


A rendering of a 3D-printed burger.
Imagine it's 2050. You wake up and make breakfast: fluffy scrambled eggs that didn't come from a chicken, but that taste identical to the ones you remember eating as a kid. You would never know that the egg protein on your plate, ovalbumin, was developed in an industrial bioreactor using fungi.
"We have this freedom to operate, freedom to engineer way beyond what we have now with livestock or plants."
For lunch, you head to your kitchen's 3D printer and pop in a cartridge, select your preferred texture and flavor, then stand back while your meal is chemically assembled. Afterward, for dessert, you snack on some chocolate that tastes more delicious than the truffles of the past. That's because these cocoa beans were gene-edited to improve their flavor.
2050 is not a random year –it's when the United Nations estimates that the world population will have ballooned to nearly 10 billion people. That's a staggering number of mouths to feed. So, scientists are already working on ways to make new food products that are unlike anything we consume today, but that could offer new, potentially improved nutritional choices and sustainable options for the masses. To whet your appetite, here are three futuristic types of food that are currently in development around the world:
1) Cellular Agriculture
Researchers at VTT Technical Research Centre of Finland, a leading R&D organization in Europe, are on the cutting-edge of developing a whole new ecosystem of food with novel ingredients and novel functionality.
In the high-tech world of cellular agriculture, single-cell organisms can be used in contained environments to produce food ingredients that are identical to traditionally sourced ingredients. For example, whey protein can be developed inside a bioreactor that is functionally the same as the kind in cow's milk.
Ditto for eggs without a chicken – so the world will finally know which came first.

The steel tank bioreactors in VTT´s piloting facility are used to grow larger amounts of plant cells or to brew dairy and egg proteins with microbes.
(VTT)
"We take the gene from a chicken genome, and place that in a microbe, and then the microbe can, with those instructions, make exactly the same protein," explains Lauri Reuter, a Senior Specialist at VTT who holds a doctorate in biotechnology. "It will swim in this bioreactor and kick out the protein, and we get this liquid that can be purified. Then you would cook or bake with it, and the food you would eat tastes and looks like food you would eat right now."
But why settle for what chickens can do? With this technology, it's possible, for example, to modify the ovalbumin protein to decrease its allergenicity.
"This is the power of what we can do with modern tools of genetic engineering," says Christopher Landowski,a Research Team Leader of the Protein Production Team. And the innovative potential doesn't stop there.
"We have this freedom to operate, freedom to engineer way beyond what we have now with livestock or plants," Reuter says. Future foods sourced from cells could include meat analogues, sugar substitutes, dairy substitutes, nutritious veggies that don't taste bitter, personalized nutrition – ingredients designed for individual needs; the list goes on. It could even be used one day to produce food on Mars.
The researchers emphasize the advantages of this method: their living cell factories are efficient – no care of complex animals is required; they can scale up or down in reaction to demand; their environments are contained and don't require antibiotics; and they provide an alternative to using animals.
But the researchers also readily admit that the biggest obstacle is consumer acceptance, which is why they seek to engage with people along the way to alleviate any concerns and to educate them about the technology. Novel foods of this sort have already been eaten in research settings, but it may take another three to five years before the egg and milk proteins hit the market, probably first in the United States before Europe.
Eventually, the researchers anticipate widespread adoption.
Emilia Nordlund, who directs the Food Solutions team, predicts, "Cellular agriculture will revolutionize the food industry as dramatically as the Internet revolutionized many other industries."

Jams made of culture cells of various plants: strawberry, scurvy grass, arctic bramble, tobacco, cloudberry and lingonberry.
(VTT/Lauri Reuter)
2) 3D-printed foods
In South Korea, researchers are developing 3D-printed foods to help solve a problem caused by aging. Elderly people often rely on soft foods which are easier to chew, but aren't always healthy, like Jello and pudding.
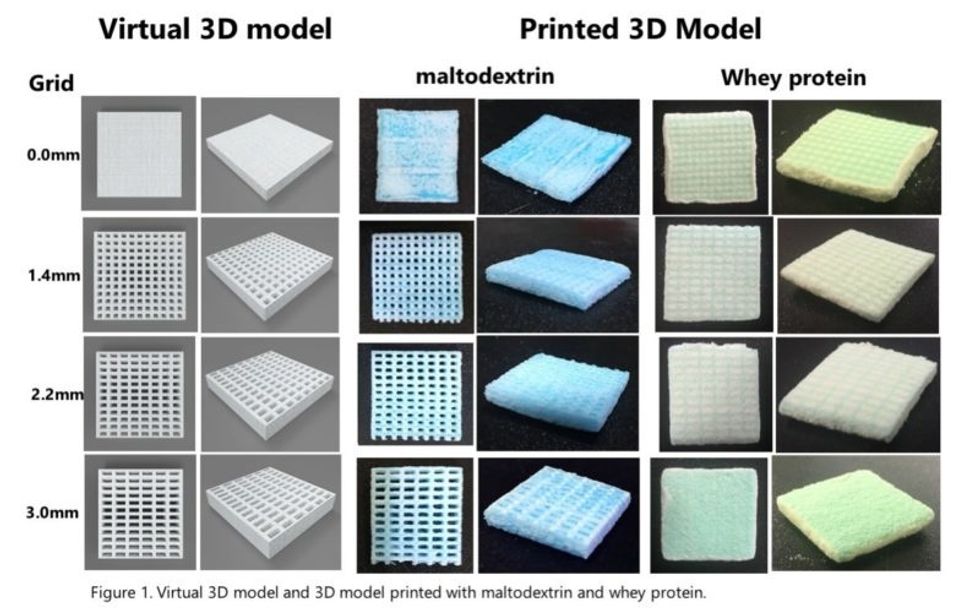
With 3D printing, foods of softer textures can be created with the same nutritional value as firmer food, via a processing method that breaks down the food into tiny nutrients by grinding it at a very low temperature with liquid nitrogen.
"The goal is that someone at home can print out food with whatever flavor and texture they want."
The micro-sized food materials are then reconstructed in layers to form what looks like a Lego block. "The cartridges are all textures, some soft and some stiff," explains Jin-Kyu Rhee, associate professor at Ewha Womans University, whose project has been funded for the last three years by the South Korean government. "We are developing a library of food textures, so that people can combine them to simulate a real type of food."
Users could then add powdered versions of various ingredients to create customized food. Flavor, of course, is of prime importance too, so the cartridges have flavors like barbecue to help simulate the experience of eating "real" food.
"The goal is that someone at home can print out food with whatever flavor and texture they want," Rhee says. "They can order their own cartridge and digital recipes to generate their own food, ready to cook with a microwave oven." It could also be used for space travel.
Rhee expects the prototype of the printer to be completed by the end of this year and will then seek out a commercial partner. If all goes well, you might be able to set up your 3D printer next to your coffee pot by 2025.
3) CRISPR-edited foods
You may not know that the cocoa plant is having a tough time out there in nature. It's plagued by fungal disease; on farms, about 30 to 40 percent of the potential cocoa beans are lost every year. For all the chocolate lovers of the world, this means less to go around.
Conventional plant breeding is very slow for trees, so researchers like Mark Guiltinan at Penn State University are devising ways to increase the plants' chances for survival – without moving any genes between species, as in genetically modified organisms (GMOs).
"Because society hasn't really embraced [GMOs] very much, we're trying to develop ways that don't use transgenic plants and speed up breeding," Guiltinan says.
He and his colleagues are using CRISPR-cas9, the precise method of editing DNA, to imbue cocoa plants with immunity to fungal disease.
How does it work? Similar to humans, the plants have an immune system. Part of it functions like brakes, repressing the whole system so it's only working when it needs to.
"Like when you get a fever, your immune system is working full blast, but your body shuts it down when it doesn't need it," he explains. "Plants do exactly the same thing. One idea is if we can reduce or eliminate that brake on the immune system, we could make plants that have a very high immunity."

A CRISPR-edited npr3 mutant cacao plantlet, not too much to see yet, but soon it will become a happy plant in the greenhouse.
(Photo credit: Mark Guiltinan)
The CRISPR-cas9 system allows "a really amazing little protein" to go into the cocoa plant cell, find a specific gene, and shut it off to put the whole immune system into overdrive. This confers the necessary immunity, and though the plant burns through a lot of energy, as if it has a fever all the time, this method would allow for more plants to fend off the fungal attacks every year. Which means more chocolate. It could also greatly reduce the need for pesticides.
"Replacing chemicals with genetics is one part of our goal," Guiltinan says. "And it's totally safe." Another goal of his project is to improve the cocoa beans' quality and flavor profile through gene editing.
Yum. Is your mouth watering yet?
