
Why Neglected Tropical Diseases Should Matter to Americans

Kissing bugs can carry a parasite called Trypanosoma cruzi, which causes Chagas disease.
Daisy Hernández was five years old when one of her favorite aunts was struck with a mysterious illness. Tía Dora had stayed behind in Colombia when Daisy's mother immigrated to Union City, New Jersey. A schoolteacher in her late 20s, she began suffering from fevers and abdominal pain, and her belly grew so big that people thought she was pregnant. Exploratory surgery revealed that her large intestine had swollen to ten times its normal size, and she was fitted with a colostomy bag. Doctors couldn't identify the underlying problem—but whatever it was, they said, it would likely kill her within a year or two.
Tía Dora's sisters in New Jersey—Hernández's mother and two other aunts—weren't about to let that happen. They pooled their savings and flew her to New York City, where a doctor at Columbia-Presbyterian Medical Center with a penchant for obscure ailments provided a diagnosis: Chagas disease. Transmitted by the bite of triatomine insects, commonly known as kissing bugs, Chagas is endemic in many parts of Latin America. It's caused by the parasite Trypanoma cruzi, which usually settles in the heart, where it feeds on muscle tissue. In some cases, however, it attacks the intestines or esophagus. Tía Dora belonged to that minority.
In 1980, U.S. immigration laws were more forgiving than they are today. Tía Dora was able to have surgery to remove a part of her colon, despite not being a citizen or having a green card. She eventually married a legal resident and began teaching Spanish at an elementary school. Over the next three decades, she earned a graduate degree, built a career, and was widowed. Meanwhile, Chagas continued its slow devastation. "Every couple of years, we were back in the hospital with her," Hernández recalls. "When I was in high school, she started feeling like she couldn't swallow anything. It was the parasite, destroying the muscles of her esophagus."
When Tía Dora died in 2010, at 59, her niece was among the family members at her bedside. By then, Hernández had become a journalist and fiction writer. Researching a short story about Chagas disease, she discovered that it affected an estimated 6 million people in South America, Central America, and Mexico—as well as 300,000 in the United States, most of whom were immigrants from those places. "I was shocked to learn it wasn't rare," she says. "That made me hungry to know more about this disease, and about the families grappling with it."
Hernández's curiosity led her to write The Kissing Bug, a lyrical hybrid of memoir and science reporting that was published in June. It also led her to another revelation: Chagas is not unique. It's among the many maladies that global health experts refer to as neglected tropical diseases—often-disabling illnesses that afflict 1.7 billion people worldwide, while getting notably less attention than the "big three" of HIV/AIDs, malaria, and tuberculosis. NTDs cause fewer deaths than those plagues, but they wreak untold suffering and economic loss.
Shortly before Hernández's book hit the shelves, the World Health Organization released its 2021-2030 roadmap for fighting NTDs. The plan sets targets for controlling, eliminating, or eradicating all the diseases on the WHO's list, through measures ranging from developing vaccines to improving healthcare infrastructure, sanitation, and access to clean water. Experts agree that for the campaign to succeed, leadership from wealthy nations—particularly the United States—is essential. But given the inward turn of many such countries in recent years (evidenced in movements ranging from America First to Brexit), and the continuing urgency of the COVID-19 crisis, public support is far from guaranteed.
As Hernández writes: "It is easier to forget a disease that cannot be seen." NTDs primarily affect residents of distant lands. They kill only 80,000 people a year, down from 204,000 in 1990. So why should Americans to bother to look?
Breaking the circle of poverty and disease
The World Health Organization counts 20 diseases as NTDs. Along with Chagas, they include dengue and chikungunya, which cause high fevers and agonizing pain; elephantiasis, which deforms victims' limbs and genitals; onchocerciasis, which causes blindness; schistosomiasis, which can damage the heart, lungs, brain, and genitourinary system; helminths such as roundworm and whipworm, which cause anemia, stunted growth, and cognitive disabilities; and a dozen more. Such ailments often co-occur in the same patient, exacerbating each other's effects and those of illnesses such as malaria.
NTDs may be spread by insects, animals, soil, or tainted water; they may be parasitic, bacterial, viral, or—in the case of snakebite envenoming—non-infectious. What they have in common is their longtime neglect by public health agencies and philanthropies. In part, this reflects their typically low mortality rates. But the biggest factor is undoubtedly their disempowered patient populations.
"These diseases occur in the setting of poverty, and they cause poverty, because of their chronic and debilitating effects," observes Peter Hotez, dean of the National School of Tropical Medicine at Baylor University and co-director of the Texas Children's Hospital for Vaccine Development. And historically, the everyday miseries of impoverished people have seldom been a priority for those who set the global health agenda.
That began to change about 20 years ago, when Hotez and others developed the conceptual framework for NTDs and early proposals for combating them. The WHO released its first roadmap in 2012, targeting 17 NTDs for control, elimination, or eradication by 2020. (Rabies, snakebite, and dengue were added later.) Since then, the number of people at risk for NTDs has fallen by 600 million, and 42 countries have eliminated at least one such disease. Cases of dracunculiasis—known as Guinea worm disease, for the parasite that creates painful blisters in a patient's skin—have dropped from the millions to just 27 in 2020.
Yet the battle is not over, and the COVID-19 pandemic has disrupted prevention and treatment programs around the globe.
A new direction — and longstanding obstacles
The WHO's new roadmap sets even more ambitious goals for 2030. Among them: reducing by 90 percent the number of people requiring treatment for NTDs; eliminating at least one NTD in another 100 countries; and fully eradicating dracunculiasis and yaws, a disfiguring skin infection.
The plan also places an increased focus on "country ownership," relying on nations with high incidence of NTDs to design their own plans based on local expertise. "I was so excited to see that," says Kristina Talbert-Slagle, director of the Yale College Global Health Studies program. "No one is a better expert on how to address these situations than the people who deal with it day by day."
Another fresh approach is what the roadmap calls "cross-cutting" targets. "One of the really cool things about the plan is how much it emphasizes coordination among different sectors of the health system," says Claire Standley, a faculty member at Georgetown University's Center for Global Health Science and Security. "For example, it explicitly takes into account the zoonotic nature of many neglected tropical diseases—the fact that we have to think about animal health as well as human health when we tackle NTDs."
Whether this grand vision can be realized, however, will depend largely on funding—and that, in turn, is a question of political will in the countries most able to provide it. On the upside, the U.S. has ended its Trump-era feud with the WHO. "One thing that's been really encouraging," says Standley, "has been the strong commitment toward global cooperation from the current administration." Even under the previous president, the U.S. remained the single largest contributor to the global health kitty, spending over $100 million annually on NTDs—six times the figure in 2006, when such financing started.
On the downside, America's outlay has remained flat for several years, and the Biden administration has so far not moved to increase it. A "back-of-the-envelope calculation," says Hotez, suggests that the current level of aid could buy medications for the most common NTDs for about 200 million people a year. But the number of people who need treatment, he notes, is at least 750 million.
Up to now, the United Kingdom—long the world's second-most generous health aid donor—has taken up a large portion of the slack. But the UK last month announced deep cuts in its portfolio, eliminating 102 previously supported countries and leaving only 34. "That really concerns me," Hotez says.
The struggle for funds, he notes, is always harder for projects involving NTDs than for those aimed at higher-profile diseases. His lab, which he co-directs with microbiologist Maria Elena Bottazzi, started developing a COVID-19 vaccine soon after the pandemic struck, for example, and is now in Phase 3 trials. The team has been working on vaccines for Chagas, hookworm, and schistosomiasis for much longer, but trials for those potential game-changers lag behind. "We struggle to get the level of resources needed to move quickly," Hotez explains.
Two million reasons to care
One way to prompt a government to open its pocketbook is for voters to clamor for action. A longtime challenge with NTDs, however, has been getting people outside the hardest-hit countries to pay attention.
The reasons to care, global health experts argue, go beyond compassion. "When we have high NTD burden," says Talbert-Slagle, "it can prevent economic growth, prevent innovation, lead to more political instability." That, in turn, can lead to wars and mass migration, affecting economic and political events far beyond an affected country's borders.
Like Hernández's aunt Dora, many people driven out of NTD-wracked regions wind up living elsewhere. And that points to another reason to care about these diseases: Some of your neighbors might have them. In the U.S., up to 14 million people suffer from neglected parasitic infections—including 70,000 with Chagas in California alone.
When Hernández was researching The Kissing Bug, she worried that such statistics would provide ammunition to racists and xenophobes who claim that immigrants "bring disease" or exploit overburdened healthcare systems. (This may help explain some of the stigma around NTDs, which led Tía Dora to hide her condition from most people outside her family.) But as the book makes clear, these infections know no borders; they flourish wherever large numbers of people lack access to resources that most residents of rich countries take for granted.
Indeed, far from gaming U.S. healthcare systems, millions of low-income immigrants can't access them—or must wait until they're sick enough to go to an emergency room. Since Congress changed the rules in 1996, green card holders have to wait five years before they can enroll in Medicaid. Undocumented immigrants can never qualify.
Closing the great divide
Hernández uses a phrase borrowed from global health crusader Paul Farmer to describe this access gap: "the great epi divide." On one side, she explains, "people will die from cancer, from diabetes, from chronic illnesses later in life. On the other side of the epidemiological divide, people are dying because they can't get to the doctor, or they can't get medication. They don't have a hospital anywhere near them. When I read Dr. Farmer's work, I realized how much that applied to neglected diseases as well."
When it comes to Chagas disease, she says, the epi divide is embodied in the lack of a federal mandate for prenatal or newborn screening. Each year, according to the Centers for Disease Control and Prevention, up to 300 babies in the U.S. are born with Chagas, which can be passed from the mother in utero. The disease can be cured with medication if treated in infancy. (It can also be cured in adults in the acute stage, but is seldom detected in time.) Yet the CDC does not require screening for Chagas—even though newborns are tested for 15 diseases that are less common. According to one study, it would be 10 times cheaper to screen and treat babies and their mothers than to cover the costs related to the illness in later years. Few states make the effort.
The gap that enables NTDs to persist, Hernández argues, is the same one that has led to COVID-19 death rates in Black and Latinx communities that are double those elsewhere in America. To close it, she suggests, caring is not enough.
"When I was working on my book," she says, "I thought about HIV in the '80s, when it had so much stigma that no one wanted to talk about it. Then activists stepped up and changed the conversation. I thought a lot about breast cancer, which was stigmatized for years, until people stepped forward and started speaking out. I thought about Lyme disease. And it wasn't only patients—it was also allies, right? The same thing needs to happen with neglected diseases around the world. Allies need to step up and make demands on policymakers. We need to make some noise."

The CRISPR-Cas9 gene editing tool could be used to "turn off" pain directly, raising ethical questions for society.
Scientists have long been aware that some people live with what's known as "congenital insensitivity to pain"—the inability to register the tingles, jolts, and aches that alert most people to injury or illness.
"If you break the chain of transmission somewhere along there, it doesn't matter what the message is—the recipient will not get it."
On the ospposite end of the spectrum, others suffer from hyperalgesia, or extreme pain; for those with erythromelalgia, also known as "Man on Fire Syndrome," warm temperatures can feel like searing heat—even wearing socks and shoes can make walking unbearable.
Strangely enough, the two conditions can be traced to mutations in the same gene, SCN9A. It produces a protein that exists in spinal cells—specifically, in the dorsal root ganglion—which transmits the sensation of pain from the nerves at the peripheral site of an injury into the central nervous system and to the brain. This fact may become the key to pain relief for the roughly 20 percent of Americans who suffer from chronic pain, and countless other patients around the world.
"If you break the chain of transmission somewhere along there, it doesn't matter what the message is—the recipient will not get it," said Dr. Fyodor Urnov, director of the Innovative Genomics Institute and a professor of molecular and cell biology at the University of California, Berkeley. "For scientists and clinicians who study this, [there's] this consistent tracking of: You break this gene, you stop feeling pain; make this gene hyperactive, you feel lots of pain—that really cuts through the correlation versus causation question."
Researchers tried for years, without much success, to find a chemical that would block that protein from working and therefore mute the pain sensation. The CRISPR-Cas9 gene editing tool could completely sidestep that approach and "turn off" pain directly.
Yet as CRISPR makes such targeted therapies increasingly possible, the ethical questions surrounding gene editing have taken on a new and more urgent cast—particularly in light of the work of the disgraced Chinese scientist He Jiankui, who announced in late 2018 that he had created the world's first genetically edited babies. He used CRISPR to edit two embryos, with the goal of disabling a gene that makes people susceptible to HIV infection; but then took the unprecedented step of implanting the edited embryos for pregnancy and birth.
Edits to germline cells, like the ones He undertook, involve alterations to gametes or embryos and carry much higher risk than somatic cell edits, since changes will be passed on to any future generations. There are also concerns that imprecise edits could result in mutations and end up causing more disorders. Recent developments, particularly the "search-and replace" prime-editing technique published last fall, will help minimize those accidental edits, but the fact remains that we have little understanding of the long-term effects of these germline edits—for the future of the patients themselves, or for the broader gene pool.
"We need to have appropriate venues where we deliberate and consider the ethical, legal and social implications of gene editing as a society."
It is much harder to predict the effects, harmful or otherwise, on the larger human population as a result of interactions with the environment or other genetic variations; with somatic cell edits, on the other hand— like the ones that would be made in an individual to turn off pain—only the person receiving the treatment is affected.
Beyond the somatic/germline distinction, there is also a larger ethical question over how much genetic interference society is willing to tolerate, which may be couched as the difference between therapeutic editing—interventions in response to a demonstrated medical need—and "enhancement" editing. The Chinese scientist He was roundly criticized in the scientific community for the fact that there are already much safer and more proven methods of preventing the parent-to-child transmission of HIV through the IVF process, making his genetic edits medically unnecessary. (The edits may also have increased the girls' risk of susceptibility to other viruses, like influenza and the West Nile virus.)
Yet there are even more extreme goals that CRISPR could be used to reach, ones further removed from any sort of medical treatment. The 1997 science fiction movie Gattaca imagined a dystopian future where genetic selection for strength and intelligence is common, creating a society that explicitly and unapologetically endorses eugenics. In the real world, Russian President Vladimir Putin has commented that genetic editing could be used to create "a genius mathematician, a brilliant musician or a soldier, a man who can fight without fear, compassion, regret or pain."
"[Such uses] would be considered using gene editing for 'enhancement,'" said Dr. Zubin Master, an associate professor of biomedical ethics at the Mayo Clinic, who noted that a series of studies have strongly suggested that members of the public, in the U.S. and around the world, are much less amenable to the prospect of gene editing for these purposes than for the treatment of illness and disease.
Putin's comments were made in 2017, before news of He's experiment broke; since then no country has moved to continue experiments on germline editing (although one Russian IVF specialist, Denis Rebrikov, appears ready to do so, if given approval). Master noted that the World Health Organization has an 18-person committee currently dedicated to considering these questions. The Expert Advisory Committee on Developing Global Standards for Governance and Oversight of Human Genome Editing first convened in March 2019; that July, it issued a recommendation to regulatory and ethics authorities in all countries to refrain from approving clinical application requests for work on human germline genome editing—the kind of alterations to genetic cells used by He. The committee's report and a fleshed-out set of guidelines is expected after its final meeting, in Geneva this September (unless the COVID-19 pandemic disrupts the timeline).
Regardless of the WHO's report, in the U.S., all regulations of new medical procedures are overseen at the federal level, subjected to extensive regulatory review by the FDA; the chance of any doctor or company going rogue is minimal to none. Likewise, the challenges we face are more on the regulatory end of the spectrum than the Gattaca end. Dr. Stephanie Malia Fullerton, a bioethics professor at the University of Washington, pointed out that eugenics not only typically involves state-sponsored control of reproduction, but requires a much more clearly delineated genetic basis of common complex traits—indeed, SCN9A is one way to get to pain, but is not the only source—and suggested that current concerns about over-prescribing opioids are a more pressing question for society to address.
In fact, Navega Therapeutics, based in San Diego, hopes to find out whether the intersection of this research into SCN9A and CRISPR would be an effective way to address the U.S. opioid crisis. Currently in a preclinical funding stage, Navega's approach focuses on editing epigenetic molecules attached to the basic DNA strand—the idea is that the gene's expression can be activated or suppressed rather than removed entirely, reducing the risk of unwanted side effects from permanently altering the genetic code.
As these studies focused on the sensation of pain go forward, what we are likely to see simultaneously is the use of CRISPR to target diseases that are the root causes of that pain. Last summer, Victoria Gray, a Mississippi woman with sickle cell disease was the second-ever person to be treated with CRISPR therapy in the U.S. The disease is caused by a genetic mutation that creates malformed blood cells, which can't carry oxygen as normal and get stuck inside blood vessels, causing debilitating pain. For the study, conducted in concert with CRISPR Therapeutics, of Cambridge, Mass., cells were removed from Gray's bone marrow, modified using CRISPR, and infused back into her body, a technique called ex vivo editing.
In early February this year, researchers at the University of Pennsylvania published a study on a first-in-human phase 1 clinical trial, in which three patients with advanced cancer received an infusion of ex vivo engineered T cells in an effort to improve antitumor immunity. The modified cells persisted for up to nine months, and the patients experienced no serious adverse side effects, suggesting that this sort of therapeutic gene editing can be performed safely and could potentially allow patients to avoid the excruciating process of chemotherapy.
Then, just this spring, researchers made another advance: The first attempt at in vivo CRISPR editing—where the edits happen inside the patient's body—is currently underway, as doctors attempt to treat a patient blinded by Leber congenital amaurosis, a rare genetic disorder. In an Oregon study sponsored by Editas Medicine and Allergan, the patient, a volunteer, was injected with a harmless virus carrying CRISPR gene-editing machinery; the hope is that the tool will be able to edit out the genetic defect and restore production of a crucial protein. Based on preliminary safety reports, the study has been cleared to continue, and data on higher doses may be available by the end of 2020. Editas Medicine and CRISPR Therapeutics are joined in this sphere by Intellia Therapeutics, which is seeking approval for a trial later this year on amyloidosis, a rare liver condition.
For any such treatment targeting SCN9A to make its way to human subjects, it would first need to undergo years' worth of testing—on mice, on primates, and then on volunteer patients after an extended informed-consent process. If everything went perfectly, Urnov estimates it could take at least three to four years end to end and cost between $5 and 10 million—but that "if" is huge.
"The idea of a regular human being, genetically pure of pain?"
And as that happens, "we need to have appropriate venues where we deliberate and consider the ethical, legal and social implications of gene editing as a society," Master said. CRISPR itself is open-source, but its application is subject to the approval of governments, institutions, and societies, which will need to figure out where to draw the line between miracle treatments and playing God. Something as unpleasant and ubiquitous as pain may in fact be the most appropriate place to start.
"The pain circuit is very old," Urnov said. "We have evolved with the senses that we have, and have become the species that we are, as a result of who we are, physiologically. Yes, I take Advil—but when I get a headache! The idea of a regular human being, genetically pure of pain?... The permanent disabling or turning down of the pain sensation, for anything other than a medical reason? … That seems to be challenging Mother Nature in the wrong ways."
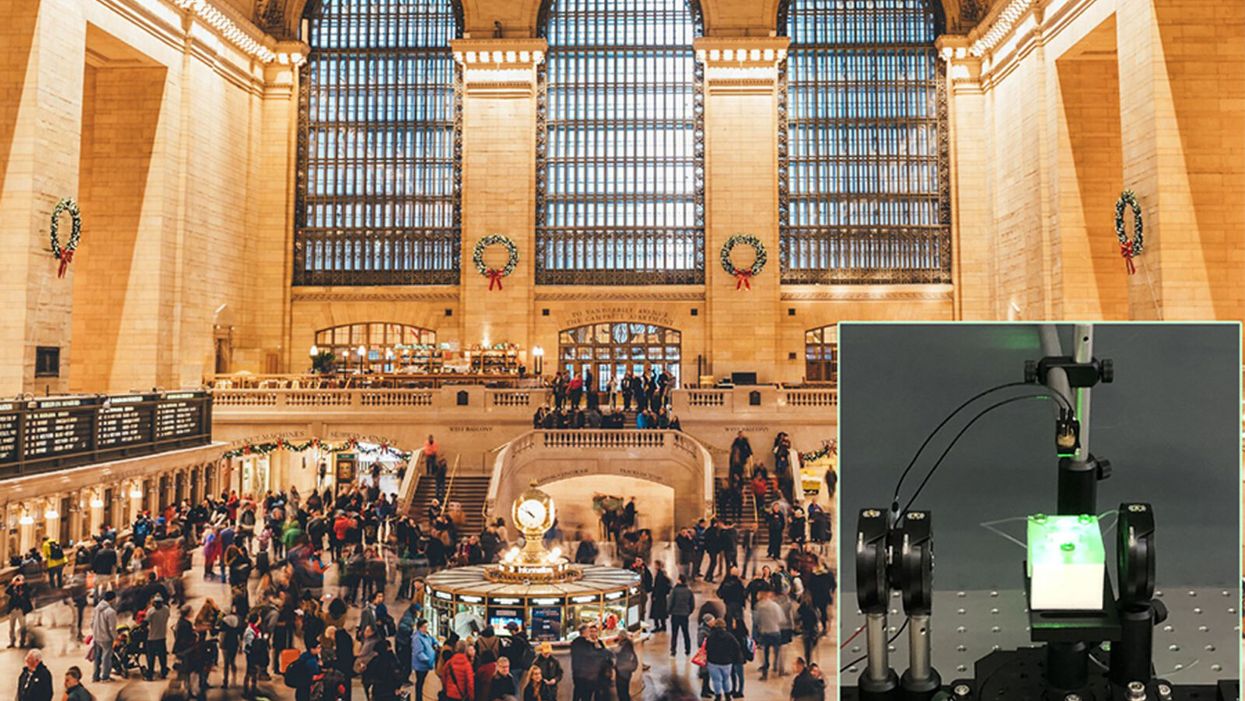
A biosensor in development (inset) could potentially be used to detect novel viruses in transit hubs like Grand Central Station in New York City.
The unprecedented scale and impact of the COVID-19 pandemic has caused scientists and engineers around the world to stop whatever they were working on and shift their research toward understanding a novel virus instead.
"We have confidence that we can use our system in the next pandemic."
For Guangyu Qiu, normally an environmental engineer at the Swiss Federal Laboratories for Materials Science and Technology, that means finding a clever way to take his work on detecting pollution in the air and apply it to living pathogens instead. He's developing a new type of biosensor to make disease diagnostics and detection faster and more accurate than what's currently available.
But even though this pandemic was the impetus for designing a new biosensor, Qiu actually has his eye on future disease outbreaks. He admits that it's unlikely his device will play a role in quelling this virus, but says researchers already need to be thinking about how to make better tools to fight the next one — because there will be a next one.
"In the last 20 years, there [have been] three different coronavirus [outbreaks] ... so we have to prepare for the coming one," Qiu says. "We have confidence that we can use our system in the next pandemic."
"A Really, Really Neat Idea"
His main concern is the diagnostic tool that's currently front and center for testing patients for SARS-Cov-2, the virus causing the novel coronavirus disease. The tool, called PCR (short for reverse transcription polymerase chain reaction), is the gold standard because it excels at detecting viruses in even very small samples of mucus. PCR can amplify genetic material in the limited sample and look for a genetic code matching the virus in question. But in many parts of the world, mucus samples have to be sent out to laboratories for that work, and results can take days to return. PCR is also notoriously prone to false positives and negatives.
"I read a lot of newspapers that report[ed] ... a lot of false negative or false positive results at the very beginning of the outbreak," Qiu says. "It's not good for protecting people to prevent further transmission of the disease."
So he set out to build a more sensitive device—one that's less likely to give you a false result. Qiu's biosensor relies on an idea similar to the dual-factor authentication required of anyone trying to access a secure webpage. Instead of verifying that a virus is really present by using one way of detecting genetic code, as with PCR, this biosensor asks for two forms of ID.
SARS-CoV-2 is what's called an RNA virus, which means it has a single strand of genetic code, unlike double-stranded DNA. Inside Qiu's biosensor are receptors with the complementary code for this particular virus' RNA; if the virus is present, its RNA will bind with the receptors, locking together like velcro. The biosensor also contains a prism and a laser that work together to verify that this RNA really belongs to SARS-CoV-2 by looking for a specific wavelength of light and temperature.
If the biosensor doesn't detect either, or only registers a match for one and not the other, then it can't produce a positive result. This multi-step authentication process helps make sure that the RNA binding with the receptors isn't a genetically similar coronavirus like SARS-CoV, known for its 2003 outbreak, or MERS-CoV, which caused an epidemic in 2012.
It could also be fitted to detect future novel viruses once their genomes are sequenced.
The dual-feature design of this biosensor "is a really, really neat idea that I have not seen before with other sensor technology," says Erin Bromage, a professor of infection and immunology at the University of Massachusetts Dartmouth; he was not involved in designing or testing Qiu's biosensor. "It makes you feel more secure that when you have a positive, you've really got a positive."
The light and temperature sensors are not in themselves new inventions, but the combination is a first. The part of the device that uses light to detect particles is actually central to Qiu's normal stream of environmental research, and is a versatile tool he's been working with for a long time to detect aerosols in the atmosphere and heavy metals in drinking water.
Bromage says this is a plus. "It's not high-risk in the sense that how they do this is unique, or not validated. They've taken aspects of really proven technology and sort of combined it together."
This new biosensor is still a prototype that will take at least another 12 months to validate in real world scenarios, though. The device is sound from a biological perspective and is sensitive enough to reliably detect SARS-CoV-2 — and to not be tricked by genetically similar viruses like SARS-CoV — but there is still a lot of engineering work that needs to be done in order for it to work outside the lab. Qiu says it's unlikely that the sensor will help minimize the impact of this pandemic, but the RNA receptors, prism, and laser inside the device can be customized to detect other viruses that may crop up in the future.
"If we choose another sequence—like SARS, like MERS, or like normal seasonal flu—we can detect other viruses, or even bacteria," Qiu says. "This device is very flexible."
It could also be fitted to detect future novel viruses once their genomes are sequenced.
The Long-Term Vision: Hospitals and Transit Hubs
The device has been designed to connect with two other systems: an air sampler and a microprocessor because the goal is to make it portable, and able to pick up samples from the air in hospitals or public areas like train stations or airports. A virus could hopefully be detected before it silently spreads and erupts into another global pandemic. In the case of SARS-CoV-2, there has been conflicting research about whether or not the virus is truly airborne (though it can be spread by droplets that briefly move through the air after a cough or sneeze), whereas the highly contagious RNA virus that causes measles can remain in the air for up to two hours.
"They've got a lot on the front end to work out," Bromage says. "They've got to work out how to capture and concentrate a virus, extract the RNA from the virus, and then get it onto the sensor. That's some pretty big hurdles, and may take some engineering that doesn't exist right now. But, if they can do that, then that works out really quite well."
One of the major obstacles in containing the COVID-19 pandemic has been in deploying accurate, quick tools that can be used for early detection of a virus outbreak and for later tracing its spread. That will still be true the next time a novel virus rears its head, and it's why Qiu feels that even if his biosensor can't help just yet, the research is still worth the effort.
It could also be fitted to detect future novel viruses once their genomes are sequenced.
The dual-feature design of this biosensor "is a really, really neat idea that I have not seen before with other sensor technology," says Erin Bromage, a professor of infection and immunology at the University of Massachusetts Dartmouth; he was not involved in designing or testing Qiu's biosensor. "It makes you feel more secure that when you have a positive, you've really got a positive."
The light and temperature sensors are not in themselves new inventions, but the combination is a first. The part of the device that uses light to detect particles is actually central to Qiu's normal stream of environmental research, and is a versatile tool he's been working with for a long time to detect aerosols in the atmosphere and heavy metals in drinking water.
Bromage says this is a plus. "It's not high-risk in the sense that how they do this is unique, or not validated. They've taken aspects of really proven technology and sort of combined it together."
This new biosensor is still a prototype that will take at least another 12 months to validate in real world scenarios, though. The device is sound from a biological perspective and is sensitive enough to reliably detect SARS-CoV-2 — and to not be tricked by genetically similar viruses like SARS-CoV — but there is still a lot of engineering work that needs to be done in order for it to work outside the lab. Qiu says it's unlikely that the sensor will help minimize the impact of this pandemic, but the RNA receptors, prism, and laser inside the device can be customized to detect other viruses that may crop up in the future.
"If we choose another sequence—like SARS, like MERS, or like normal seasonal flu—we can detect other viruses, or even bacteria," Qiu says. "This device is very flexible."
It could also be fitted to detect future novel viruses once their genomes are sequenced.
The Long-Term Vision: Hospitals and Transit Hubs
The device has been designed to connect with two other systems: an air sampler and a microprocessor because the goal is to make it portable, and able to pick up samples from the air in hospitals or public areas like train stations or airports. A virus could hopefully be detected before it silently spreads and erupts into another global pandemic. In the case of SARS-CoV-2, there has been conflicting research about whether or not the virus is truly airborne (though it can be spread by droplets that briefly move through the air after a cough or sneeze), whereas the highly contagious RNA virus that causes measles can remain in the air for up to two hours.
"They've got a lot on the front end to work out," Bromage says. "They've got to work out how to capture and concentrate a virus, extract the RNA from the virus, and then get it onto the sensor. That's some pretty big hurdles, and may take some engineering that doesn't exist right now. But, if they can do that, then that works out really quite well."
One of the major obstacles in containing the COVID-19 pandemic has been in deploying accurate, quick tools that can be used for early detection of a virus outbreak and for later tracing its spread. That will still be true the next time a novel virus rears its head, and it's why Qiu feels that even if his biosensor can't help just yet, the research is still worth the effort.