

The Cocoanut Grove fire in Boston in 1942 tragically claimed 490 lives, but was the catalyst for several important medical advances.
On the evening of November 28, 1942, more than 1,000 revelers from the Boston College-Holy Cross football game jammed into the Cocoanut Grove, Boston's oldest nightclub. When a spark from faulty wiring accidently ignited an artificial palm tree, the packed nightspot, which was only designed to accommodate about 500 people, was quickly engulfed in flames. In the ensuing panic, hundreds of people were trapped inside, with most exit doors locked. Bodies piled up by the only open entrance, jamming the exits, and 490 people ultimately died in the worst fire in the country in forty years.
"People couldn't get out," says Dr. Kenneth Marshall, a retired plastic surgeon in Boston and president of the Cocoanut Grove Memorial Committee. "It was a tragedy of mammoth proportions."
Within a half an hour of the start of the blaze, the Red Cross mobilized more than five hundred volunteers in what one newspaper called a "Rehearsal for Possible Blitz." The mayor of Boston imposed martial law. More than 300 victims—many of whom subsequently died--were taken to Boston City Hospital in one hour, averaging one victim every eleven seconds, while Massachusetts General Hospital admitted 114 victims in two hours. In the hospitals, 220 victims clung precariously to life, in agonizing pain from massive burns, their bodies ravaged by infection.
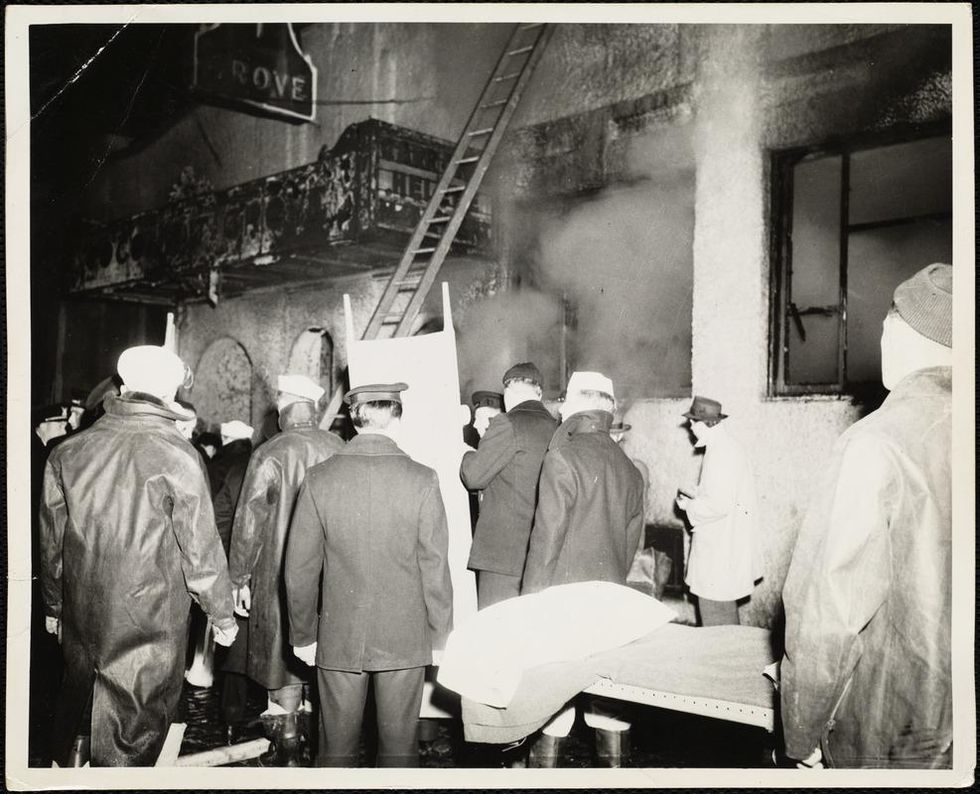
The scene of the fire.
Boston Public Library
Tragic Losses Prompted Revolutionary Leaps
But there is a silver lining: this horrific disaster prompted dramatic changes in safety regulations to prevent another catastrophe of this magnitude and led to the development of medical techniques that eventually saved millions of lives. It transformed burn care treatment and the use of plasma on burn victims, but most importantly, it introduced to the public a new wonder drug that revolutionized medicine, midwifed the birth of the modern pharmaceutical industry, and nearly doubled life expectancy, from 48 years at the turn of the 20th century to 78 years in the post-World War II years.
The devastating grief of the survivors also led to the first published study of post-traumatic stress disorder by pioneering psychiatrist Alexandra Adler, daughter of famed Viennese psychoanalyst Alfred Adler, who was a student of Freud. Dr. Adler studied the anxiety and depression that followed this catastrophe, according to the New York Times, and "later applied her findings to the treatment World War II veterans."
Dr. Ken Marshall is intimately familiar with the lingering psychological trauma of enduring such a disaster. His mother, an Irish immigrant and a nurse in the surgical wards at Boston City Hospital, was on duty that cold Thanksgiving weekend night, and didn't come home for four days. "For years afterward, she'd wake up screaming in the middle of the night," recalls Dr. Marshall, who was four years old at the time. "Seeing all those bodies lined up in neat rows across the City Hospital's parking lot, still in their evening clothes. It was always on her mind and memories of the horrors plagued her for the rest of her life."
The sheer magnitude of casualties prompted overwhelmed physicians to try experimental new procedures that were later successfully used to treat thousands of battlefield casualties. Instead of cutting off blisters and using dyes and tannic acid to treat burned tissues, which can harden the skin, they applied gauze coated with petroleum jelly. Doctors also refined the formula for using plasma--the fluid portion of blood and a medical technology that was just four years old--to replenish bodily liquids that evaporated because of the loss of the protective covering of skin.
"Every war has given us a new medical advance. And penicillin was the great scientific advance of World War II."
"The initial insult with burns is a loss of fluids and patients can die of shock," says Dr. Ken Marshall. "The scientific progress that was made by the two institutions revolutionized fluid management and topical management of burn care forever."
Still, they could not halt the staph infections that kill most burn victims—which prompted the first civilian use of a miracle elixir that was being secretly developed in government-sponsored labs and that ultimately ushered in a new age in therapeutics. Military officials quickly realized this disaster could provide an excellent natural laboratory to test the effectiveness of this drug and see if it could be used to treat the acute traumas of combat in this unfortunate civilian approximation of battlefield conditions. At the time, the very existence of this wondrous medicine—penicillin—was a closely guarded military secret.
From Forgotten Lab Experiment to Wonder Drug
In 1928, Alexander Fleming discovered the curative powers of penicillin, which promised to eradicate infectious pathogens that killed millions every year. But the road to mass producing enough of the highly unstable mold was littered with seemingly unsurmountable obstacles and it remained a forgotten laboratory curiosity for over a decade. But Fleming never gave up and penicillin's eventual rescue from obscurity was a landmark in scientific history.
In 1940, a group at Oxford University, funded in part by the Rockefeller Foundation, isolated enough penicillin to test it on twenty-five mice, which had been infected with lethal doses of streptococci. Its therapeutic effects were miraculous—the untreated mice died within hours, while the treated ones played merrily in their cages, undisturbed. Subsequent tests on a handful of patients, who were brought back from the brink of death, confirmed that penicillin was indeed a wonder drug. But Britain was then being ravaged by the German Luftwaffe during the Blitz, and there were simply no resources to devote to penicillin during the Nazi onslaught.
In June of 1941, two of the Oxford researchers, Howard Florey and Ernst Chain, embarked on a clandestine mission to enlist American aid. Samples of the temperamental mold were stored in their coats. By October, the Roosevelt Administration had recruited four companies—Merck, Squibb, Pfizer and Lederle—to team up in a massive, top-secret development program. Merck, which had more experience with fermentation procedures, swiftly pulled away from the pack and every milligram they produced was zealously hoarded.
After the nightclub fire, the government ordered Merck to dispatch to Boston whatever supplies of penicillin that they could spare and to refine any crude penicillin broth brewing in Merck's fermentation vats. After working in round-the-clock relays over the course of three days, on the evening of December 1st, 1942, a refrigerated truck containing thirty-two liters of injectable penicillin left Merck's Rahway, New Jersey plant. It was accompanied by a convoy of police escorts through four states before arriving in the pre-dawn hours at Massachusetts General Hospital. Dozens of people were rescued from near-certain death in the first public demonstration of the powers of the antibiotic, and the existence of penicillin could no longer be kept secret from inquisitive reporters and an exultant public. The next day, the Boston Globe called it "priceless" and Time magazine dubbed it a "wonder drug."
Within fourteen months, penicillin production escalated exponentially, churning out enough to save the lives of thousands of soldiers, including many from the Normandy invasion. And in October 1945, just weeks after the Japanese surrender ended World War II, Alexander Fleming, Howard Florey and Ernst Chain were awarded the Nobel Prize in medicine. But penicillin didn't just save lives—it helped build some of the most innovative medical and scientific companies in history, including Merck, Pfizer, Glaxo and Sandoz.
"Every war has given us a new medical advance," concludes Marshall. "And penicillin was the great scientific advance of World War II."

Ordinary people are living better with chronic conditions thanks to a recent explosion of developments in medical implants.
The demand for transplantable organs dwarfs their availability. There are currently over 100,000 people on the transplant waiting list in the U.S., compared to 40,000 transplants completed in 2021. But even this doesn’t reflect the number of people in dire straits who don’t qualify for a transplant because of things like frailty, smoking status and their low odds of surviving the surgery.
My journey to becoming a cyborg came about because of a lifelong medical condition characterized by pathologically low motility of the digestive system, called gastroparesis. Ever since I was in my teens, I’ve had chronic problems with severe nausea. Flareups can be totally incapacitating and last anywhere from hours to months, interspersed with periods of relief. The cycle is totally unpredictable, and for decades my condition went both un- and misdiagnosed by doctors who were not even aware that the condition existed. Over the years I was labeled with whatever fashionable but totally inappropriate medical label existed at the time, and not infrequently, hypochondria.
Living with the gastric pacer is easy. In fact, most of the time, I don’t even know it’s there.
One of the biggest turning points in my life came when a surgeon at the George Washington University Hospital, Dr. Frederick Brody, ordered a gastric emptying test that revealed gastroparesis. This was in 2009, and an implantable device, called a gastric pacer, had been approved by the FDA for compassionate use, meaning that no other treatments were available. The small device is like a pacemaker that’s implanted beneath the skin of the abdomen and is attached to the stomach through electrodes that carry electrical pulses that stimulate the stomach, making it contract as it’s supposed to.
Dr. Brody implanted the electrical wires and the device, and, once my stomach started to respond to the pulses, I got the most significant nausea relief I’d had in decades of futile treatments. It sounds cliché to say that my debt to Dr. Brody is immeasurable, but the pacer has given me more years of relative normalcy than I previously could have dreamed of.
I should emphasize that the pacer is not a cure. I still take a lot of medicine and have to maintain a soft, primarily vegetarian diet, and the condition has progressed with age. I have ups and downs, and can still have periods of severe illness, but there’s no doubt I would be far worse off without the electrical stimulation provided by the pacer.
Living with the gastric pacer is easy. In fact, most of the time, I don’t even know it’s there. It entails periodic visits with a surgeon who can adjust the strength of the electrical pulses using a wireless device, so when symptoms are worse, he or she can amp up the juice. If the pulses are too strong, they can cause annoying contractions in the abdominal muscles, but this is easily fixed with a simple wireless adjustment. The battery runs down after a few years, and when this happens the whole device has to be replaced in what is considered minor surgery.
Such devices could fill gaps in treating other organ failures. By far most of the people on transplant waiting lists are waiting for kidneys. Despite the fact that live donations are possible, there’s still a dire shortage of organs. A bright spot on the horizon is The Kidney Project, a program spearheaded by bioengineer Shuvo Roy at the University of California, San Francisco, which is developing a fully implantable artificial kidney. The device combines living cells with artificial materials and relies not on a battery, but on the patient’s own blood pressure to keep it functioning.
Several years into this project, a prototype of the kidney, about the size of a smart phone, has been successfully tested in pigs. The device seems to provide many of the functions of a biological kidney (unlike dialysis, which replaces only one main function) and reliably produces urine. One of its most critical components is a special artificial membrane, called a hemofilter, that filters out toxins and waste products from the blood without leaking important molecules like albumin. Since it allows for total mobility, the artificial kidney will provide patients with a higher quality of life than those on dialysis, and is in some important ways, even better than a biological transplant.
The beauty of the device is that, even though it contains kidney cells sourced, as of now, from cadavers or pigs, the cells are treated so that they can’t be rejected and the device doesn’t require the highly problematic immunosuppressant drugs a biological organ requires. “Anti-rejection drugs,” says Roy, “make you susceptible to all kinds of infections and damage the transplanted organ, causing steady deterioration. Eventually they kill the kidney. A biological transplant has about a 10-year limit,” after which the kidney fails and the body rejects it.
Eventually, says Roy, the cells used in the artificial kidney will be sourced from the patient himself, the ultimate genetic match. The patient’s adult stem cells can be used to produce some or all of the 25 to 30 specialized cells of a biological kidney that provide all the functions of a natural organ. People formerly on dialysis could drastically improve their functionality and quality of life without being tethered to a machine for hours at a time, three days a week.
As exciting as this project is, it suffers from a common theme in early biomedical research—keeping a steady stream of funding that will move the project from the lab, into human clinical trials and eventually to the bedside. “It’s the issue,” says Roy. “Potential investors want to see more data indicating that it works, but you need funding to create data. It’s a Catch-22 that puts you in a kind of no-man’s land of funding.” The constant pursuit of funding introduces a variable that makes it hard to predict when the kidney will make it to market, despite the enormous need for such a technology.
Another critical variable is if and when insurance companies will decide to cover transplants with the artificial kidney, so that it becomes affordable for the average person. But Roy thinks that this hurdle, too, will be crossed. Insurance companies stand to save a great deal of money compared to what they ordinarily spend on transplant patients. The cost of yearly maintenance will be a fraction of that associated with the tens of thousands of dollars for immunosuppressant drugs and the attendant complications associated with a biological transplant.
One estimate that the multidisciplinary team of researchers involved with The Kidney Project are still trying to establish is how long the artificial kidney will last once transplanted into the body. Animal trials so far have been looking at how the kidney works for 30 days, and will soon extend that study to 90 days. Additional studies will extend much farther into the future, but first the kidneys have to be implanted into people who can be followed over many years to answer this question. But unlike the gastric pacer and other implants, there won’t be a need for periodic surgeries to replace a depleted battery, and the stark improvements in quality of life compared to dialysis add a special dimension to the value of whatever time the kidney lasts.
Another life-saving implant could address a major scourge of the modern world—heart disease. Despite significant advances in recent decades, including the cardiac implants mentioned above, cardiovascular disease still causes one in three deaths across the world. One of the most promising developments in recent years is the Total Artificial Heart, a pneumatically driven device that can be used in patients with biventricular heart failure, affecting both sides of the heart, when a biological organ is not available.
The TAH is implanted in the chest cavity and has two tubes that snake down the body, come out through the abdomen and attach to a 13.5-pound external driver that the patient carries around in a backpack. It was first developed as a bridge to transplant, a temporary alternative while the patient waited for a biological heart to replace it. However, SynCardia Systems, LLC, the Tucson-based company that makes it, is now investigating whether the heart can be used on a long-term basis.
There’s good reason to think that this will be the case. I spoke with Daniel Teo, one of the board members of SynCardia, who said that so far, one patient lived with the TAH for six years and nine months, before he died of other causes. Another patient, still alive, has lived with the device for over five years and another one has lived with it for over four years. About 2,000 of these transplants have been done in patients waiting for biological hearts so far, and most have lived mobile, even active lives. One TAH recipient hiked for 600 miles, and another ran the 4.2-mile Pat Tillman Run, both while on the artificial heart. This is a far cry from their activities before surgery, while living with advanced heart failure.

Randy Shepard, a recipient of the Total Artificial Heart, teaches archery to his son.
Randy Shepard
If removing and replacing one’s biological heart with a synthetic device sounds scary, it is. But then so is replacing one’s heart with biological one. “The TAH is very emotionally loaded for most people,” says Teo. “People sometimes hold back because of philosophical, existential questions and other nonmedical reasons.” He also cites cultural reasons why some people could be hesitant to accept an artificial heart, saying that some religions could frown upon it, just as they forbid other medical interventions.
The first TAHs that were approved were 70 cubic centimeters in size and fit into the chest cavities of men and larger women, but there’s now a smaller, 50 cc size meant for women and adolescents. The FDA first cleared the 70 cc heart as a bridge to transplant in 2004, and the 50 cc model received approval in 2014. SynCardia’s focus now is on seeking FDA approval to use the heart on a long-term basis. There are other improvements in the works.
One issue being refined deals with the external driver that holds the pneumatic device for moving the blood through a patient’s body. The two tubes connecting the driver to the heart entail openings in the skin that could get infected, and carrying the backpack is less than ideal. The driver also makes an audible sound that some people find disturbing. The next generation TAH will be quieter and involve wearing a smaller, lighter device on a belt rather than carrying the backpack. SynCardia is also working toward a fully implantable heart that wouldn’t require any external components and would contain an energy source that can be recharged wirelessly.
Teo says the jury is out as to whether artificial hearts will ever obviate the need for biological organs, but the world’s number one killer isn’t going away any time soon. “The heart is one of the strongest organs,” he says, “but it’s not made to last forever. If you live long enough, the heart will eventually fail, and heart failure leads to the failure of other organs like the kidney, the lungs and the liver.” As long as this remains the case and as long as the current direction of research continues, artificial organs are likely to play an ever larger part of our everyday lives.
Oh, wait. Maybe we cyborgs will take over the world after all.
