

A future app may help you avoid getting the flu by informing you of your local risk on a given day.
(© Dmytro Flisak/Adobe)
Applied mathematician Sara del Valle works at the U.S.'s foremost nuclear weapons lab: Los Alamos. Once colloquially called Atomic City, it's a hidden place 45 minutes into the mountains northwest of Santa Fe. Here, engineers developed the first atomic bomb.
Like AccuWeather, an app for disease prediction could help people alter their behavior to live better lives.
Today, Los Alamos still a small science town, though no longer a secret, nor in the business of building new bombs. Instead, it's tasked with, among other things, keeping the stockpile of nuclear weapons safe and stable: not exploding when they're not supposed to (yes, please) and exploding if someone presses that red button (please, no).
Del Valle, though, doesn't work on any of that. Los Alamos is also interested in other kinds of booms—like the explosion of a contagious disease that could take down a city. Predicting (and, ideally, preventing) such epidemics is del Valle's passion. She hopes to develop an app that's like AccuWeather for germs: It would tell you your chance of getting the flu, or dengue or Zika, in your city on a given day. And like AccuWeather, it could help people alter their behavior to live better lives, whether that means staying home on a snowy morning or washing their hands on a sickness-heavy commute.

Sara del Valle of Los Alamos is working to predict and prevent epidemics using data and machine learning.
Since the beginning of del Valle's career, she's been driven by one thing: using data and predictions to help people behave practically around pathogens. As a kid, she'd always been good at math, but when she found out she could use it to capture the tentacular spread of disease, and not just manipulate abstractions, she was hooked.
When she made her way to Los Alamos, she started looking at what people were doing during outbreaks. Using social media like Twitter, Google search data, and Wikipedia, the team started to sift for trends. Were people talking about hygiene, like hand-washing? Or about being sick? Were they Googling information about mosquitoes? Searching Wikipedia for symptoms? And how did those things correlate with the spread of disease?
It was a new, faster way to think about how pathogens propagate in the real world. Usually, there's a 10- to 14-day lag in the U.S. between when doctors tap numbers into spreadsheets and when that information becomes public. By then, the world has moved on, and so has the disease—to other villages, other victims.
"We found there was a correlation between actual flu incidents in a community and the number of searches online and the number of tweets online," says del Valle. That was when she first let herself dream about a real-time forecast, not a 10-days-later backcast. Del Valle's group—computer scientists, mathematicians, statisticians, economists, public health professionals, epidemiologists, satellite analysis experts—has continued to work on the problem ever since their first Twitter parsing, in 2011.
They've had their share of outbreaks to track. Looking back at the 2009 swine flu pandemic, they saw people buying face masks and paying attention to the cleanliness of their hands. "People were talking about whether or not they needed to cancel their vacation," she says, and also whether pork products—which have nothing to do with swine flu—were safe to buy.
At the latest meeting with all the prediction groups, del Valle's flu models took first and second place.
They watched internet conversations during the measles outbreak in California. "There's a lot of online discussion about anti-vax sentiment, and people trying to convince people to vaccinate children and vice versa," she says.
Today, they work on predicting the spread of Zika, Chikungunya, and dengue fever, as well as the plain old flu. And according to the CDC, that latter effort is going well.
Since 2015, the CDC has run the Epidemic Prediction Initiative, a competition in which teams like de Valle's submit weekly predictions of how raging the flu will be in particular locations, along with other ailments occasionally. Michael Johannson is co-founder and leader of the program, which began with the Dengue Forecasting Project. Its goal, he says, was to predict when dengue cases would blow up, when previously an area just had a low-level baseline of sick people. "You'll get this massive epidemic where all of a sudden, instead of 3,000 to 4,000 cases, you have 20,000 cases," he says. "They kind of come out of nowhere."
But the "kind of" is key: The outbreaks surely come out of somewhere and, if scientists applied research and data the right way, they could forecast the upswing and perhaps dodge a bomb before it hit big-time. Questions about how big, when, and where are also key to the flu.
A big part of these projects is the CDC giving the right researchers access to the right information, and the structure to both forecast useful public-health outcomes and to compare how well the models are doing. The extra information has been great for the Los Alamos effort. "We don't have to call departments and beg for data," says del Valle.
When data isn't available, "proxies"—things like symptom searches, tweets about empty offices, satellite images showing a green, wet, mosquito-friendly landscape—are helpful: You don't have to rely on anyone's health department.
At the latest meeting with all the prediction groups, del Valle's flu models took first and second place. But del Valle wants more than weekly numbers on a government website; she wants that weather-app-inspired fortune-teller, incorporating the many diseases you could get today, standing right where you are. "That's our dream," she says.

This plot shows the the correlations between the online data stream, from Wikipedia, and various infectious diseases in different countries. The results of del Valle's predictive models are shown in brown, while the actual number of cases or illness rates are shown in blue.
(Courtesy del Valle)
The goal isn't to turn you into a germophobic agoraphobe. It's to make you more aware when you do go out. "If you know it's going to rain today, you're more likely to bring an umbrella," del Valle says. "When you go on vacation, you always look at the weather and make sure you bring the appropriate clothing. If you do the same thing for diseases, you think, 'There's Zika spreading in Sao Paulo, so maybe I should bring even more mosquito repellent and bring more long sleeves and pants.'"
They're not there yet (don't hold your breath, but do stop touching your mouth). She estimates it's at least a decade away, but advances in machine learning could accelerate that hypothetical timeline. "We're doing baby steps," says del Valle, starting with the flu in the U.S., dengue in Brazil, and other efforts in Colombia, Ecuador, and Canada. "Going from there to forecasting all diseases around the globe is a long way," she says.
But even AccuWeather started small: One man began predicting weather for a utility company, then helping ski resorts optimize their snowmaking. His influence snowballed, and now private forecasting apps, including AccuWeather's, populate phones across the planet. The company's progression hasn't been without controversy—privacy incursions, inaccuracy of long-term forecasts, fights with the government—but it has continued, for better and for worse.
Disease apps, perhaps spun out of a small, unlikely team at a nuclear-weapons lab, could grow and breed in a similar way. And both the controversies and public-health benefits that may someday spin out of them lie in the future, impossible to predict with certainty.

The Cocoanut Grove fire in Boston in 1942 tragically claimed 490 lives, but was the catalyst for several important medical advances.
Boston Public Library
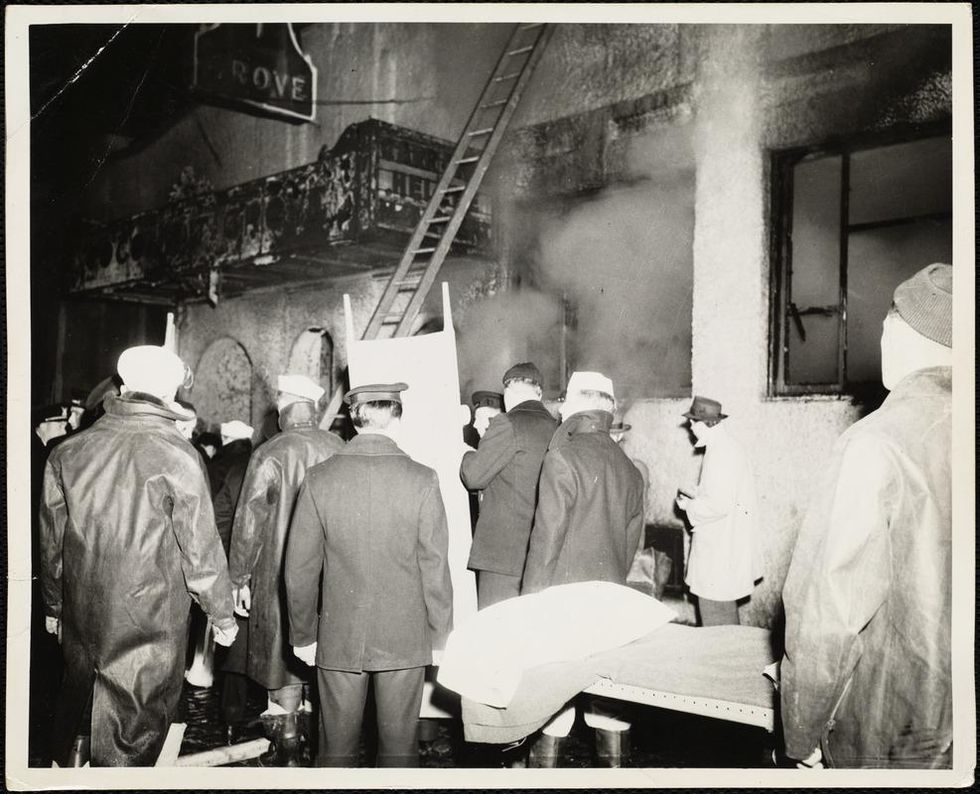
The scene of the fire.
Boston Public Library
Tragic Losses Prompted Revolutionary Leaps
But there is a silver lining: this horrific disaster prompted dramatic changes in safety regulations to prevent another catastrophe of this magnitude and led to the development of medical techniques that eventually saved millions of lives. It transformed burn care treatment and the use of plasma on burn victims, but most importantly, it introduced to the public a new wonder drug that revolutionized medicine, midwifed the birth of the modern pharmaceutical industry, and nearly doubled life expectancy, from 48 years at the turn of the 20th century to 78 years in the post-World War II years.
The devastating grief of the survivors also led to the first published study of post-traumatic stress disorder by pioneering psychiatrist Alexandra Adler, daughter of famed Viennese psychoanalyst Alfred Adler, who was a student of Freud. Dr. Adler studied the anxiety and depression that followed this catastrophe, according to the New York Times, and "later applied her findings to the treatment World War II veterans."
Dr. Ken Marshall is intimately familiar with the lingering psychological trauma of enduring such a disaster. His mother, an Irish immigrant and a nurse in the surgical wards at Boston City Hospital, was on duty that cold Thanksgiving weekend night, and didn't come home for four days. "For years afterward, she'd wake up screaming in the middle of the night," recalls Dr. Marshall, who was four years old at the time. "Seeing all those bodies lined up in neat rows across the City Hospital's parking lot, still in their evening clothes. It was always on her mind and memories of the horrors plagued her for the rest of her life."
The sheer magnitude of casualties prompted overwhelmed physicians to try experimental new procedures that were later successfully used to treat thousands of battlefield casualties. Instead of cutting off blisters and using dyes and tannic acid to treat burned tissues, which can harden the skin, they applied gauze coated with petroleum jelly. Doctors also refined the formula for using plasma--the fluid portion of blood and a medical technology that was just four years old--to replenish bodily liquids that evaporated because of the loss of the protective covering of skin.
"Every war has given us a new medical advance. And penicillin was the great scientific advance of World War II."
"The initial insult with burns is a loss of fluids and patients can die of shock," says Dr. Ken Marshall. "The scientific progress that was made by the two institutions revolutionized fluid management and topical management of burn care forever."
Still, they could not halt the staph infections that kill most burn victims—which prompted the first civilian use of a miracle elixir that was being secretly developed in government-sponsored labs and that ultimately ushered in a new age in therapeutics. Military officials quickly realized this disaster could provide an excellent natural laboratory to test the effectiveness of this drug and see if it could be used to treat the acute traumas of combat in this unfortunate civilian approximation of battlefield conditions. At the time, the very existence of this wondrous medicine—penicillin—was a closely guarded military secret.
From Forgotten Lab Experiment to Wonder Drug
In 1928, Alexander Fleming discovered the curative powers of penicillin, which promised to eradicate infectious pathogens that killed millions every year. But the road to mass producing enough of the highly unstable mold was littered with seemingly unsurmountable obstacles and it remained a forgotten laboratory curiosity for over a decade. But Fleming never gave up and penicillin's eventual rescue from obscurity was a landmark in scientific history.
In 1940, a group at Oxford University, funded in part by the Rockefeller Foundation, isolated enough penicillin to test it on twenty-five mice, which had been infected with lethal doses of streptococci. Its therapeutic effects were miraculous—the untreated mice died within hours, while the treated ones played merrily in their cages, undisturbed. Subsequent tests on a handful of patients, who were brought back from the brink of death, confirmed that penicillin was indeed a wonder drug. But Britain was then being ravaged by the German Luftwaffe during the Blitz, and there were simply no resources to devote to penicillin during the Nazi onslaught.
In June of 1941, two of the Oxford researchers, Howard Florey and Ernst Chain, embarked on a clandestine mission to enlist American aid. Samples of the temperamental mold were stored in their coats. By October, the Roosevelt Administration had recruited four companies—Merck, Squibb, Pfizer and Lederle—to team up in a massive, top-secret development program. Merck, which had more experience with fermentation procedures, swiftly pulled away from the pack and every milligram they produced was zealously hoarded.
After the nightclub fire, the government ordered Merck to dispatch to Boston whatever supplies of penicillin that they could spare and to refine any crude penicillin broth brewing in Merck's fermentation vats. After working in round-the-clock relays over the course of three days, on the evening of December 1st, 1942, a refrigerated truck containing thirty-two liters of injectable penicillin left Merck's Rahway, New Jersey plant. It was accompanied by a convoy of police escorts through four states before arriving in the pre-dawn hours at Massachusetts General Hospital. Dozens of people were rescued from near-certain death in the first public demonstration of the powers of the antibiotic, and the existence of penicillin could no longer be kept secret from inquisitive reporters and an exultant public. The next day, the Boston Globe called it "priceless" and Time magazine dubbed it a "wonder drug."
Within fourteen months, penicillin production escalated exponentially, churning out enough to save the lives of thousands of soldiers, including many from the Normandy invasion. And in October 1945, just weeks after the Japanese surrender ended World War II, Alexander Fleming, Howard Florey and Ernst Chain were awarded the Nobel Prize in medicine. But penicillin didn't just save lives—it helped build some of the most innovative medical and scientific companies in history, including Merck, Pfizer, Glaxo and Sandoz.
"Every war has given us a new medical advance," concludes Marshall. "And penicillin was the great scientific advance of World War II."