
How Excessive Regulation Helped Ignite COVID-19's Rampant Spread
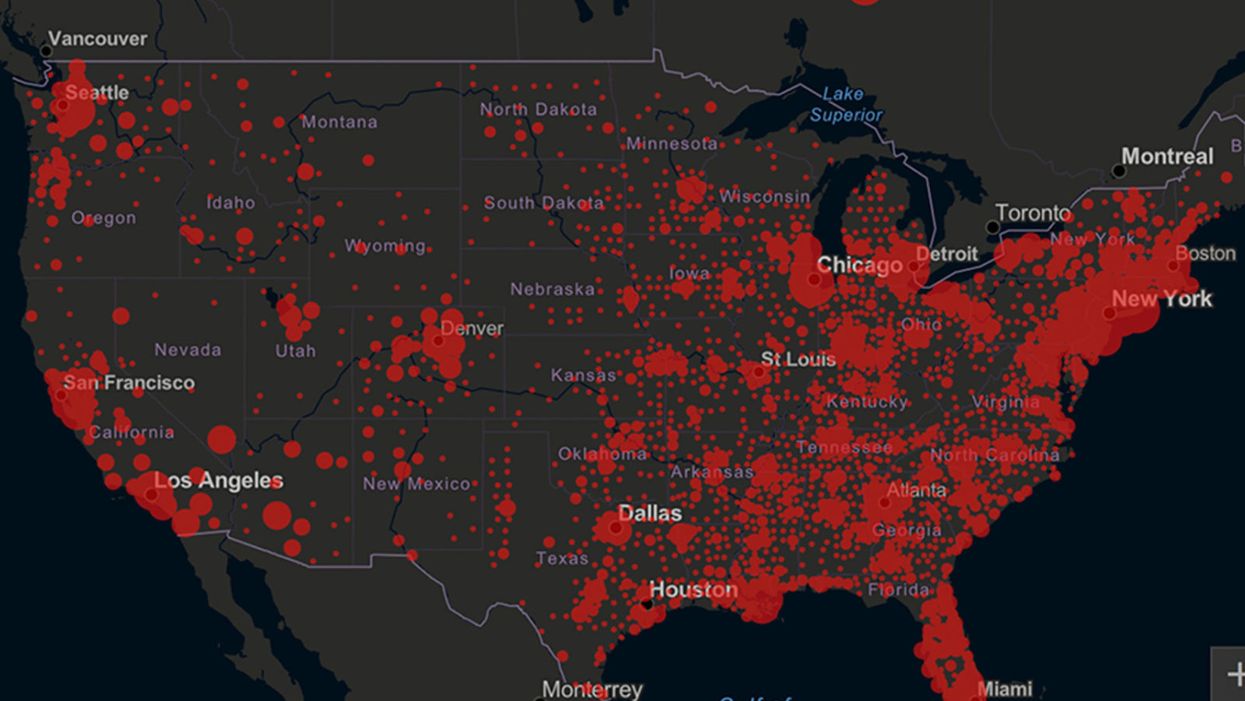
Screenshot of an interactive map of coronavirus cases across the United States, current as of 1:45 p.m. Pacific time on Tuesday, March 31st. Full map accessible at https://coronavirus.jhu.edu/map.html
When historians of the future look back at the 2020 pandemic, the heroic work of Helen Y. Chu, a flu researcher at the University of Washington, will be worthy of recognition.
Chu's team bravely defied the order and conducted the testing anyway.
In late January, Chu was testing nasal swabs for the Seattle Flu Study to monitor influenza spread when she learned of the first case of COVID-19 in Washington state. She deemed it a pressing public health matter to document if and how the illness was spreading locally, so that early containment efforts could succeed. So she sought regulatory approval to adapt the Flu Study to test for the coronavirus, but the federal government denied the request because the original project was funded to study only influenza.
Aware of the urgency, Chu's team bravely defied the order and conducted the testing anyway. Soon they identified a local case in a teenager without any travel history, followed by others. Still, the government tried to shutter their efforts until the outbreak grew dangerous enough to command attention.
Needless testing delays, prompted by excessive regulatory interference, eliminated any chances of curbing the pandemic at its initial stages. Even after Chu went out on a limb to sound alarms, a heavy-handed bureaucracy crushed the nation's ability to roll out early and widespread testing across the country. The Centers for Disease Control and Prevention infamously blundered its own test, while also impeding state and private labs from coming on board, fueling a massive shortage.
The long holdup created "a backlog of testing that needed to be done," says Amesh Adalja, an infectious disease specialist who is a senior scholar at the Johns Hopkins University Center for Health Security.
In a public health crisis, "the ideal situation" would allow the government's test to be "supplanted by private laboratories" without such "a lag in that transition," Adalja says. Only after the eventual release of CDC's test could private industry "begin in earnest" to develop its own versions under the Food and Drug Administration's emergency use authorization.
In a statement, CDC acknowledged that "this process has not gone as smoothly as we would have liked, but there is currently no backlog for testing at CDC."
Now, universities and corporations are in a race against time, playing catch up as the virus continues its relentless spread, also afflicting many health care workers on the front lines.
"Home-testing accessibility is key to preventing further spread of the COVID-19 pandemic."
Hospitals are attempting to add the novel coronavirus to the testing panel of their existent diagnostic machines, which would reduce the results processing time from 48 hours to as little as four hours. Meanwhile, at least four companies announced plans to deliver at-home collection tests to help meet the demand – before a startling injunction by the FDA halted their plans.
Everlywell, an Austin, Texas-based digital health company, had been set to launch online sales of at-home collection kits directly to consumers last week. Scaling up in a matter of days to an initial supply of 30,000 tests, Everlywell collaborated with multiple laboratories where consumers could ship their nasal swab samples overnight, projecting capacity to screen a quarter-million individuals on a weekly basis, says Frank Ong, chief medical and scientific officer.
Secure digital results would have been available online within 48 hours of a sample's arrival at the lab, as well as a telehealth consultation with an independent, board-certified doctor if someone tested positive, for an inclusive $135 cost. The test has a less than 3 percent false-negative rate, Ong says, and in the event of an inadequate self-swab, the lab would not report a conclusive finding. "Home-testing accessibility," he says, "is key to preventing further spread of the COVID-19 pandemic."
But on March 20, the FDA announced restrictions on home collection tests due to concerns about accuracy. The agency did note "the public health value in expanding the availability of COVID-19 testing through safe and accurate tests that may include home collection," while adding that "we are actively working with test developers in this space."
After the restrictions were announced, Everlywell decided to allocate its initial supply of COVID-19 collection kits to hospitals, clinics, nursing homes, and other qualifying health care companies that can commit to no-cost screening of frontline workers and high-risk symptomatic patients. For now, no consumers can order a home-collection test.
"Losing two months is close to disastrous, and that's what we did."
Currently, the U.S. has ramped up to testing an estimated 100,000 people a day, according to Stat News. But 150,000 or more Americans should be tested every day, says Ashish Jha, professor and director of the Harvard Global Health Institute. Due to the dearth of tests, many sick people who suspect they are infected still cannot get confirmation unless they need to be hospitalized.
To give a concrete sense of how far behind we are in testing, consider Palm Beach County, Fla. The state's only drive-thru test center just opened there, requiring an appointment. The center aims to test 750 people per day, but more than 330,000 people have already called to try to book a slot.
"This is such a rapidly moving infection that losing a few days is bad, and losing a couple of weeks is terrible," says Jha, a practicing general internist. "Losing two months is close to disastrous, and that's what we did."
At this point, it will take a long time to fully ramp up. "We are blindfolded," he adds, "and I'd like to take the blindfolds off so we can fight this battle with our eyes wide open."
Better late than never: Yesterday, FDA Commissioner Stephen Hahn said in a statement that the agency has worked with more than 230 test developers and has approved 20 tests since January. An especially notable one was authorized last Friday – 67 days since the country's first known case in Washington state. It's a rapid point-of-care test from medical-device firm Abbott that provides positive results in five minutes and negative results in 13 minutes. Abbott will send 50,000 tests a day to urgent care settings. The first tests are expected to ship tomorrow.
Should egg and sperm donors reveal their identities? The debate pivots on genetics and medical history.

Cassandra Adams performs on stage at the Jersey City Theater Center in March 2019 to raise awareness about traumatic experiences that she and others have had with anonymous donor conception.
Until age 35, Cassandra Adams assumed her mother and father were her biological parents. Then she took saliva tests through two genealogy databases—23andMe and AncestryDNA—and discovered a discrepancy in her heritage. In bringing up the matter with her parents, she learned that fertility issues had led the couple to use a sperm donor.
“Most people my age were not told,” said Adams, now 40 and a stay-at-home mom in Jersey City, New Jersey, who is involved with donor-conception advocacy. “Even now, there’s still a lot of secrecy in the industry. There are still many parents who aren’t truthful or planning not to be truthful with their children.”
While some of those offspring may never know a significant part of their medical history, Adams is grateful that she does. Surprisingly, the DNA test revealed Jewish ancestry.
“There are a lot more genetic conditions that run in Jewish families, so it was really important that I get my medical history, because it’s very different from my dad who raised me,” said Adams, who has met her biological father and two of three known half-siblings. As a result of this experience, she converted to Judaism. “It has been a big journey,” she said.
In an era of advancing assisted reproduction technologies, genetics and medical history have become front and center of the debate as to whether or not egg and sperm donations should be anonymous – and whether secrecy is even possible in many cases.
Obstacles to staying anonymous
People looking to become parents can choose what’s called an “identity-release donor,” meaning their child can receive information about the donor when he or she turns 18. There’s no way to ensure that the donor will consent to a relationship at that time. Instead, if a relationship between the donor and child is a priority, parents may decide to use a known donor.
The majority of donors want to remain anonymous, said reproductive endocrinologist Robert Kiltz, founder and director of CNY Fertility in Syracuse, New York. “In general, egg and sperm donation is mostly anonymous, meaning the recipient doesn’t know the donor and the donor doesn’t know the recipient.”
Even if the donor isn’t disclosed, though, the mystery may become unraveled when a donor-conceived person undergoes direct-to-consumer genetic testing through ancestry databases, which are growing in number and popularity. These services offer DNA testing and links to relatives with identifiable information.
In the future, another obstacle to anonymity could be laws that prohibit anonymous sperm and egg donations, if they catch on. In June, Colorado became the first state in the nation to ban anonymous sperm and egg donations. The law, which takes effect in 2025, will give donor-conceived adults the legal authority to obtain their donor’s identity and medical history. It also requires banks that provide sperm and egg collection to keep current medical records and contact information for all donors. Meanwhile, it prohibits donations from those who won’t consent to identity disclosures.
“The tradition of anonymous sperm or egg donation has created a vast array of problems, most significantly that the people thus created want to know who their mommy and daddy are,” said Kenneth W. Goodman, professor and director of the Institute for Bioethics and Health Policy at the University of Miami Miller School of Medicine.
“There are counter arguments on both sides. But the current situation has led to great uncertainty and, in many cases, grief,” Goodman said.
Donors should bear some moral responsibility for their role in reproduction by allowing their identity to be disclosed to donor-conceived individuals when they turn 18, Goodman added, noting that “there are counter arguments on both sides. But the current situation has led to great uncertainty and, in many cases, grief.”
Adams, the Jersey City woman who learned she was Jewish, has channeled these feelings into several works of art and performances on stage at venues such as the Jersey City Theater Center. During these performances, she describes the trauma of “not knowing where we come from [or] who we look like.”
In the last five years, Kathleen “Casey” DiPaola, a lawyer in Albany, New York, who focuses her practice on adoption, assisted reproduction and surrogacy, has observed a big shift toward would-be parents looking to use known sperm donors. On the other hand, with egg donation, “I’m not seeing a whole lot of change,” she said. Compared to sperm donation, more medical screening is involved with egg donation, so donors are primarily found through fertility clinics and egg donor agencies that prefer anonymity. This leads to fewer options for prospective parents seeking an egg donor with disclosed identity, DiPaola said.
Some donors want to keep in touch
Rachel Lemmons, 32, who lives in Denver, grew interested in becoming an egg donor when, as a graduate student in environmental sciences, she saw an online advertisement. “It seemed like a good way to help pay off my student loan debt,” said Lemmons, who is married and has a daughter who will turn 2-years-old in December. She didn’t end up donating until many years later, after she’d paid off the debt. “The primary motivation at that point wasn’t financial,” she said. “Instead, it felt like a really wonderful way to help someone else have a family in a few weeks’ time.”
Lemmons originally donated anonymously because she didn’t know open donations existed. She was content with that until she became aware of donor-conceived individuals’ struggles. “It concerned me that I could potentially be contributing to this,” she said, adding that the egg donor and surrogacy agency and fertility clinic wouldn’t allow her to disclose her identity retroactively.
Since then, she has donated as an open donor, and kept in touch with the recipients through email and video calls. Knowing that they were finally able to have children is “incredibly rewarding,” Lemmons said.
When to tell the kids
Stanton Honig, professor of urology and division chief of sexual and reproductive medicine at Yale School of Medicine, said for years his team has recommended that couples using donor sperm inform children about the role of the donor and their identity. “Honesty is always the best policy, and it is likely that when they become of age, they might or will be able to find out about their biological sperm donor,” he said. “Hiding it creates more of a complicated situation for children in the long run.”
Amy Jones, a 45-year-old resident of Syracuse, N.Y., has three children, including twins, who know they were conceived with anonymous donor eggs from the same individual, so they share the same genetics. Jones, who is a registered nurse and asked for her real name not to be published, told them around age seven.
“The thought of using a known donor brought more concerns—what if she wanted my babies after they were born, or how would I feel if she treated them as her own every time I saw her?” said Jones.
“I did a lot of reading, and all psychologists said that it is best to start the conversation early,” she recalled. “They understood very little of what I was telling them, but through the years, I have brought it up in discussion and encouraged them to ask questions. To this day, they don't seem to be all that interested, but I expect that later on in life they may have more questions.”
Jones and her husband opted to use a donor because premature ovarian failure at age 27 had rendered her infertile. “The decision to use an egg donor was hard enough,” she said. “The thought of using a known donor brought more concerns—what if she wanted my babies after they were born, or how would I feel if she treated them as her own every time I saw her?”
Susan C. Klock, a clinical psychologist in the section of fertility and reproductive medicine at Northwestern University Feinberg School of Medicine, said, “Anonymity is virtually impossible in the age of direct-to-consumer genetic testing.” In addition, “selecting an identity-release donor is typically not the first thing parents are looking at when they select a donor. First and foremost, they are looking for a donor with a healthy medical background. Then they may consider donor characteristics that resemble the parents.”
The donor’s medical history can be critical
Donor agencies rely on the self-reported medical history of egg and sperm donors, which can lead to gaps in learning important information. Knowing a donor’s medical history may have led some families to make different or more well-informed choices.
After Steven Gunner, a donor-conceived adult, suffered from schizophrenia and died of a drug overdose at age 27 in 2020, his parents, who live in New York, learned of a potential genetic link to his mental illness. A website, Donor Sibling Registry, revealed that the sperm donor the couple had used, a college student at the time of donation, had been hospitalized during childhood for schizophrenia and died of a drug overdose at age 46. Gunner’s story inspired Steven’s Law, a bill that was introduced in Congress in July. If passed, it would mandate sperm banks to collect information on donors’ medical conditions, and donors would have to disclose medical information the banks weren’t able to find.
With limited exceptions, the U.S. Food and Drug Administration requires donors to be screened and tested for relevant communicable disease agents and diseases such as HIV, hepatitis viruses B and C, the Zika virus and several STDs. With current technology, it is also impossible to screen for thousands of rare genetic diseases. “If a couple is using IVF (in vitro fertilization) to conceive with the donor gamete, some may opt for pre-implantation genetic testing to assess for chromosomal abnormalities,” Klock said.
Even these precautions wouldn't cover every disease, and some would-be parents don't get the genetic screening. In a situation where one donor has a large number of offspring, it is concerning that he or she can spread a rare disease to multiple people, said Nick Isel, 37, of Yorkville, Illinois, who was conceived with donor sperm due to his parents’ fertility issues. They told him the truth when he was a teenager, and he found his biological father with a journalist’s help.
Since 2016, Isel, who owns a roofing company, has been petitioning the FDA to extend the retention of medical records, requiring the fertility establishment to maintain information on sperm and egg donors for 50 years instead of the current 10-year mandate.
“The lack of family health information,” he said, “is an ongoing, slow-motion public health crisis since donor conception began being regulated by the FDA as a practice.”
Saliva May Help Diagnose PTSD in Veterans

A recent study finds that former soldiers with post traumatic stress disorders have a certain set of bacteria in their saliva, a distinct signature that is believed to be the first biological marker for PTSD.
As a bioinformatician and young veteran, Guy Shapira welcomed the opportunity to help with conducting a study to determine if saliva can reveal if war veterans have post-traumatic stress disorder, or PTSD.
The research team, which drew mostly from Tel Aviv University’s Sackler Faculty of Medicine and Sagol School of Neuroscience, collected saliva samples from approximately 200 veterans who suffered psychological trauma stemming from the years they spent fighting in the First Lebanon War in 1982. The researchers also characterized the participants’ psychological, social and medical conditions, including a detailed analysis of their microbiomes.
They found that the former soldiers with PTSD have a certain set of bacteria in their saliva, a distinct microbiotic signature that is believed to be the first biological marker for PTSD. The finding suggests that, in the future, saliva tests could be used to help identify this disorder. As of now, PTSD is often challenging to diagnose.
Shapira, a Ph.D. student at Tel Aviv University, was responsible for examining genetic and health-related data of the veterans who participated – information that had been compiled steadily over four decades. The veterans provided this data voluntarily, Shapira says, at least partly because the study carries important implications for their own psychological health.
The research was led by Illana Gozes, professor emerita of clinical biochemistry. “We looked at the bacteria in their blood and their saliva,” Gozes explains. To discover the microbial signatures, they analyzed the biometric data for each soldier individually and as a group. Comparing the results of the participants’ microbial distribution to the results of their psychological examinations and their responses to personal welfare questionnaires, the researchers learned that veterans with PTSD – and, more generally, those with significant mental health issues – have the same bacterial content in their saliva.
“Having empirical metrics to assess whether or not someone has PTSD can help veterans who make their case to the Army to get reparations,” Shapira says.
More research is required to support this finding, published in July in Nature’s prestigious Molecular Psychiatry, but it could have important implications for identifying people with PTSD. Currently, it can be diagnosed only through psychological and behavioral symptoms such as flashbacks, nightmares, sleep disorders, increased irritability and physical aggressiveness. Veterans sometimes don’t report these symptoms to health providers or realize they’re related to the trauma they experienced during combat.
The researchers also identified a correlation that indicates people with a higher level of education show a lower occurrence of the microbiotic signature linked to PTSD, while people who experienced greater exposure to air pollution show a higher occurrence of this signature. That confirms their finding that the veterans’ health is dependent on their individual biology combined with the conditions of their environment.
“Thanks to this study, it may be possible in the future to use objective molecular and biological characteristics to distinguish PTSD sufferers, taking into account environmental influences,” Gozes said in an article in Israel21c. “We hope that this new discovery and the microbial signatures described in this study might promote easier diagnosis of post-traumatic stress in soldiers so they can receive appropriate treatment.”
Gozes added that roughly a third of the subjects in their study hadn’t been diagnosed with PTSD previously. That meant they had never received any support from Israel’s Ministry of Defense or other officials for treatment and reparations, the payments to compensate for injuries sustained during war.
Shapira’s motivation to participate in this study is personal as well as professional: in addition to being veteran himself, his father served in the First Lebanon War. “Fortunately, he did not develop any PTSD, despite being shot in the foot...some of his friends died, so it wasn’t easy on him,” says Shapira.
“Having empirical metrics to assess whether or not someone has PTSD can help veterans who make their case to the Army to get reparations,” Shapira says. “It is a very difficult and demanding process, so the more empirical metrics we have to assess PTSD, the less people will have to suffer in these committees and unending examinations that are mostly pitched against the veterans because the state is trying to avoid spending too much money.”