on petroleum by switching to locally produced green energy in 2015, and it saved $1.2 million per year in the process. Kaiser Permanente eliminated its 800,000 ton carbon footprint through energy efficiency and purchasing carbon offsets, reaching a balance between carbon emissions and removing carbon from the atmosphere in 2020, the first U.S. health system to do so.
Cleveland Clinic has pledged to join Kaiser in becoming carbon neutral by 2027. Realizing that 80 percent of its 2008 carbon emissions came from electricity consumption, the Clinic started switching to renewable energy and installing solar panels, and it has invested in researching recyclable products and packaging. The Clinic’s sustainability report outlines several strategies for producing less waste, such as reusing cases for sterilizing instruments, cutting back on materials that can’t be recycled, and putting pressure on vendors to reduce product packaging.
The Charité Berlin, Europe’s biggest university hospital, has also announced its goal to become carbon neutral. Its sustainability managers have begun to identify the biggest carbon culprits in its operations. “We’ve already reduced CO2 emissions by 21 percent since 2016,” says Simon Batt-Nauerz, the director of infrastructure and sustainability.
The hospital still emits 100,000 tons of CO2 every year, as much as a city with 10,000 residents, but it’s making progress through ride share and bicycle programs for its staff of 20,000 employees, who can get their bikes repaired for free in one of the Charité-operated bike workshops. Another program targets doctors’ and nurses’ scrubs, which cause more than 200 tons of CO2 during manufacturing and cleaning. The staff is currently testing lighter, more sustainable scrubs made from recycled cellulose that is grown regionally and requires 80 percent less land use and 30 percent less water.

The Charité hospital in Berlin still emits 100,000 tons of CO2 every year, but it’s making progress through ride share and bicycle programs for its staff of 20,000 employees.
Wiebke Peitz | Specific to Charité
Anesthesiologist Susanne Koch spearheads sustainability efforts in anesthesiology at the Charité. She says that up to a third of hospital waste comes from surgery rooms. To reduce medical waste, she recommends what she calls the 5 Rs: Reduce, Reuse, Recycle, Rethink, Research. “In medicine, people don’t question the use of plastic because of safety concerns,” she says. “Nobody wants to be sued because something is reused. However, it is possible to reduce plastic and other materials safely.”
For instance, she says, typical surgery kits are single-use and contain more supplies than are actually needed, and the entire kit is routinely thrown out after the surgery. “Up to 20 percent of materials in a surgery room aren’t used but will be discarded,” Koch says. One solution could be smaller kits, she explains, and another would be to recycle the plastic. Another example is breathing tubes. “When they became scarce during the pandemic, studies showed that they can be used seven days instead of 24 hours without increased bacteria load when we change the filters regularly,” Koch says, and wonders, “What else can we reuse?”
In the Netherlands, TU Delft researchers Tim Horeman and Bart van Straten designed a method to melt down the blue polypropylene wrapping paper that keeps medical instruments sterile, so that the material can be turned it into new medical devices. Currently, more than a million kilos of the blue paper are used in Dutch hospitals every year. A growing number of Dutch hospitals are adopting this approach.
Another common practice that’s ripe for improvement is the use of a certain plastic, called PVC, in hospital equipment such as blood bags, tubes and masks. Because of its toxic components, PVC is almost never recycled in the U.S., but University of Michigan researchers Danielle Fagnani and Anne McNeil have discovered a chemical process that can break it down into material that could be incorporated back into production. This could be a step toward a circular economy “that accounts for resource inputs and emissions throughout a product’s life cycle, including extraction of raw materials, manufacturing, transport, use and reuse, and disposal,” as medical experts have proposed. “It’s a failure of humanity to have created these amazing materials which have improved our lives in many ways, but at the same time to be so shortsighted that we didn’t think about what to do with the waste,” McNeil said in a press release.
Susanne Koch puts it more succinctly: “What’s the point if we save patients while killing the planet?”