

Drones are just one of several new technologies that are rising to the challenge of more frequent wildfires.
Robots have been a game-changer. Inspired by Paris, the Los Angeles Fire Department (LAFD) was the first in the U.S. to deploy a firefighting robot in 2021, the Thermite Robotics System 3 – RS3, for short.
RS3 is a 3,500-pound turbine on a crawler—the size of a Smart car—with a 36.8 horsepower engine that can go for 20 hours without refueling. It can plow through hazardous terrain, move cars from its path, and pull an 8,000-pound object from a fire.
All that while spurting 2,500 gallons of water per minute with a rear exhaust fan clearing the smoke. At a recent trade show, RS3 was billed as equivalent to 10 firefighters. The Los Angeles Times referred to it as “a droid on steroids.”

Robots such as the Thermite RS3 can plow through hazardous terrain and pull an 8,000-pound object from a fire.
Los Angeles Fire Department
The advantage of the robot is obvious. Operated remotely from a distance, it greatly reduces an emergency responder’s exposure to danger, says Wade White, assistant chief of the LAFD. The robot can be sent into airplane fires, nuclear reactors, hazardous areas with carcinogens (think East Palestine, Ohio), or buildings where a roof collapse is imminent.
Advances for firefighters are taking many other forms as well. Fibers have been developed that make the firefighter’s coat lighter and more protective from carcinogens. New wearable devices track firefighters’ biometrics in real time so commanders can monitor their heat stress and exertion levels. A sensor patch is in development which takes readings every four seconds to detect dangerous gases such as methane and carbon dioxide. A sonic fire extinguisher is being explored that uses low frequency soundwaves to remove oxygen from air molecules without unhealthy chemical compounds.
The demand for this technology is only increasing, especially with the recent rise in wildfires. In 2021, fires were responsible for 3,800 deaths and 14,700 injuries of civilians in this country. Last year, 68,988 wildfires burned down 7.6 million acres. Whether the next generation of firefighting can address these new challenges could depend on special cameras, robots of the aerial variety, AI and smart systems.
Fighting fire with cameras
Another key innovation for firefighters is a thermal imaging camera (TIC) that improves visibility through smoke. “At a fire, you might not see your hand in front of your face,” says White. “Using the TIC screen, you can find the door to get out safely or see a victim in the corner.” Since these cameras were introduced in the 1990s, the price has come down enough (from $10,000 or more to about $700) that every LAFD firefighter on duty has been carrying one since 2019, says White.
TICs are about the size of a cell phone. The camera can sense movement and body heat so it is ideal as a search tool for people trapped in buildings. If a firefighter has not moved in 30 seconds, the motion detector picks that up, too, and broadcasts a distress signal and directional information to others.
To enable firefighters to operate the camera hands-free, the newest TICs can attach inside a helmet. The firefighter sees the images inside their mask.
TICs also can be mounted on drones to get a bird’s-eye, 360 degree view of a disaster or scout for hot spots through the smoke. In addition, the camera can take photos to aid arson investigations or help determine the cause of a fire.
More help From above
Firefighters prefer the term “unmanned aerial systems” (UAS) to drones to differentiate them from military use.
A UAS carrying a camera can provide aerial scene monitoring and topography maps to help fire captains deploy resources more efficiently. At night, floodlights from the drone can illuminate the landscape for firefighters. They can drop off payloads of blankets, parachutes, life preservers or radio devices for stranded people to communicate, too. And like the robot, the UAS reduces risks for ground crews and helicopter pilots by limiting their contact with toxic fumes, hazardous chemicals, and explosive materials.
“The nice thing about drones is that they perform multiple missions at once,” says Sean Triplett, team lead of fire and aviation management, tools and technology at the Forest Service.
Experts predict we’ll see swarms of drones dropping water and fire retardant on burning buildings and forests in the near future.
The UAS is especially helpful during wildfires because it can track fires, get ahead of wind currents and warn firefighters of wind shifts in real time. The U.S. Forest Service also uses long endurance, solar-powered drones that can fly for up to 30 days at a time to detect early signs of wildfire. Wildfires are no longer seasonal in California – they are a year-long threat, notes Thanh Nguyen, fire captain at the Orange County Fire Authority.
In March, Nguyen’s crew deployed a drone to scope out a huge landslide following torrential rains in San Clemente, CA. Emergency responders used photos and videos from the drone to survey the evacuated area, enabling them to stay clear of ground on the hillside that was still sliding.
Improvements in drone batteries are enabling them to fly for longer with heavier payloads. Experts predict we’ll see swarms of drones dropping water and fire retardant on burning buildings and forests in the near future.
AI to the rescue
The biggest peril for a firefighter is often what they don’t see coming. Flashovers are a leading cause of firefighter deaths, for example. They occur when flammable materials in an enclosed area ignite almost instantaneously. Or dangerous backdrafts can happen when a firefighter opens a window or door; the air rushing in can ignite a fire without warning.
The Fire Fighting Technology Group at the National Institute of Standards and Technology (NIST) is developing tools and systems to predict these potentially lethal events with computer models and artificial intelligence.
Partnering with other institutions, NIST researchers developed the Flashover Prediction Neural Network (FlashNet) after looking at common house layouts and running sets of scenarios through a machine-learning model. In the lab, FlashNet was able to predict a flashover 30 seconds before it happened with 92.1% success. When ready for release, the technology will be bundled with sensors that are already installed in buildings, says Anthony Putorti, leader of the NIST group.
The NIST team also examined data from hundreds of backdrafts as a basis for a machine-learning model to predict them. In testing chambers the model predicted them correctly 70.8% of the time; accuracy increased to 82.4% when measures of backdrafts were taken in more positions at different heights in the chambers. Developers are working on how to integrate the AI into a small handheld device that can probe the air of a room through cracks around a door or through a created opening, Putorti says. This way, the air can be analyzed with the device to alert firefighters of any significant backdraft risk.
Early wildfire detection technologies based on AI are in the works, too. The Forest Service predicts the acreage burned each year during wildfires will more than triple in the next 80 years. By gathering information on historic fires, weather patterns, and topography, says White, AI can help firefighters manage wildfires before they grow out of control and create effective evacuation plans based on population data and fire patterns.
The future is connectivity
We are in our infancy with “smart firefighting,” says Casey Grant, executive director emeritus of the Fire Protection Research Foundation. Grant foresees a new era of cyber-physical systems for firefighters—a massive integration of wireless networks, advanced sensors, 3D simulations, and cloud services. To enhance teamwork, the system will connect all branches of emergency responders—fire, emergency medical services, law enforcement.
FirstNet (First Responder Network Authority) now provides a nationwide high-speed broadband network with 5G capabilities for first responders through a terrestrial cell network. Battling wildfires, however, the Forest Service needed an alternative because they don’t always have access to a power source. In 2022, they contracted with Aerostar for a high altitude balloon (60,000 feet up) that can extend cell phone power and LTE. “It puts a bubble of connectivity over the fire to hook in the internet,” Triplett explains.
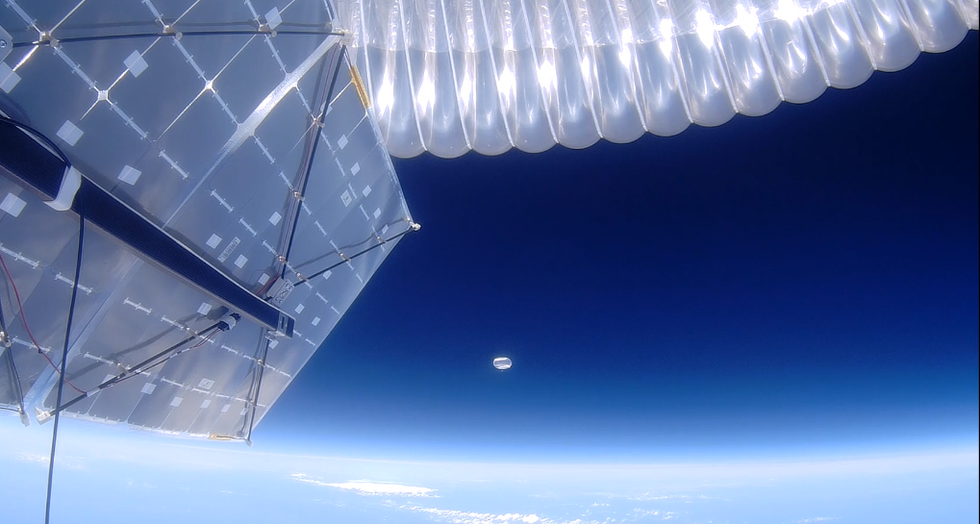
A high altitude balloon, 60,000 feet high, can extend cell phone power and LTE, putting a "bubble" of internet connectivity over fires.
Courtesy of USDA Forest Service
Advances in harvesting, processing and delivering data will improve safety and decision-making for firefighters, Grant sums up. Smart systems may eventually calculate fire flow paths and make recommendations about the best ways to navigate specific fire conditions. NIST’s plan to combine FlashNet with sensors is one example.
The biggest challenge is developing firefighting technology that can work across multiple channels—federal, state, local and tribal systems as well as for fire, police and other emergency services— in any location, says Triplett. “When there’s a wildfire, there are no political boundaries,” he says. “All hands are on deck.”


In the U.S., hospitals generate an estimated 6,000 tons of waste per day. A few clinics are leading the way in transitioning to clean energy sources.
She decided to research alternatives for plastic in the medical sector and learned that cups could be reused and easily disinfected. All dentists routinely disinfect their tools anyway and, Stroetzel reasoned, it wouldn’t be too hard to extend that practice to cups.
It's a good example for how often plastic is used unnecessarily in medical practice, she says. The health care sector is the fifth biggest source of pollution and trash in industrialized countries. In the U.S., hospitals generate an estimated 6,000 tons of waste per day, including an average of 400 grams of plastic per patient per day, and this sector produces 8.5 percent of greenhouse gas emissions nationwide.
“Sustainable alternatives exist,” Stroetzel says, “but you have to painstakingly look for them; they are often not offered by the big manufacturers, and all of this takes way too much time [that] medical staff simply does not have during their hectic days.”
When Stroetzel spoke with medical staff in Germany, she found they were often frustrated by all of this waste, especially as they took care to avoid single-use plastic at home. Doctors in other countries share this frustration. In a recent poll, nine out of ten doctors in Germany said they’re aware of the urgency to find sustainable solutions in the health industry but don’t know how to achieve this goal.
After a year of researching more sustainable alternatives, Stroetzel founded a social enterprise startup called POP, short for Practice Without Plastic, together with IT expert Nicolai Niethe, to offer well-researched solutions. “Sustainable alternatives exist,” she says, “but you have to painstakingly look for them; they are often not offered by the big manufacturers, and all of this takes way too much time [that] medical staff simply does not have during their hectic days.”
In addition to reusable dentist cups, other good options for the heath care sector include washable N95 face masks and gloves made from nitrile, which waste less water and energy in their production. But Stroetzel admits that truly making a medical facility more sustainable is a complex task. “This includes negotiating with manufacturers who often package medical materials in double and triple layers of extra plastic.”
While initiatives such as Stroetzel’s provide much needed information, other experts reason that a wholesale rethinking of healthcare is needed. Voluntary action won’t be enough, and government should set the right example. Kari Nadeau, a Stanford physician who has spent 30 years researching the effects of environmental pollution on the immune system, and Kenneth Kizer, the former undersecretary for health in the U.S. Department of Veterans Affairs, wrote in JAMA last year that the medical industry and federal agencies that provide health care should be required to measure and make public their carbon footprints. “Government health systems do not disclose these data (and very rarely do private health care organizations), unlike more than 90% of the Standard & Poor’s top 500 companies and many nongovernment entities," they explained. "This could constitute a substantial step toward better equipping health professionals to confront climate change and other planetary health problems.”
Compared to the U.K., the U.S. healthcare industry lags behind in terms of measuring and managing its carbon footprint, and hospitals are the second highest energy user of any sector in the U.S.
Kizer and Nadeau look to the U.K. National Health Service (NHS), which created a Sustainable Development Unit in 2008 and began that year to conduct assessments of the NHS’s carbon footprint. The NHS also identified its biggest culprits: Of the 2019 footprint, with emissions totaling 25 megatons of carbon dioxide equivalent, 62 percent came from the supply chain, 24 percent from the direct delivery of care, 10 percent from staff commute and patient and visitor travel, and 4 percent from private health and care services commissioned by the NHS. From 1990 to 2019, the NHS has reduced its emission of carbon dioxide equivalents by 26 percent, mostly due to the switch to renewable energy for heat and power. Meanwhile, the NHS has encouraged health clinics in the U.K. to install wind generators or photovoltaics that convert light to electricity -- relatively quick ways to decarbonize buildings in the health sector.
Compared to the U.K., the U.S. healthcare industry lags behind in terms of measuring and managing its carbon footprint, and hospitals are the second highest energy user of any sector in the U.S. “We are already seeing patients with symptoms from climate change, such as worsened respiratory symptoms from increased wildfires and poor air quality in California,” write Thomas B. Newman, a pediatrist at the University of California, San Francisco, and UCSF clinical research coordinator Daisy Valdivieso. “Because of the enormous health threat posed by climate change, health professionals should mobilize support for climate mitigation and adaptation efforts.” They believe “the most direct place to start is to approach the low-lying fruit: reducing healthcare waste and overuse.”
In addition to resulting in waste, the plastic in hospitals ultimately harms patients, who may be even more vulnerable to the effects due to their health conditions. Microplastics have been detected in most humans, and on average, a human ingests five grams of microplastic per week. Newman and Valdivieso refer to the American Board of Internal Medicine's Choosing Wisely program as one of many initiatives that identify and publicize options for “safely doing less” as a strategy to reduce unnecessary healthcare practices, and in turn, reduce cost, resource use, and ultimately reduce medical harm.
A few U.S. clinics are pioneers in transitioning to clean energy sources. In Wisconsin, the nonprofit Gundersen Health network became the first hospital to cut its reliance on petroleum by switching to locally produced green energy in 2015, and it saved $1.2 million per year in the process. Kaiser Permanente eliminated its 800,000 ton carbon footprint through energy efficiency and purchasing carbon offsets, reaching a balance between carbon emissions and removing carbon from the atmosphere in 2020, the first U.S. health system to do so.
Cleveland Clinic has pledged to join Kaiser in becoming carbon neutral by 2027. Realizing that 80 percent of its 2008 carbon emissions came from electricity consumption, the Clinic started switching to renewable energy and installing solar panels, and it has invested in researching recyclable products and packaging. The Clinic’s sustainability report outlines several strategies for producing less waste, such as reusing cases for sterilizing instruments, cutting back on materials that can’t be recycled, and putting pressure on vendors to reduce product packaging.
The Charité Berlin, Europe’s biggest university hospital, has also announced its goal to become carbon neutral. Its sustainability managers have begun to identify the biggest carbon culprits in its operations. “We’ve already reduced CO2 emissions by 21 percent since 2016,” says Simon Batt-Nauerz, the director of infrastructure and sustainability.
The hospital still emits 100,000 tons of CO2 every year, as much as a city with 10,000 residents, but it’s making progress through ride share and bicycle programs for its staff of 20,000 employees, who can get their bikes repaired for free in one of the Charité-operated bike workshops. Another program targets doctors’ and nurses’ scrubs, which cause more than 200 tons of CO2 during manufacturing and cleaning. The staff is currently testing lighter, more sustainable scrubs made from recycled cellulose that is grown regionally and requires 80 percent less land use and 30 percent less water.

The Charité hospital in Berlin still emits 100,000 tons of CO2 every year, but it’s making progress through ride share and bicycle programs for its staff of 20,000 employees.
Wiebke Peitz | Specific to Charité
Anesthesiologist Susanne Koch spearheads sustainability efforts in anesthesiology at the Charité. She says that up to a third of hospital waste comes from surgery rooms. To reduce medical waste, she recommends what she calls the 5 Rs: Reduce, Reuse, Recycle, Rethink, Research. “In medicine, people don’t question the use of plastic because of safety concerns,” she says. “Nobody wants to be sued because something is reused. However, it is possible to reduce plastic and other materials safely.”
For instance, she says, typical surgery kits are single-use and contain more supplies than are actually needed, and the entire kit is routinely thrown out after the surgery. “Up to 20 percent of materials in a surgery room aren’t used but will be discarded,” Koch says. One solution could be smaller kits, she explains, and another would be to recycle the plastic. Another example is breathing tubes. “When they became scarce during the pandemic, studies showed that they can be used seven days instead of 24 hours without increased bacteria load when we change the filters regularly,” Koch says, and wonders, “What else can we reuse?”
In the Netherlands, TU Delft researchers Tim Horeman and Bart van Straten designed a method to melt down the blue polypropylene wrapping paper that keeps medical instruments sterile, so that the material can be turned it into new medical devices. Currently, more than a million kilos of the blue paper are used in Dutch hospitals every year. A growing number of Dutch hospitals are adopting this approach.
Another common practice that’s ripe for improvement is the use of a certain plastic, called PVC, in hospital equipment such as blood bags, tubes and masks. Because of its toxic components, PVC is almost never recycled in the U.S., but University of Michigan researchers Danielle Fagnani and Anne McNeil have discovered a chemical process that can break it down into material that could be incorporated back into production. This could be a step toward a circular economy “that accounts for resource inputs and emissions throughout a product’s life cycle, including extraction of raw materials, manufacturing, transport, use and reuse, and disposal,” as medical experts have proposed. “It’s a failure of humanity to have created these amazing materials which have improved our lives in many ways, but at the same time to be so shortsighted that we didn’t think about what to do with the waste,” McNeil said in a press release.
Susanne Koch puts it more succinctly: “What’s the point if we save patients while killing the planet?”