
A new injection is helping stave off RSV this season

The FDA approved a single-dose, long-acting injection to protect babies and toddlers from RSV over the fall and winter.
In November 2021, Mickayla Wininger’s then one-month-old son, Malcolm, endured a terrifying bout with RSV, the respiratory syncytial (sin-SISH-uhl) virus—a common ailment that affects all age groups. Most people recover from mild, cold-like symptoms in a week or two, but RSV can be life-threatening in others, particularly infants.
Wininger, who lives in southern Illinois, was dressing Malcolm for bed when she noticed what seemed to be a minor irregularity with this breathing. She and her fiancé, Gavin McCullough, planned to take him to the hospital the next day. The matter became urgent when, in the morning, the boy’s breathing appeared to have stopped.
After they dialed 911, Malcolm started breathing again, but he ended up being hospitalized three times for RSV and defects in his heart. Eventually, he recovered fully from RSV, but “it was our worst nightmare coming to life,” Wininger recalled.
It’s a scenario that the federal government is taking steps to prevent. In July, the Food and Drug Administration approved a single-dose, long-acting injection to protect babies and toddlers. The injection, called Beyfortus, or nirsevimab, became available this October. It reduces the incidence of RSV in pre-term babies and other infants for their first RSV season. Children at highest risk for severe RSV are those who were born prematurely and have either chronic lung disease of prematurity or congenital heart disease. In those cases, RSV can progress to lower respiratory tract diseases such as pneumonia and bronchiolitis, or swelling of the lung’s small airway passages.
Each year, RSV is responsible for 2.1 million outpatient visits among children younger than five-years-old, 58,000 to 80,000 hospitalizations in this age group, and between 100 and 300 deaths, according to the Centers for Disease Control and Prevention. Transmitted through close contact with an infected person, the virus circulates on a seasonal basis in most regions of the country, typically emerging in the fall and peaking in the winter.
In August, however, the CDC issued a health advisory on a late-summer surge in severe cases of RSV among young children in Florida and Georgia. The agency predicts "increased RSV activity spreading north and west over the following two to three months.”
Infants are generally more susceptible to RSV than older people because their airways are very small, and their mechanisms to clear these passages are underdeveloped. RSV also causes mucus production and inflammation, which is more of a problem when the airway is smaller, said Jennifer Duchon, an associate professor of newborn medicine and pediatrics in the Icahn School of Medicine at Mount Sinai in New York.
In 2021 and 2022, RSV cases spiked, sending many to emergency departments. “RSV can cause serious disease in infants and some children and results in a large number of emergency department and physician office visits each year,” John Farley, director of the Office of Infectious Diseases in the FDA’s Center for Drug Evaluation and Research, said in a news release announcing the approval of the RSV drug. The decision “addresses the great need for products to help reduce the impact of RSV disease on children, families and the health care system.”
Sean O’Leary, chair of the committee on infectious diseases for the American Academy of Pediatrics, says that “we’ve never had a product like this for routine use in children, so this is very exciting news.” It is recommended for all kids under eight months old for their first RSV season. “I would encourage nirsevimab for all eligible children when it becomes available,” O’Leary said.
For those children at elevated risk of severe RSV and between the ages of 8 and 19 months, the CDC recommends one dose in their second RSV season.
The drug will be “really helpful to keep babies healthy and out of the hospital,” said O’Leary, a professor of pediatrics at the University of Colorado Anschutz Medical Campus/Children’s Hospital Colorado in Denver.
An antiviral drug called Synagis (palivizumab) has been an option to prevent serious RSV illness in high-risk infants since it was approved by the FDA in 1998. The injection must be given monthly during RSV season. However, its use is limited to “certain children considered at high risk for complications, does not help cure or treat children already suffering from serious RSV disease, and cannot prevent RSV infection,” according to the National Foundation for Infectious Diseases.
Until the approval this summer of the new monoclonal antibody, nirsevimab, there wasn’t a reliable method to prevent infection in most healthy infants.
Both nirsevimab and palivizumab are monoclonal antibodies that act against RSV. Monoclonal antibodies are lab-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses. A single intramuscular injection of nirsevimab preceding or during RSV season may provide protection.
The strategy with the new monoclonal antibody is “to extend protection to healthy infants who nonetheless are at risk because of their age, as well as infants with additional medical risk factors,” said Philippa Gordon, a pediatrician and infectious disease specialist in Brooklyn, New York, and medical adviser to Park Slope Parents, an online community support group.
No specific preventive measure is needed for older and healthier kids because they will develop active immunity, which is more durable. Meanwhile, older adults, who are also vulnerable to RSV, can receive one of two new vaccines. So can pregnant women, who pass on immunity to the fetus, Gordon said.
Until the approval this summer of the new monoclonal antibody, nirsevimab, there wasn’t a reliable method to prevent infection in most healthy infants, “nor is there any treatment other than giving oxygen or supportive care,” said Stanley Spinner, chief medical officer and vice president of Texas Children’s Pediatrics and Texas Children’s Urgent Care.
As with any virus, washing hands frequently and keeping infants and children away from sick people are the best defenses, Duchon said. This approach isn’t foolproof because viruses can run rampant in daycare centers, schools and parents’ workplaces, she added.
Mickayla Wininger, Malcolm’s mother, insists that family and friends wear masks, wash their hands and use hand sanitizer when they’re around her daughter and two sons. She doesn’t allow them to kiss or touch the children. Some people take it personally, but she would rather be safe than sorry.
Wininger recalls the severe anxiety caused by Malcolm's ordeal with RSV. After returning with her infant from his hospital stays, she was terrified to go to sleep. “My fiancé and I would trade shifts, so that someone was watching over our son 24 hours a day,” she said. “I was doing a night shift, so I would take caffeine pills to try and keep myself awake and would end up crashing early hours in the morning and wake up frantically thinking something happened to my son.”
Two years later, her anxiety has become more manageable, and Malcolm is doing well. “He is thriving now,” Wininger said. He recently had his second birthday and "is just the spunkiest boy you will ever meet. He looked death straight in the eyes and fought to be here today.”

Last month, a paper published in Cell by Harvard biologist David Sinclair explored root cause of aging, as well as examining whether this process can be controlled. We talked with Dr. Sinclair about this new research.
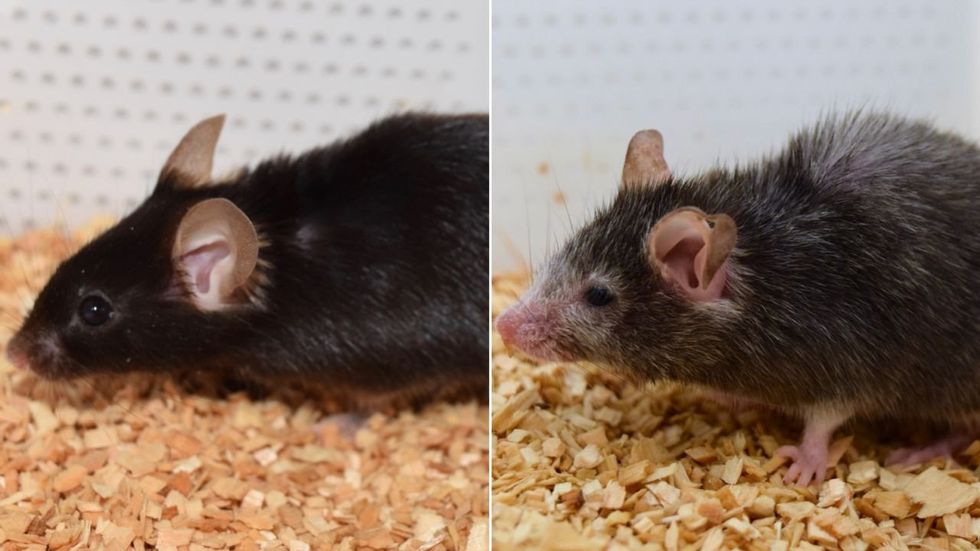
What causes aging? In a paper published last month, Dr. David Sinclair, Professor in the Department of Genetics at Harvard Medical School, reports that he and his co-authors have found the answer. Harnessing this knowledge, Dr. Sinclair was able to reverse this process, making mice younger, according to the study published in the journal Cell.
I talked with Dr. Sinclair about his new study for the latest episode of Making Sense of Science. Turning back the clock on mouse age through what’s called epigenetic reprogramming – and understanding why animals get older in the first place – are key steps toward finding therapies for healthier aging in humans. We also talked about questions that have been raised about the research.
Show links:
Dr. Sinclair's paper, published last month in Cell.
Recent pre-print paper - not yet peer reviewed - showing that mice treated with Yamanaka factors lived longer than the control group.
Dr. Sinclair's podcast.
Previous research on aging and DNA mutations.
Dr. Sinclair's book, Lifespan.

Harvard Medical School
Breakthrough therapies are breaking patients' banks. Key changes could improve access, experts say.

Single-treatment therapies are revolutionizing medicine. But insurers and patients wonder whether they can afford treatment and, if they can, whether the high costs are worthwhile.
CSL Behring’s new gene therapy for hemophilia, Hemgenix, costs $3.5 million for one treatment, but helps the body create substances that allow blood to clot. It appears to be a cure, eliminating the need for other treatments for many years at least.
Likewise, Novartis’s Kymriah mobilizes the body’s immune system to fight B-cell lymphoma, but at a cost $475,000. For patients who respond, it seems to offer years of life without the cancer progressing.
These single-treatment therapies are at the forefront of a new, bold era of medicine. Unfortunately, they also come with new, bold prices that leave insurers and patients wondering whether they can afford treatment and, if they can, whether the high costs are worthwhile.
“Most pharmaceutical leaders are there to improve and save people’s lives,” says Jeremy Levin, chairman and CEO of Ovid Therapeutics, and immediate past chairman of the Biotechnology Innovation Organization. If the therapeutics they develop are too expensive for payers to authorize, patients aren’t helped.
“The right to receive care and the right of pharmaceuticals developers to profit should never be at odds,” Levin stresses. And yet, sometimes they are.
Leigh Turner, executive director of the bioethics program, University of California, Irvine, notes this same tension between drug developers that are “seeking to maximize profits by charging as much as the market will bear for cell and gene therapy products and other medical interventions, and payers trying to control costs while also attempting to provide access to medical products with promising safety and efficacy profiles.”
Why Payers Balk
Health insurers can become skittish around extremely high prices, yet these therapies often accompany significant overall savings. For perspective, the estimated annual treatment cost for hemophilia exceeds $300,000. With Hemgenix, payers would break even after about 12 years.
But, in 12 years, will the patient still have that insurer? Therein lies the rub. U.S. payers, are used to a “pay-as-you-go” model, in which the lifetime costs of therapies typically are shared by multiple payers over many years, as patients change jobs. Single treatment therapeutics eliminate that cost-sharing ability.
"As long as formularies are based on profits to middlemen…Americans’ healthcare costs will continue to skyrocket,” says Patricia Goldsmith, the CEO of CancerCare.
“There is a phenomenally complex, bureaucratic reimbursement system that has grown, layer upon layer, during several decades,” Levin says. As medicine has innovated, payment systems haven’t kept up.
Therefore, biopharma companies begin working with insurance companies and their pharmacy benefit managers (PBMs), which act on an insurer’s behalf to decide which drugs to cover and by how much, early in the drug approval process. Their goal is to make sophisticated new drugs available while still earning a return on their investment.
New Payment Models
Pay-for-performance is one increasingly popular strategy, Turner says. “These models typically link payments to evidence generation and clinically significant outcomes.”
A biotech company called bluebird bio, for example, offers value-based pricing for Zynteglo, a $2.8 million possible cure for the rare blood disorder known as beta thalassaemia. It generally eliminates patients’ need for blood transfusions. The company is so sure it works that it will refund 80 percent of the cost of the therapy if patients need blood transfusions related to that condition within five years of being treated with Zynteglo.
In his February 2023 State of the Union speech, President Biden proposed three pilot programs to reduce drug costs. One of them, the Cell and Gene Therapy Access Model calls on the federal Centers for Medicare & Medicaid Services to establish outcomes-based agreements with manufacturers for certain cell and gene therapies.
A mortgage-style payment system is another, albeit rare, approach. Amortized payments spread the cost of treatments over decades, and let people change employers without losing their healthcare benefits.
Only about 14 percent of all drugs that enter clinical trials are approved by the FDA. Pharma companies, therefore, have an exigent need to earn a profit.
The new payment models that are being discussed aren’t solutions to high prices, says Bill Kramer, senior advisor for health policy at Purchaser Business Group on Health (PBGH), a nonprofit that seeks to lower health care costs. He points out that innovative pricing models, although well-intended, may distract from the real problem of high prices. They are attempts to “soften the blow. The best thing would be to charge a reasonable price to begin with,” he says.
Instead, he proposes making better use of research on cost and clinical effectiveness. The Institute for Clinical and Economic Review (ICER) conducts such research in the U.S., determining whether the benefits of specific drugs justify their proposed prices. ICER is an independent non-profit research institute. Its reports typically assess the degrees of improvement new therapies offer and suggest prices that would reflect that. “Publicizing that data is very important,” Kramer says. “Their results aren’t used to the extent they could and should be.” Pharmaceutical companies tend to price their therapies higher than ICER’s recommendations.
Drug Development Costs Soar
Drug developers have long pointed to the onerous costs of drug development as a reason for high prices.
A 2020 study found the average cost to bring a drug to market exceeded $1.1 billion, while other studies have estimated overall costs as high as $2.6 billion. The development timeframe is about 10 years. That’s because modern therapeutics target precise mechanisms to create better outcomes, but also have high failure rates. Only about 14 percent of all drugs that enter clinical trials are approved by the FDA. Pharma companies, therefore, have an exigent need to earn a profit.
Skewed Incentives Increase Costs
Pricing isn’t solely at the discretion of pharma companies, though. “What patients end up paying has much more to do with their PBMs than the actual price of the drug,” Patricia Goldsmith, CEO, CancerCare, says. Transparency is vital.
PBMs control patients’ access to therapies at three levels, through price negotiations, pricing tiers and pharmacy management.
When negotiating with drug manufacturers, Goldsmith says, “PBMs exchange a preferred spot on a formulary (the insurer’s or healthcare provider’s list of acceptable drugs) for cash-base rebates.” Unfortunately, 25 percent of the time, those rebates are not passed to insurers, according to the PBGH report.
Then, PBMs use pricing tiers to steer patients and physicians to certain drugs. For example, Kramer says, “Sometimes PBMs put a high-cost brand name drug in a preferred tier and a lower-cost competitor in a less preferred, higher-cost tier.” As the PBGH report elaborates, “(PBMs) are incentivized to include the highest-priced drugs…since both manufacturing rebates, as well as the administrative fees they charge…are calculated as a percentage of the drug’s price.
Finally, by steering patients to certain pharmacies, PBMs coordinate patients’ access to treatments, control patients’ out-of-pocket costs and receive management fees from the pharmacies.
Therefore, Goldsmith says, “As long as formularies are based on profits to middlemen…Americans’ healthcare costs will continue to skyrocket.”
Transparency into drug pricing will help curb costs, as will new payment strategies. What will make the most impact, however, may well be the development of a new reimbursement system designed to handle dramatic, breakthrough drugs. As Kramer says, “We need a better system to identify drugs that offer dramatic improvements in clinical care.”