

Hyperbaric oxygen therapy has been used in the past to help people with traumatic brain injury, stroke and other conditions involving wounds to the brain. Now, researchers at Shamir Medical Center in Tel Aviv are studying how it could treat Long Covid.
Long COVID is not a single disease, it is a syndrome or cluster of symptoms that can arise from exposure to SARS-CoV-2, a virus that affects an unusually large number of different tissue types. That's because the ACE2 receptor it uses to enter cells is common throughout the body, and inflammation from the immune response fighting that infection can damage surrounding tissue.
One of the most widely shared groups of symptoms is fatigue and what has come to be called “brain fog,” a difficulty focusing and an amorphous feeling of slowed mental functioning and capacity. Researchers have tied these COVID-related symptoms to tissue damage in specific sections of the brain and actual shrinkage in its size.
When Shai Efrati, medical director of the Sagol Center for Hyperbaric Medicine and Research in Tel Aviv, first looked at functional magnetic resonance images (fMRIs) of patients with what is now called long COVID, he saw “micro infarcts along the brain.” It reminded him of similar lesions in other conditions he had treated with hyperbaric oxygen therapy (HBOT). “Once we saw that, we said, this is the type of wound we can treat. It doesn't matter if the primary cause is mechanical injury like TBI [traumatic brain injury] or stroke … we know how to oxidize them.”Efrati came to HBOT almost by accident. The physician had seen how it had helped heal diabetic ulcers and improved the lives of other patients, but he was busy with his own research. Then the director of his Tel Aviv hospital threatened to shut down the small HBOT chamber unless Efrati took on administrative responsibility for it. He reluctantly agreed, a decision that shifted the entire focus of his research.
“The main difference between wounds in the leg and wounds in the brain is that one is something we can see, it's tangible, and the wound in the brain is hidden,” says Efrati. With fMRIs, he can measure how a limited supply of oxygen in blood is shuttled around to fuel activity in various parts of the brain. Years of research have mapped how specific areas of the brain control activity ranging from thinking to moving. An fMRI captures the brain area as it’s activated by supplies of oxygen; lack of activity after the same stimuli suggests damage has occurred in that tissue. Suddenly, what was hidden became visible to researchers using fMRI. It helped to make a diagnosis and measure response to treatment.
HBOT is not a single thing but rather a tool, a process or approach with variations depending on the condition being treated. It aims to increase the amount of oxygen that gets to damaged tissue and speed up healing. Regular air is about 21 percent oxygen. But inside the HBOT chamber the atmospheric pressure can be increased to up to three times normal pressure at sea level and the patient breathes pure oxygen through a mask; blood becomes saturated with much higher levels of oxygen. This can defuse through the damaged capillaries of a wound and promote healing.
The trial
Efrati’s clinical trials started in December 2020, barely a year after SARS-CoV-2 had first appeared in Israel. Patients who’d experienced cognitive issues after having COVID received 40 sessions in the chamber over a period of 60 days. In each session, they spent 90 minutes breathing through a mask at two atmospheres of pressure. While inside, they performed mental exercises to train the brain. The only difference between the two groups of patients was that one breathed pure oxygen while the other group breathed normal air. No one knew who was receiving which level of oxygen.
The results were striking. Before and after fMRIs showed significant repair of damaged tissue in the brain and functional cognition tests improved substantially among those who received pure oxygen. Importantly, 80 percent of patients said they felt back to “normal,” but Efrati says they didn't include patient evaluation in the paper because there was no baseline data to show how they functioned before COVID. After the study was completed, the placebo group was offered a new round of treatments using 100 percent oxygen, and the team saw similar results.
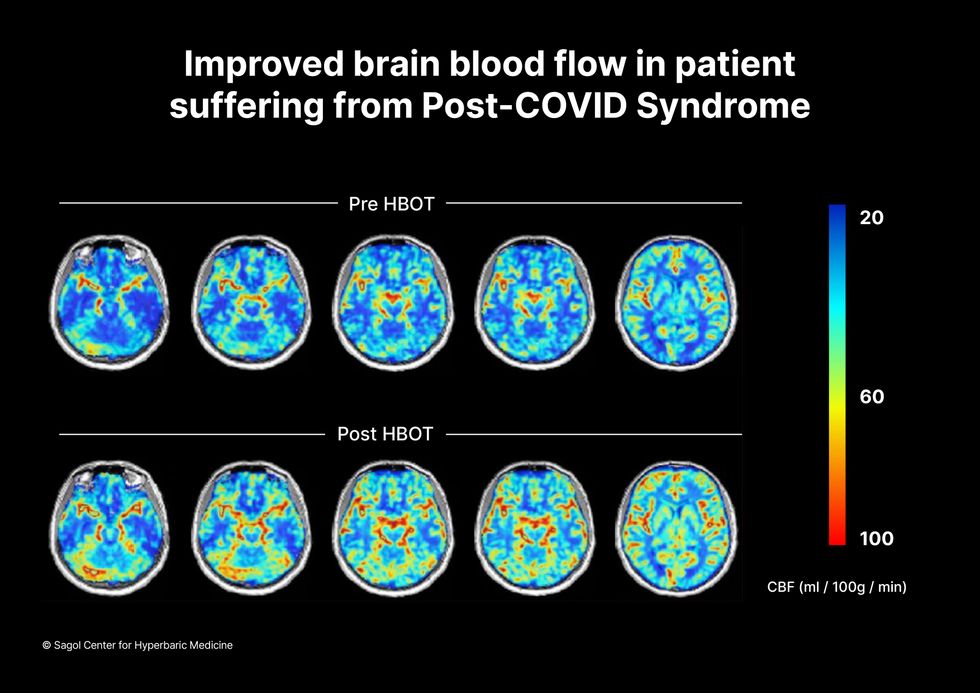
Scans show improved blood flow in a patient suffering from Long Covid.
Sagol Center for Hyperbaric Medicine
Efrati's use of HBOT is part of an emerging geroscience approach to diseases associated with aging. These researchers see systems dysfunctions that are common to several diseases, such as inflammation, which has been shown to play a role in micro infarcts, heart disease and Alzheimer’s disease. Preliminary research suggests that HBOT can retard some underlying mechanisms of aging, which might address several medical conditions. However, the drug approval process is set up to regulate individual disease, not conditions as broad as aging, and so they concentrate on treating the low hanging fruit: disorders where effective treatments currently are limited and success might be demonstrated.
The key to HBOT's effectiveness is something called the hyperoxic-hypoxic paradox where a body does not react to an increase in available oxygen, only to a decrease, regardless of the starting point. That danger signal has a powerful effect on gene expression, resulting in changes in metabolism, and the proliferation of stem cells. That occurs with each cycle of 20 minutes of pure oxygen followed by 5 minutes of regular air circulating through the masks, while the chamber remains pressurized. The high levels of oxygen in the blood provide the fuel necessary for tissue regeneration.
The hyperbaric chamber that Efrati has built can hold a dozen patients and attending medical staff. Think of it as a pressurized airplane cabin, only with much more space than even in first class. In the U.S., people think of HBOT as “a sack of air or some tube that you can buy on Amazon” or find at a health spa. “That is total bullshit,” Efrati says. “It has to be a medical class center where a physician can lose their license if they are not operating it properly.”

Shai Efrati
Alexander Charney, a research psychiatrist at the Icahn School of Medicine at Mount Sinai in New York City, calls Efrati’s study thoughtful and well designed. But it demands a lot from patients with its intense number of sessions. Those types of regimens have proven difficult to roll out to large numbers of patients. Still, the results are intriguing enough to merit additional trials.
John J. Miller, a physician and editor in chief of Psychiatric Times, has seen “many physicians that use hyperbaric oxygen for various brain disorders such as TBI.” He is intrigued by Efrati's work and believes the approach “has great potential to help patients with long COVID whose symptoms are related to brain tissue changes.”
Efrati believes so much in the power of the hyperoxic-hypoxic paradox to heal a variety of tissue injuries that he is leading the medical advisory board at Aviv Clinic, an international network of clinics that are delivering HBOT treatments based on research conducted in Israel. His goal is to silence doubters by quickly opening about 50 such clinics worldwide, based on the model of standalone dialysis clinics in the United States. Sagol Center is treating 300 patients per day, and clinics have opened in Florida and Dubai. There are plans to open another in Manhattan.

Rakhi Patel is among an increasing number of health care professionals, including doctors and nurses, who maintain an active persona on Instagram, TikTok and other social media sites.
“Health care professionals are quite prevalent on social media,” said Mercer Gary, a postdoctoral researcher at The Hastings Center, an independent bioethics research institute in Garrison, New York. “They’ve been posting on #medTwitter for many years, mainly to communicate with one another, but, of course, anyone can see the threads. Most recently, doctors and nurses have become a presence on TikTok.”
On social media, many health care providers perceive themselves to be “humanizing” their profession by coming across as more approachable — “reminding patients that providers are people and workers, as well as repositories of medical expertise,” Gary said. As a result, she noted that patients who are often intimidated by clinicians may feel comfortable enough to overcome barriers to scheduling health care appointments. The use of TikTok in particular may help doctors and nurses connect with younger followers.
When health care providers post on social media, they must bear in mind that they have legal and ethical duties to their patients, profession and society, said Elizabeth Levy, founder and director of Physicians for Justice.
While enduring three years of pandemic conditions, many health care professionals have struggled with burnout, exhaustion and moral distress. “Much health care provider content on social media seeks to expose the difficulties of the work,” Gary added. “TikTok and Instagram reels have shown health care providers crying after losing a patient or exhausted after a night shift in the emergency department.”
A study conducted in Beijing, China and published last year found that TikTok is the world’s most rapidly growing video application, amassing 1.6 billion users in 2021. “More and more patients are searching for information on genitourinary cancers via TikTok,” the study’s authors wrote in Frontiers in Oncology, referring to cancers of the urinary tracts and male reproductive organs. Among the 61 sample videos examined by the researchers, health care practitioners contributed the content in 29, or 47 percent, of them. Yet, 22 posts, 36 percent, were misinformative, mostly due to outdated information.
More than half of the videos offered good content on disease symptoms and examinations. The authors concluded that “most videos on genitourinary cancers on TikTok are of poor to medium quality and reliability. However, videos posted by media agencies enjoyed great public attention and interaction. Medical practitioners could improve the video quality by cooperating with media agencies and avoiding unexplained terminologies.”
When health care providers post on social media, they must bear in mind that they have legal and ethical duties to their patients, profession and society, said Elizabeth Levy, founder and director of Physicians for Justice in Irvine, Calif., a nonprofit network of volunteer physicians partnering with public interest lawyers to address the social determinants of health.
“Providers are also responsible for understanding the mechanics of their posts,” such as who can see these messages and how long they stay up, Levy said. As a starting point for figuring what’s acceptable, providers could look at social media guidelines put out by their professional associations. Even beyond that, though, they must exercise prudent judgment. “As social media continues to evolve, providers will also need to stay updated with the changing risks and benefits of participation.”
Patients often research their providers online, so finding them on social media can help inform about values and approaches to care, said M. Sara Rosenthal, a professor and founding director of the program for bioethics and chair of the hospital ethics committee at the University of Kentucky College of Medicine.
Health care providers’ posts on social media also could promote patient education. They can advance informed consent and help patients navigate the risks and benefits of various treatments or preventive options. However, providers could violate ethical principles if they espouse “harmful, risky or questionable therapies or medical advice that is contrary to clinical practice guidelines or accepted standards of care,” Rosenthal said.
Inappropriate self-disclosure also can affect a provider’s reputation, said Kelly Michelson, a professor of pediatrics and director of the Center for Bioethics and Medical Humanities at Northwestern University’s Feinberg School of Medicine. A clinician’s obligations to professionalism extend beyond those moments when they are directly taking care of their patients, she said. “Many experts recommend against clinicians ‘friending’ patients or the families on social media because it blurs the patient-clinician boundary.”
Meanwhile, clinicians need to adhere closely to confidentiality. In sharing a patient’s case online for educational purposes, safeguarding identity becomes paramount. Removing names and changing minor details is insufficient, Michelson said.
“The patient-clinician relationship is sacred, and it can only be effective if patients have 100 percent confidence that all that happens with their clinician is kept in the strictest of confidence,” she said, adding that health care providers also should avoid obtaining information about their patients from social media because it can lead to bias and risk jeopardizing objectivity.
Academic clinicians can use social media as a recruitment tool to expand the pool of research participants for their studies, Michelson said. Because the majority of clinical research is conducted at academic medical centers, large segments of the population are excluded. “This affects the quality of the data and knowledge we gain from research,” she said.
Don S. Dizon, a professor of medicine and surgery at the Warren Alpert Medical School of Brown University in Providence, Rhode Island, uses LinkedIn and Doximity, as well as Twitter, Instagram, TikTok, Facebook, and most recently, YouTube and Post. He’s on Twitter nearly every day, where he interacts with the oncology community and his medical colleagues.
Also, he said, “I really like Instagram. It’s where you will see a hybrid of who I am professionally and personally. I’ve become comfortable sharing both up to a limit, but where else can I combine my appreciation of clothes with my professional life?” On that site, he’s seen sporting shirts with polka dots or stripes and an occasional bow-tie. He also posts photos of his cats.

Don S. Dizon, a professor of medicine and surgery at Brown, started using TikTok several years ago, telling medical stories in short-form videos.
Don S. Dizon
Dizon started using TikTok several years ago, telling medical stories in short-form videos. He may talk about an inspirational patient, his views on end-of-life care and death, or memories of people who have passed. But he is careful not to divulge any details that would identify anyone.
Recently, some people have become his patients after viewing his content on social media or on the Internet in general, which he clearly states isn’t a forum for medical advice. “In both situations, they are so much more relaxed when we meet, because it’s as if they have a sense of who I am as a person,” Dizon said. “I think that has helped so much in talking through a cancer diagnosis and a treatment plan, and yes, even discussions about prognosis.”
He also posts about equity and diversity. “I have found myself more likely to repost or react to issues that are inherently political, including racism, homophobia, transphobia and lack-of-access issues, because medicine is not isolated from society, and I truly believe that medicine is a social justice issue,” said Dizon, who is vice chair of diversity, equity, inclusion and professional integrity at the SWOG Cancer Research Network.
Through it all, Dizon likes “to break through the notion of doctor as infallible and all-knowing, the doctor as deity,” he said. “Humanizing what I do, especially in oncology, is something that challenges me on social media, and I appreciate the opportunities to do it on TikTok.”

Previous research showed that restricting calories results in longer lives for mice, worms and flies. A new study by Columbia University researchers applied those findings to people. But what does this paper actually show?
Evan Hadley, Director of the Division of Geriatrics and Clinical Gerontology at the National Institute of Aging
NIA