

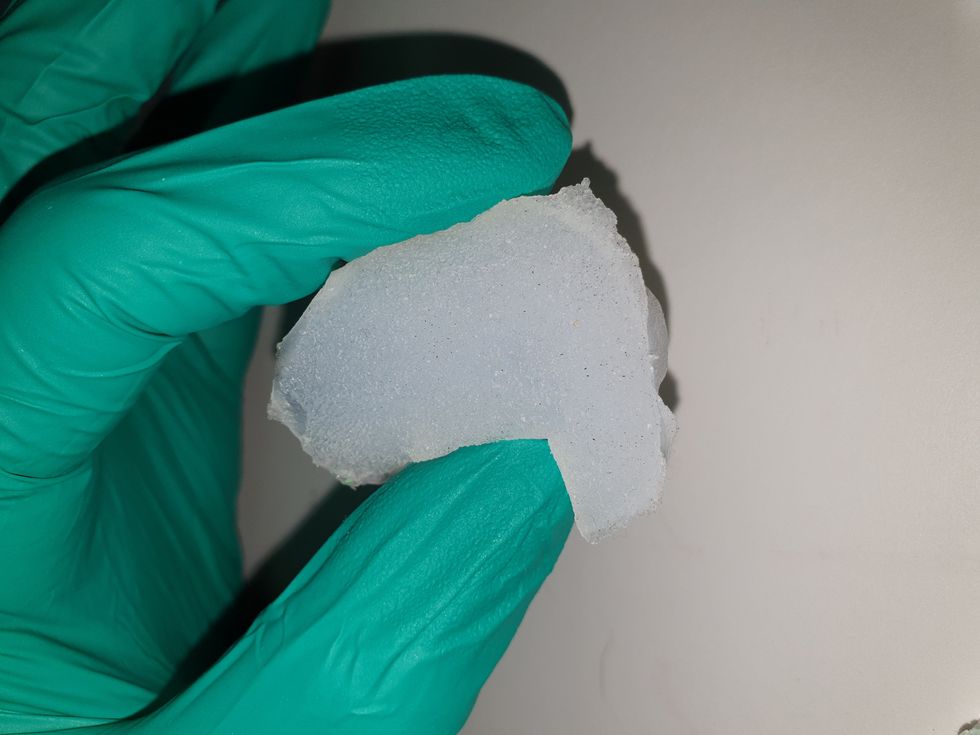
Researchers are looking to engineer chocolate with less oil, which could reduce some of its detriments to health.
Creamy milk with velvety texture. Dark with sprinkles of sea salt. Crunchy hazelnut-studded chunks. Chocolate is a treat that appeals to billions of people worldwide, no matter the age. And it’s not only the taste, but the feel of a chocolate morsel slowly melting in our mouths—the smoothness and slipperiness—that’s part of the overwhelming satisfaction. Why is it so enjoyable?
That’s what an interdisciplinary research team of chocolate lovers from the University of Leeds School of Food Science and Nutrition and School of Mechanical Engineering in the U.K. resolved to study in 2021. They wanted to know, “What is making chocolate that desirable?” says Siavash Soltanahmadi, one of the lead authors of a new study about chocolates hedonistic quality.
Besides addressing the researchers’ general curiosity, their answers might help chocolate manufacturers make the delicacy even more enjoyable and potentially healthier. After all, chocolate is a billion-dollar industry. Revenue from chocolate sales, whether milk or dark, is forecasted to grow 13 percent by 2027 in the U.K. In the U.S., chocolate and candy sales increased by 11 percent from 2020 to 2021, on track to reach $44.9 billion by 2026. Figuring out how chocolate affects the human palate could up the ante even more.
Building a 3D tongue
The team began by building a 3D tongue to analyze the physical process by which chocolate breaks down inside the mouth.
As part of the effort, reported earlier this year in the scientific journal ACS Applied Materials and Interfaces, the team studied a large variety of human tongues with the intention to build an “average” 3D model, says Soltanahmadi, a lubrication scientist. When it comes to edible substances, lubrication science looks at how food feels in the mouth and can help design foods that taste better and have more satisfying texture or health benefits.
There are variations in how people enjoy chocolate; some chew it while others “lick it” inside their mouths.
Tongue impressions from human participants studied using optical imaging helped the team build a tongue with key characteristics. “Our tongue is not a smooth muscle, it’s got some texture, it has got some roughness,” Soltanahmadi says. From those images, the team came up with a digital design of an average tongue and, using 3D printed molds, built a “mimic tongue.” They also added elastomers—such as silicone or polyurethane—to mimic the roughness, the texture and the mechanical properties of a real tongue. “Wettability" was another key component of the 3D tongue, Soltanahmadi says, referring to whether a surface mixes with water (hydrophilic) or, in the case of oil, resists it (hydrophobic).
Notably, the resulting artificial 3D-tongues looked nothing like the human version, but they were good mimics. The scientists also created “testing kits” that produced data on various physical parameters. One such parameter was viscosity, the measure of how gooey a food or liquid is — honey is more viscous compared to water, for example. Another was tribology, which defines how slippery something is — high fat yogurt is more slippery than low fat yogurt; milk can be more slippery than water. The researchers then mixed chocolate with artificial saliva and spread it on the 3D tongue to measure the tribology and the viscosity. From there they were able to study what happens inside the mouth when we eat chocolate.
The team focused on the stages of lubrication and the location of the fat in the chocolate, a process that has rarely been researched.
The artificial 3D-tongues look nothing like human tongues, but they function well enough to do the job.
Courtesy Anwesha Sarkar and University of Leeds
The oral processing of chocolate
We process food in our mouths in several stages, Soltanahmadi says. And there is variation in these stages depending on the type of food. So, the oral processing of a piece of meat would be different from, say, the processing of jelly or popcorn.
There are variations with chocolate, in particular; some people chew it while others use their tongues to explore it (within their mouths), Soltanahmadi explains. “Usually, from a consumer perspective, what we find is that if you have a luxury kind of a chocolate, then people tend to start with licking the chocolate rather than chewing it.” The researchers used a luxury brand of dark chocolate and focused on the process of licking rather than chewing.
As solid cocoa particles and fat are released, the emulsion envelops the tongue and coats the palette creating a smooth feeling of chocolate all over the mouth. That tactile sensation is part of the chocolate’s hedonistic appeal we crave.
Understanding the make-up of the chocolate was also an important step in the study. “Chocolate is a composite material. So, it has cocoa butter, which is oil, it has some particles in it, which is cocoa solid, and it has sugars," Soltanahmadi says. "Dark chocolate has less oil, for example, and less sugar in it, most of the time."
The researchers determined that the oral processing of chocolate begins as soon as it enters a person’s mouth; it starts melting upon exposure to one’s body temperature, even before the tongue starts moving, Soltanahmadi says. Then, lubrication begins. “[Saliva] mixes with the oily chocolate and it makes an emulsion." An emulsion is a fluid with a watery (or aqueous) phase and an oily phase. As chocolate breaks down in the mouth, that solid piece turns into a smooth emulsion with a fatty film. “The oil from the chocolate becomes droplets in a continuous aqueous phase,” says Soltanahmadi. In other words, as solid cocoa particles and fat are released, the emulsion envelops the tongue and coats the palette, creating a smooth feeling of chocolate all over the mouth. That tactile sensation is part of the chocolate’s hedonistic appeal we crave, says Soltanahmadi.
Finding the sweet spot
After determining how chocolate is orally processed, the research team wanted to find the exact sweet spot of the breakdown of solid cocoa particles and fat as they are released into the mouth. They determined that the epicurean pleasure comes only from the chocolate's outer layer of fat; the secondary fatty layers inside the chocolate don’t add to the sensation. It was this final discovery that helped the team determine that it might be possible to produce healthier chocolate that would contain less oil, says Soltanahmadi. And therefore, less fat.
Rongjia Tao, a physicist at Temple University in Philadelphia, thinks the Leeds study and the concept behind it is “very interesting.” Tao, himself, did a study in 2016 and found he could reduce fat in milk chocolate by 20 percent. He believes that the Leeds researchers’ discovery about the first layer of fat being more important for taste than the other layer can inform future chocolate manufacturing. “As a scientist I consider this significant and an important starting point,” he says.
Chocolate is rich in polyphenols, naturally occurring compounds also found in fruits and vegetables, such as grapes, apples and berries. Research found that plant polyphenols can protect against cancer, diabetes and osteoporosis as well as cardiovascular ad neurodegenerative diseases.
Not everyone thinks it’s a good idea, such as chef Michael Antonorsi, founder and owner of Chuao Chocolatier, one of the leading chocolate makers in the U.S. First, he says, “cacao fat is definitely a good fat.” Second, he’s not thrilled that science is trying to interfere with nature. “Every time we've tried to intervene and change nature, we get things out of balance,” says Antonorsi. “There’s a reason cacao is botanically known as food of the gods. The botanical name is the Theobroma cacao: Theobroma in ancient Greek, Theo is God and Brahma is food. So it's a food of the gods,” Antonorsi explains. He’s doubtful that a chocolate made only with a top layer of fat will produce the same epicurean satisfaction. “You're not going to achieve the same sensation because that surface fat is going to dissipate and there is no fat from behind coming to take over,” he says.
Without layers of fat, Antonorsi fears the deeply satisfying experiential part of savoring chocolate will be lost. The University of Leeds team, however, thinks that it may be possible to make chocolate healthier - when consumed in limited amounts - without sacrificing its taste. They believe the concept of less fatty but no less slick chocolate will resonate with at least some chocolate-makers and consumers, too.
Chocolate already contains some healthful compounds. Its cocoa particles have “loads of health benefits,” says Soltanahmadi. Dark chocolate usually has more cocoa than milk chocolate. Some experts recommend that dark chocolate should contain at least 70 percent cocoa in order for it to offer some health benefit. Research has shown that the cocoa in chocolate is rich in polyphenols, naturally occurring compounds also found in fruits and vegetables, such as grapes, apples and berries. Research has shown that consuming plant polyphenols can be protective against cancer, diabetes and osteoporosis as well as cardiovascular and neurodegenerative diseases.
“So keeping the healthy part of it and reducing the oily part of it, which is not healthy, but is giving you that indulgence of it … that was the final aim,” Soltanahmadi says. He adds that the team has been approached by individuals in the chocolate industry about their research. “Everyone wants to have a healthy chocolate, which at the same time tastes brilliant and gives you that self-indulging experience.”

In today's podcast episode, law professor Gaia Bernstein talks about the challenges of keeping control over our thoughts and actions, even when some powerful forces are pushing in the other direction.
Gaia’s book is called Unwired: Gaining Control Over Addictive Technologies. It’s fascinating and I had a chance to talk with her about it for today’s podcast. At its heart, our conversation is really about how and whether we can maintain control over our thoughts and actions, even when some powerful forces are pushing in the other direction.
Listen on Apple | Listen on Spotify | Listen on Stitcher | Listen on Amazon | Listen on Google
We discuss the idea that, in certain situations, maybe it's not reasonable to expect that we’ll be able to enjoy personal freedom and autonomy. We also talk about how to be a good parent when it sometimes seems like our kids prefer to be raised by their iPads; so-called educational video games that actually don’t have anything to do with education; the root causes of tech addictions for people of all ages; and what kinds of changes we should be supporting.
Gaia is Seton’s Hall’s Technology, Privacy and Policy Professor of Law, as well as Co-Director of the Institute for Privacy Protection, and Co-Director of the Gibbons Institute of Law Science and Technology. She’s the founding director of the Institute for Privacy Protection. She created and spearheaded the Institute’s nationally recognized Outreach Program, which educated parents and students about technology overuse and privacy.
Professor Bernstein's scholarship has been published in leading law reviews including the law reviews of Vanderbilt, Boston College, Boston University, and U.C. Davis. Her work has been selected to the Stanford-Yale Junior Faculty Forum and received extensive media coverage. Gaia joined Seton Hall's faculty in 2004. Before that, she was a fellow at the Engelberg Center of Innovation Law & Policy and at the Information Law Institute of the New York University School of Law. She holds a J.S.D. from the New York University School of Law, an LL.M. from Harvard Law School, and a J.D. from Boston University.
Gaia’s work on this topic is groundbreaking I hope you’ll listen to the conversation and then consider pre-ordering her new book. It comes out on March 28.


Rakhi Patel is among an increasing number of health care professionals, including doctors and nurses, who maintain an active persona on Instagram, TikTok and other social media sites.
“Health care professionals are quite prevalent on social media,” said Mercer Gary, a postdoctoral researcher at The Hastings Center, an independent bioethics research institute in Garrison, New York. “They’ve been posting on #medTwitter for many years, mainly to communicate with one another, but, of course, anyone can see the threads. Most recently, doctors and nurses have become a presence on TikTok.”
On social media, many health care providers perceive themselves to be “humanizing” their profession by coming across as more approachable — “reminding patients that providers are people and workers, as well as repositories of medical expertise,” Gary said. As a result, she noted that patients who are often intimidated by clinicians may feel comfortable enough to overcome barriers to scheduling health care appointments. The use of TikTok in particular may help doctors and nurses connect with younger followers.
When health care providers post on social media, they must bear in mind that they have legal and ethical duties to their patients, profession and society, said Elizabeth Levy, founder and director of Physicians for Justice.
While enduring three years of pandemic conditions, many health care professionals have struggled with burnout, exhaustion and moral distress. “Much health care provider content on social media seeks to expose the difficulties of the work,” Gary added. “TikTok and Instagram reels have shown health care providers crying after losing a patient or exhausted after a night shift in the emergency department.”
A study conducted in Beijing, China and published last year found that TikTok is the world’s most rapidly growing video application, amassing 1.6 billion users in 2021. “More and more patients are searching for information on genitourinary cancers via TikTok,” the study’s authors wrote in Frontiers in Oncology, referring to cancers of the urinary tracts and male reproductive organs. Among the 61 sample videos examined by the researchers, health care practitioners contributed the content in 29, or 47 percent, of them. Yet, 22 posts, 36 percent, were misinformative, mostly due to outdated information.
More than half of the videos offered good content on disease symptoms and examinations. The authors concluded that “most videos on genitourinary cancers on TikTok are of poor to medium quality and reliability. However, videos posted by media agencies enjoyed great public attention and interaction. Medical practitioners could improve the video quality by cooperating with media agencies and avoiding unexplained terminologies.”
When health care providers post on social media, they must bear in mind that they have legal and ethical duties to their patients, profession and society, said Elizabeth Levy, founder and director of Physicians for Justice in Irvine, Calif., a nonprofit network of volunteer physicians partnering with public interest lawyers to address the social determinants of health.
“Providers are also responsible for understanding the mechanics of their posts,” such as who can see these messages and how long they stay up, Levy said. As a starting point for figuring what’s acceptable, providers could look at social media guidelines put out by their professional associations. Even beyond that, though, they must exercise prudent judgment. “As social media continues to evolve, providers will also need to stay updated with the changing risks and benefits of participation.”
Patients often research their providers online, so finding them on social media can help inform about values and approaches to care, said M. Sara Rosenthal, a professor and founding director of the program for bioethics and chair of the hospital ethics committee at the University of Kentucky College of Medicine.
Health care providers’ posts on social media also could promote patient education. They can advance informed consent and help patients navigate the risks and benefits of various treatments or preventive options. However, providers could violate ethical principles if they espouse “harmful, risky or questionable therapies or medical advice that is contrary to clinical practice guidelines or accepted standards of care,” Rosenthal said.
Inappropriate self-disclosure also can affect a provider’s reputation, said Kelly Michelson, a professor of pediatrics and director of the Center for Bioethics and Medical Humanities at Northwestern University’s Feinberg School of Medicine. A clinician’s obligations to professionalism extend beyond those moments when they are directly taking care of their patients, she said. “Many experts recommend against clinicians ‘friending’ patients or the families on social media because it blurs the patient-clinician boundary.”
Meanwhile, clinicians need to adhere closely to confidentiality. In sharing a patient’s case online for educational purposes, safeguarding identity becomes paramount. Removing names and changing minor details is insufficient, Michelson said.
“The patient-clinician relationship is sacred, and it can only be effective if patients have 100 percent confidence that all that happens with their clinician is kept in the strictest of confidence,” she said, adding that health care providers also should avoid obtaining information about their patients from social media because it can lead to bias and risk jeopardizing objectivity.
Academic clinicians can use social media as a recruitment tool to expand the pool of research participants for their studies, Michelson said. Because the majority of clinical research is conducted at academic medical centers, large segments of the population are excluded. “This affects the quality of the data and knowledge we gain from research,” she said.
Don S. Dizon, a professor of medicine and surgery at the Warren Alpert Medical School of Brown University in Providence, Rhode Island, uses LinkedIn and Doximity, as well as Twitter, Instagram, TikTok, Facebook, and most recently, YouTube and Post. He’s on Twitter nearly every day, where he interacts with the oncology community and his medical colleagues.
Also, he said, “I really like Instagram. It’s where you will see a hybrid of who I am professionally and personally. I’ve become comfortable sharing both up to a limit, but where else can I combine my appreciation of clothes with my professional life?” On that site, he’s seen sporting shirts with polka dots or stripes and an occasional bow-tie. He also posts photos of his cats.

Don S. Dizon, a professor of medicine and surgery at Brown, started using TikTok several years ago, telling medical stories in short-form videos.
Don S. Dizon
Dizon started using TikTok several years ago, telling medical stories in short-form videos. He may talk about an inspirational patient, his views on end-of-life care and death, or memories of people who have passed. But he is careful not to divulge any details that would identify anyone.
Recently, some people have become his patients after viewing his content on social media or on the Internet in general, which he clearly states isn’t a forum for medical advice. “In both situations, they are so much more relaxed when we meet, because it’s as if they have a sense of who I am as a person,” Dizon said. “I think that has helped so much in talking through a cancer diagnosis and a treatment plan, and yes, even discussions about prognosis.”
He also posts about equity and diversity. “I have found myself more likely to repost or react to issues that are inherently political, including racism, homophobia, transphobia and lack-of-access issues, because medicine is not isolated from society, and I truly believe that medicine is a social justice issue,” said Dizon, who is vice chair of diversity, equity, inclusion and professional integrity at the SWOG Cancer Research Network.
Through it all, Dizon likes “to break through the notion of doctor as infallible and all-knowing, the doctor as deity,” he said. “Humanizing what I do, especially in oncology, is something that challenges me on social media, and I appreciate the opportunities to do it on TikTok.”