
Pregnant & Breastfeeding Women Who Get the COVID-19 Vaccine Are Protecting Their Infants, Research Suggests

Becky Cummings, who got vaccinated in December, snuggles her newborn, Clark, while he takes a nap.
Becky Cummings had multiple reasons to get vaccinated against COVID-19 while tending to her firstborn, Clark, who arrived in September 2020 at 27 weeks.
The 29-year-old intensive care unit nurse in Greensboro, North Carolina, had witnessed the devastation day in and day out as the virus took its toll on the young and old. But when she was offered the vaccine, she hesitated, skeptical of its rapid emergency use authorization.
Exclusion of pregnant and lactating mothers from clinical trials fueled her concerns. Ultimately, though, she concluded the benefits of vaccination outweighed the risks of contracting the potentially deadly virus.
"Long story short," Cummings says, in December "I got vaccinated to protect myself, my family, my patients, and the general public."
At the time, Cummings remained on the fence about breastfeeding, citing a lack of evidence to support its safety after vaccination, so she pumped and stashed breast milk in the freezer. Her son is adjusting to life as a preemie, requiring mother's milk to be thickened with formula, but she's becoming comfortable with the idea of breastfeeding as more research suggests it's safe.
"If I could pop him on the boob," she says, "I would do it in a heartbeat."
Now, a study recently published in the Journal of the American Medical Association found "robust secretion" of specific antibodies in the breast milk of mothers who received a COVID-19 vaccine, indicating a potentially protective effect against infection in their infants.
The presence of antibodies in the breast milk, detectable as early as two weeks after vaccination, lasted for six weeks after the second dose of the Pfizer-BioNTech vaccine.
"We believe antibody secretion into breast milk will persist for much longer than six weeks, but we first wanted to prove any secretion at all after vaccination," says Ilan Youngster, the study's corresponding author and head of pediatric infectious diseases at Shamir Medical Center in Zerifin, Israel.
That's why the research team performed a preliminary analysis at six weeks. "We are still collecting samples from participants and hope to soon be able to comment about the duration of secretion."
As with other respiratory illnesses, such as influenza and pertussis, secretion of antibodies in breast milk confers protection from infection in infants. The researchers expect a similar immune response from the COVID-19 vaccine and are expecting the findings to spur an increase in vaccine acceptance among pregnant and lactating women.
A COVID-19 outbreak struck three families the research team followed in the study, resulting in at least one non-breastfed sibling developing symptomatic infection; however, none of the breastfed babies became ill. "This is obviously not empirical proof," Youngster acknowledges, "but still a nice anecdote."
Leaps.org inquired whether infants who derive antibodies only through breast milk are likely to have a lower immunity than infants whose mothers were vaccinated while they were in utero. In other words, is maternal transmission of antibodies stronger during pregnancy than during breastfeeding, or about the same?
"This is a different kind of transmission," Youngster explains. "When a woman is infected or vaccinated during pregnancy, some antibodies will be transferred through the placenta to the baby's bloodstream and be present for several months." But in the nursing mother, that protection occurs through local action. "We always recommend breastfeeding whenever possible, and, in this case, it might have added benefits."
A study published online in March found COVID-19 vaccination provided pregnant and lactating women with robust immune responses comparable to those experienced by their nonpregnant counterparts. The study, appearing in the American Journal of Obstetrics and Gynecology, documented the presence of vaccine-generated antibodies in umbilical cord blood and breast milk after mothers had been vaccinated.
Natali Aziz, a maternal-fetal medicine specialist at Stanford University School of Medicine, notes that it's too early to draw firm conclusions about the reduction in COVID-19 infection rates among newborns of vaccinated mothers. Citing the two aforementioned research studies, she says it's biologically plausible that antibodies passed through the placenta and breast milk impart protective benefits. While thousands of pregnant and lactating women have been vaccinated against COVID-19, without incurring adverse outcomes, many are still wondering whether it's safe to breastfeed afterward.
It's important to bear in mind that pregnant women may develop more severe COVID-19 complications, which could lead to intubation or admittance to the intensive care unit. "We, in our practice, are supporting pregnant and breastfeeding patients to be vaccinated," says Aziz, who is also director of perinatal infectious diseases at Stanford Children's Health, which has been vaccinating new mothers and other hospitalized patients at discharge since late April.
Earlier in April, Huntington Hospital in Long Island, New York, began offering the COVID-19 vaccine to women after they gave birth. The hospital chose the one-shot Johnson & Johnson vaccine for postpartum patients, so they wouldn't need to return for a second shot while acclimating to life with a newborn, says Mitchell Kramer, chairman of obstetrics and gynecology.
The hospital suspended the program when the Food and Drug Administration and the Centers for Disease Control and Prevention paused use of the J&J vaccine starting April 13, while investigating several reports of dangerous blood clots and low platelet counts among more than 7 million people in the United States who had received that vaccine.
In lifting the pause April 23, the agencies announced the vaccine's fact sheets will bear a warning of the heightened risk for a rare but serious blood clot disorder among women under age 50. As a result, Kramer says, "we will likely not be using the J&J vaccine for our postpartum population."
So, would it make sense to vaccinate infants when one for them eventually becomes available, not just their mothers? "In general, most of the time, infants do not have as good of an immune response to vaccines," says Jonathan Temte, associate dean for public health and community engagement at the University of Wisconsin School of Medicine and Public Health in Madison.
"Many of our vaccines are held until children are six months of age. For example, the influenza vaccine starts at age six months, the measles vaccine typically starts one year of age, as do rubella and mumps. Immune response is typically not very good for viral illnesses in young infants under the age of six months."
So far, the FDA has granted emergency use authorization of the Pfizer-BioNTech vaccine for children as young as 16 years old. The agency is considering data from Pfizer to lower that age limit to 12. Studies are also underway in children under age 12. Meanwhile, data from Moderna on 12-to 17-year-olds and from Pfizer on 12- to 15-year-olds have not been made public. (Pfizer announced at the end of March that its vaccine is 100 percent effective in preventing COVID-19 in the latter age group, and FDA authorization for this population is expected soon.)
"There will be step-wise progression to younger children, with infants and toddlers being the last ones tested," says James Campbell, a pediatric infectious diseases physician and head of maternal and child clinical studies at the University of Maryland School of Medicine Center for Vaccine Development.
"Once the data are analyzed for safety, tolerability, optimal dose and regimen, and immune responses," he adds, "they could be authorized and recommended and made available to American children." The data on younger children are not expected until the end of this year, with regulatory authorization possible in early 2022.
For now, Vonnie Cesar, a family nurse practitioner in Smyrna, Georgia, is aiming to persuade expectant and new mothers to get vaccinated. She has observed that patients in metro Atlanta seem more inclined than their rural counterparts.
To quell some of their skepticism and fears, Cesar, who also teaches nursing students, conceived a visual way to demonstrate the novel mechanism behind the COVID-19 vaccine technology. Holding a palm-size physical therapy ball outfitted with clear-colored push pins, she simulates the spiked protein of the coronavirus. Slime slathered at the gaps permeates areas around the spikes—a process similar to how our antibodies build immunity to the virus.
These conversations often lead hesitant patients to discuss vaccination with their husbands or partners. "The majority of people I'm speaking with," she says, "are coming to the conclusion that this is the right thing for me, this is the common good, and they want to make sure that they're here for their children."
CORRECTION: An earlier version of this article mistakenly stated that the COVID-19 vaccines were granted emergency "approval." They have been granted emergency use authorization, not full FDA approval. We regret the error.
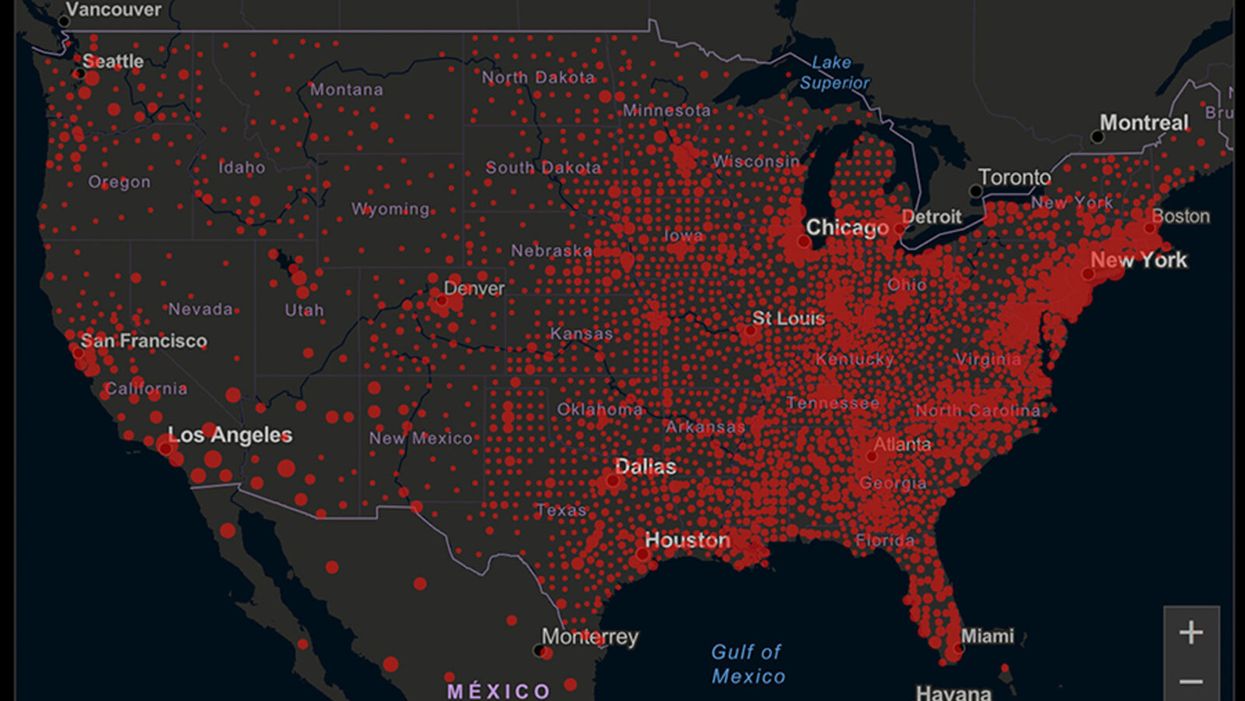
A map of cumulative known cases of COVID-19 in the U.S., as of June 12th, 2020.
Have you felt a bit like an armchair epidemiologist lately? Maybe you've been poring over coronavirus statistics on your county health department's website or on the pages of your local newspaper.
If the percentage of positive tests steadily stays under 8 percent, that's generally a good sign.
You're likely to find numbers and charts but little guidance about how to interpret them, let alone use them to make day-to-day decisions about pandemic safety precautions.
Enter the gurus. We asked several experts to provide guidance for laypeople about how to navigate the numbers. Here's a look at several common COVID-19 statistics along with tips about how to understand them.
Case Counts: Consider the Context
The number of confirmed COVID-19 cases in American counties is widely available. Local and state health departments should provide them online, or you can easily look them up at The New York Times' coronavirus database. However, you need to be cautious about interpreting them.
"Case counts are the obvious numbers to look at. But they're probably the hardest thing to sort out," said Dr. Jeff Martin, an epidemiologist at the University of California at San Francisco.
That's because case counts by themselves aren't a good window into how the coronavirus is affecting your community since they rely on testing. And testing itself varies widely from day to day and community to community.
"The more testing that's done, the more infections you'll pick up," explained Dr. F. Perry Wilson, a physician at Yale University. The numbers can also be thrown off when tests are limited to certain groups of people.
"If the tests are being mostly given to people with a high probability of having been infected -- for example, they have had symptoms or work in a high-risk setting -- then we expect lots of the tests to be positive. But that doesn't tell us what proportion of the general public is likely to have been infected," said Eleanor Murray, an epidemiologist at Boston University.
These Stats Are More Meaningful
According to Dr. Wilson, it's more useful to keep two other statistics in mind: the number of COVID tests that are being performed in your community and the percentage that turn up positive, showing that people have the disease. (These numbers may or may not be available locally. Check the websites of your community's health department and local news media outlets.)
If the number of people being tested is going up, but the percentage of positive tests is going down, Dr. Wilson said, that's a good sign. But if both numbers are going up – the number of people tested and the percentage of positive results – then "that's a sign that there are more infections burning in the community."
It's especially worrisome if the percentage of positive cases is growing compared to previous days or weeks, he said. According to him, that's a warning of a "high-risk situation."
Dr. George Rutherford, an epidemiologist at University of California at San Francisco, offered this tip: If the percentage of positive tests steadily stays under 8 percent, that's generally a good sign.
There's one more caveat about case counts. It takes an average of a week for someone to be infected with COVID-19, develop symptoms, and get tested, Dr. Rutherford said. It can take an additional several days for those test results to be reported to the county health department. This means that case numbers don't represent infections happening right now, but instead are a picture of the state of the pandemic more than a week ago.
Hospitalizations: Focus on Current Statistics
You should be able to find numbers about how many people in your community are currently hospitalized – or have been hospitalized – with diagnoses of COVID-19. But experts say these numbers aren't especially revealing unless you're able to see the number of new hospitalizations over time and track whether they're rising or falling. This number often isn't publicly available, however.
If new hospitalizations are increasing, "you may want to react by being more careful yourself."
And there's an important caveat: "The problem with hospitalizations is that they do lag," UC San Francisco's Dr. Martin said, since it takes time for someone to become ill enough to need to be hospitalized. "They tell you how much virus was being transmitted in your community 2 or 2.5 weeks ago."
Also, he said, people should be cautious about comparing new hospitalization rates between communities unless they're adjusted to account for the number of more-vulnerable older people.
Still, if new hospitalizations are increasing, he said, "you may want to react by being more careful yourself."
Deaths: They're an Even More Delayed Headline
Cable news networks obsessively track the number of coronavirus deaths nationwide, and death counts for every county in the country are available online. Local health departments and media websites may provide charts tracking the growth in deaths over time in your community.
But while death rates offer insight into the disease's horrific toll, they're not useful as an instant snapshot of the pandemic in your community because severely ill patients are typically sick for weeks. Instead, think of them as a delayed headline.
"These numbers don't tell you what's happening today. They tell you how much virus was being transmitted 3-4 weeks ago," Dr. Martin said.
'Reproduction Value': It May Be Revealing
You're not likely to find an available "reproduction value" for your community, but it is available for your state and may be useful.
A reproduction value, also known as R0 or R-naught, "tells us how many people on average we expect will be infected from a single case if we don't take any measures to intervene and if no one has been infected before," said Boston University's Murray.
As The New York Times explained, "R0 is messier than it might look. It is built on hard science, forensic investigation, complex mathematical models — and often a good deal of guesswork. It can vary radically from place to place and day to day, pushed up or down by local conditions and human behavior."
It may be impossible to find the R0 for your community. However, a website created by data specialists is providing updated estimates of a related number -- effective reproduction number, or Rt – for each state. (The R0 refers to how infectious the disease is in general and if precautions aren't taken. The Rt measures its infectiousness at a specific time – the "t" in Rt.) The site is at rt.live.
"The main thing to look at is whether the number is bigger than 1, meaning the outbreak is currently growing in your area, or smaller than 1, meaning the outbreak is currently decreasing in your area," Murray said. "It's also important to remember that this number depends on the prevention measures your community is taking. If the Rt is estimated to be 0.9 in your area and you are currently under lockdown, then to keep it below 1 you may need to remain under lockdown. Relaxing the lockdown could mean that Rt increases above 1 again."
"Whether they're on the upswing or downswing, no state is safe enough to ignore the precautions about mask wearing and social distancing."
Keep in mind that you can still become infected even if an outbreak in your community appears to be slowing. Low risk doesn't mean no risk.
Putting It All Together: Why the Numbers Matter
So you've reviewed COVID-19 statistics in your community. Now what?
Dr. Wilson suggests using the data to remind yourself that the coronavirus pandemic "is still out there. You need to take it seriously and continue precautions," he said. "Whether they're on the upswing or downswing, no state is safe enough to ignore the precautions about mask wearing and social distancing. 'My state is doing well, no one I know is sick, is it time to have a dinner party?' No."
He also recommends that laypeople avoid tracking COVID-19 statistics every day. "Check in once a week or twice a month to see how things are going," he suggested. "Don't stress too much. Just let it remind you to put that mask on before you get out of your car [and are around others]."
GOOD10: The Pandemic Issue explores big-picture ways that science innovation and communication can usher in a more equitable, more progress-oriented, and safer world.
This issue is a collaboration among GOOD, leapsmag, and the Aspen Institute Science & Society Program.
The GOOD10 format explores fundamental issues facing humanity through the lenses of ten forces pushing the needle toward progress: Places, Philanthropists, Celebrities, Whistleblowers, Companies, Media, Products, Politicians, Scientists, and Actions. Across these categories, we seek to present unexpected and encouraging paradigms emerging from this historic crisis.
This special issue is available as an e-reader version for both desktop and mobile. It is also available as a free downloadable PDF.
TABLE OF CONTENTS:
- PLACES:
55 Lessons Learned About Science Communication Around the World; Quarantining Our Way Into Outer Space - PLACES:
Quarantining Our Way Into Outer Space - PHILANTHROPISTS:
An Exclusive Interview with Wendy Schmidt about Science in the Pandemic Era - CELEBRITIES:
Neil deGrasse Tyson Wants Celebrities to Promote Scientists - WHISTLEBLOWERS:
The Science Sleuths Holding Fraudulent Research Accountable - COMPANIES:
The Biggest Challenge for a COVID-19 Vaccine: Making It Accessible and Affordable - MEDIA:
Isaac Asimov on the History of Infectious Disease—And How Humanity Learned To Fight Back - PRODUCTS:
Will COVID-19 Pave the Way For DIY Precision Medicine? - POLITICIANS:
Will the Pandemic Propel STEM Experts to Political Power? - SCIENTISTS:
Would a Broad-Spectrum Antiviral Drug Stop the Pandemic? - ACTIONS:
Pseudoscience is Rampant: How Not to Fall For It - ACTIONS:
How COVID-19 Could Usher In a New Age of Collective Drug Discovery
THE EVENT:
"The Pandemic Science Summit" focused on how science innovation is key to society's future stability as we emerge from the pandemic, featuring:

Christopher Bailey – Arts and Health Lead, World Health Organization

Elisabeth Bik, Ph.D. – Microbiologist and scientific integrity consultant

Margaret Hamburg, M.D. – Foreign Secretary, National Academy of Medicine; former Commissioner, U.S. Food and Drug Administration

Peggy Oti-Boateng, Ph.D. – Director, Division of Science Policy and Capacity- Building, UNESCO

George Yancopoulos, M.D., Ph.D. – President and Chief Scientific Officer, Regeneron Pharmaceuticals
Kira Peikoff was the editor-in-chief of Leaps.org from 2017 to 2021. As a journalist, her work has appeared in The New York Times, Newsweek, Nautilus, Popular Mechanics, The New York Academy of Sciences, and other outlets. She is also the author of four suspense novels that explore controversial issues arising from scientific innovation: Living Proof, No Time to Die, Die Again Tomorrow, and Mother Knows Best. Peikoff holds a B.A. in Journalism from New York University and an M.S. in Bioethics from Columbia University. She lives in New Jersey with her husband and two young sons. Follow her on Twitter @KiraPeikoff.