


The Dock to Dish model has expanded across North and Central America. Above, artisanal fishermen on the Pacific coast of Costa Rica head out to sea seeking schools of abundant forage fish to supply the program.
In 2012, entrepreneur Sean Barrett founded Dock to Dish in Montauk, New York. It connected local fishermen and women with local chefs, enabling the chefs to serve hyper-fresh seafood – with the caveat that they didn't know what would be on their menus until it arrived in their kitchens the night before.
"Since we're not a seafood-centric culture, people don't know what's what, where fish are from, and when they're in season, making them easy to dupe."
In June of 2017, The United Nations Foundation designated Dock to Dish as one of the top breakthrough innovations that can scale to solve the ocean's grand challenges. His company has since expanded across the Americas and has just opened up shop in Fiji. Leapsmag recently chatted with Barrett about his inspirations and ideas for how to overcome the hurdles of farming wild seafood. This interview has been edited and condensed for clarity.
What inspired you to start Dock to Dish?
The short story is "A Tale of Two Hills."
The first is Quail Hill Farm in Amagansett. I grew up in the commercial fishing port of Chinicock in the 1980's and 90's, working on my family's dock from an early age and in the restaurant industry in my teens. By my thirties, I had accrued my 10,000 hours of experience in both dock and dish. I watched the food system shift from local to global, especially in seafood. By the early 2000's, over 90 percent of seafood in the U.S. was imported. It was bad.
Quail Hill was the first CSA [Community Supported Agriculture, in which customers pay up front for a share in whatever crops grow (or don't) on the farm that season] in the U.S., founded in 1990. So people in the area were accustomed to getting their produce that way. Scott Chaskey, the poet farmer at Quail Hill, really helped crystallize the philosophy for me and inspired me to apply it to seafood. Fishermen had always been bringing a share of their day's catch to their neighbors; now we were just doing it in a more formalized way.
The second is Blue Hill at Stone Barns. [Executive chef and co-owner] Dan Barber literally trademarked the phrase "Know Thy Farmer"; we just expanded it to Know Thy Fisherman and it took off like a rocket ship. His connections in the restaurant world were also indispensable.

17th generation Montauk fisherman Captain Bruce Beckwith (above left) with crew Charlie Etzel (Center) and Jeremy Gould (right).
Do you have any issues that are unique to seafood that a CSA or meat co-op wouldn't face?
This food is WILD. People are totally disconnected from what that word means, and it makes seafood different from everything else. Everything changes when viewed through the prism of that word.
This is the last wild food we eat. It is unpredictable, and subject to variables ranging from currents and tides to which way the wind is blowing. But it is what makes our model so much more impactful and beneficial than the industrialized, demand-driven marketplace that surrounds us. The ocean and its ecosystem are the boss, not chefs and consumers.
There has a been a lot of press about seafood being mislabeled. How and why does that happen? Can Dock to Dish fix it?
Imported, farmed seafood is cheap. Wild, sustainable seafood is not. People are buying low and selling high to make a buck; and while fisheries are extraordinarily regulated, the marketplace isn't. There is no punishment for mislabeling, and no means to correct it. Since we're not a seafood-centric culture, people don't know what's what, where fish are from, and when they're in season, making them easy to dupe. But technology is poised to fix that; DNA testing can test what a fish sample is and where it's from, and SciO handheld spectrometers – soon to be incorporated into smartphones – can analyze the molecular makeup of anything on your plate.
We've created the first ever live tracking system and database for wild fisheries. It is similar to the electronic system used to monitor commercial fisheries, thanks to which the resurgence of wild seafood in U.S. waters is a model for the rest of the world. We have vessel tracking devices on our fishing boats and delivery vans, so the path of each fish is publicly available in real time.
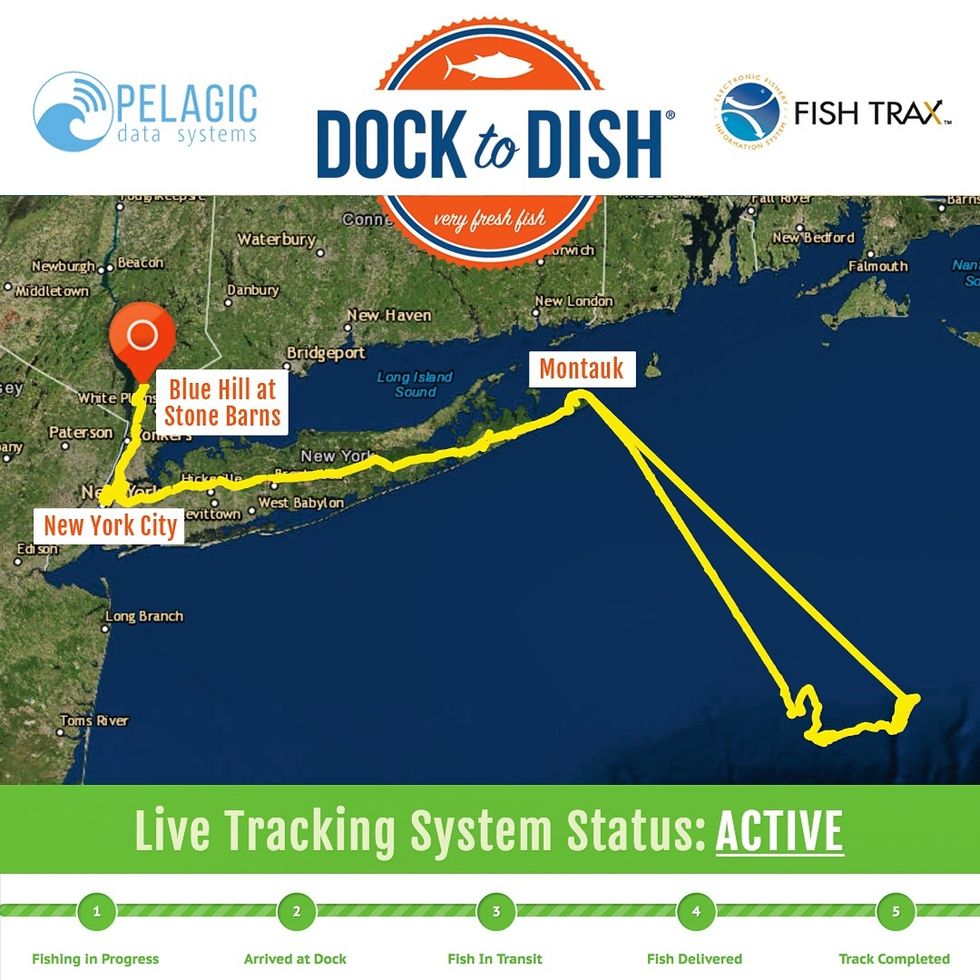
In 2017, Dock to Dish launched the world's first live "end-to-end" tracking system for wild seafood, which provides full chain transparency and next-generation traceability for members.
People are increasingly looking to seafood as a healthier, possibly more sustainable protein option than meat. Can Dock to Dish scale up to accommodate this potentially growing market?
Nope. We can't scale; the supply is finite. That's why the price keeps going up. To avoid becoming "fish for the rich" we are working closely with Greenwave.org to create a network of 3D restorative ocean farms growing kelp and shellfish, which sequester carbon and nitrogen out of the air and soil. Restorative, because sustainable is no longer an option. In fifty years, a plate of seafood will be mostly ocean vegetables with a small amount of finfish as a garnish.

