

Aubrey de Grey at the World Stem Cell Summit in Miami on January 25, 2018.
Aging is not a mystery, says famed researcher Dr. Aubrey de Grey, perhaps the world's foremost advocate of the provocative view that medical technology will one day allow humans to control the aging process and live healthily into our hundreds—or even thousands.
"The cultural attitudes toward all of this are going to be completely turned upside down by sufficiently promising results in the lab, in mice."
He likens aging to a car wearing down over time; as the body operates normally, it accumulates damage which can be tolerated for a while, but eventually sends us into steep decline. The most promising way to escape this biological reality, he says, is to repair the damage as needed with precise scientific tools.
The bad news is that doing this groundbreaking research takes a long time and a lot of money, which has not always been readily available, in part due to a cultural phenomenon he terms "the pro-aging trance." Cultural attitudes have long been fatalistic about the inevitability of aging; many people balk at the seemingly implausible prospect of indefinite longevity.
But the good news for de Grey—and those who are cheering him on—is that his view is becoming less radical these days. Both the academic and private sectors are racing to tackle aging; his own SENS Research Foundation, for one, has spun out into five different companies. Defeating aging, he says, "is not just a future industry; it's an industry now that will be both profitable and extremely good for your health."
De Grey sat down with Editor-in-Chief Kira Peikoff at the World Stem Cell Summit in Miami to give LeapsMag the latest scoop on his work. Here is an edited and condensed version of our conversation.
Since your book Ending Aging was published a decade ago, scientific breakthroughs in stem cell research, genome editing, and other fields have taken the world by storm. Which of these have most affected your research?
They have all affected it a lot in one way, and hardly at all in another way. They have speeded it up--facilitated short cuts, ways to get where we're already trying to go. What they have not done is identified any fundamental changes to the overall strategy. In the book, we described the seven major types of damage, and particular ways of going about fixing each of them, and that hasn't changed.
"Repair at the microscopic level, one would be able to expect to do without surgery, just by injecting the right kind of stem cells."
Has any breakthrough specifically made the biggest impact?
It's not just the obvious things, like iPS (induced pluripotent stem cells) and CRISPR (a precise tool for editing genes). It's also the more esoteric things that applied specifically to certain of our areas, but most people don't really know about them. For example, the identification of how to control something called co-translational mitochondrial protein import.
How much of the future of anti-aging treatments will involve regeneration of old tissue, or wholesale growth of new organs?
The more large-scale ones, regenerating whole new organs, are probably only going to play a role in the short-term and will be phased out relatively rapidly, simply because, in order to be useful, one has to employ surgery, which is really invasive. We'll want to try to get around that, but it seems quite likely that in the very early stages, the techniques we have for repairing things at the molecular and cellular level in situ will be insufficiently comprehensive, and so we will need to do the more sledgehammer approach of building a whole new organ and sticking it in.
Every time you are in a position where you're replacing an organ, you have the option, in principle, of repairing the organ, without replacing it. And repair at the microscopic level, one would be able to expect to do without surgery, just by injecting the right kind of stem cells or whatever. That would be something one would expect to be able to apply to someone much closer to death's door and much more safely in general, and probably much more cheaply. One would expect that subsequent generations of these therapies would move in that direction.
Your foundation is working on an initiative requiring $50 million in funding—
Well, if we had $50 million per year in funding, we could go about three times faster than we are on $5 million per year.
And you're looking at a 2021 timeframe to start human trials?
That's approximate. Remember, because we accumulate in the body so many different types of damage, that means we have many different types of therapy to repair that damage. And of course, each of those types has to be developed independently. It's very much a divide and conquer therapy. The therapies interact with each other to some extent; the repair of one type of damage may slow down the creation of another type of damage, but still that's how it's going to be.
And some of these therapies are much easier to implement than others. The easier components of what we need to do are already in clinical trials—stem cell therapies especially, and immunotherapy against amyloid in the brain, for example. Even in phase III clinical trials in some cases. So when I talk about a timeframe like 2021, or early 20s shall we say, I'm really talking about the most difficult components.
What recent strides are you most excited about?
Looking back over the past couple of years, I'm particularly proud of the successes we've had in the very most difficult areas. If you go through the 7 components of SENS, there are two that have absolutely been stuck in a rut and have gotten nowhere for 15 to 20 years, and we basically fixed that in both cases. We published two years ago in Science magazine that essentially showed a way forward against the stiffening of the extracellular matrix, which is responsible for things like wrinkles and hypertension. And then a year ago, we published a real breakthrough paper with regard to placing copies of the mitochondria DNA in the nuclear DNA modified in such a way that they still work, which is an idea that had been around for 30 years; everyone had given up on it, some a long time ago, and we basically revived it.
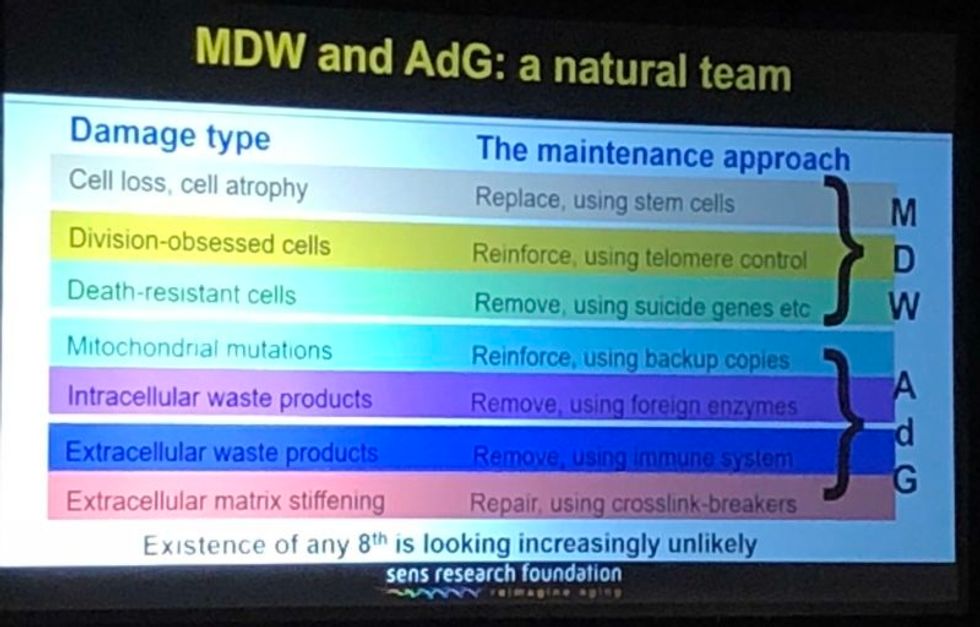
A slide presented by Aubrey de Grey, referencing his collaboration with Mike West at AgeX, showing the 7 types of damage that he believes must be repaired to end aging.
(Courtesy Kira Peikoff)
That's exciting. What do you think are the biggest barriers to defeating aging today: the technological challenges, the regulatory framework, the cost, or the cultural attitude of the "pro-aging" trance?
One can't really address those independently of each other. The technological side is one thing; it's hard, but we know where we're going, we've got a plan. The other ones are very intertwined with each other. A lot of people are inclined to say, the regulatory hurdle will be completely insurmountable, plus people don't recognize aging as a disease, so it's going to be a complete nonstarter. I think that's nonsense. And the reason is because the cultural attitudes toward all of this are going to be completely turned upside down before we have to worry about the regulatory hurdles. In other words, they're going to be turned upside down by sufficiently promising results in the lab, in mice. Once we get to be able to rejuvenate actually old mice really well so they live substantially longer than they otherwise would have done, in a healthy state, everyone's going to know about it and everyone's going to demand – it's not going to be possible to get re-elected unless you have a manifesto commitment to turn the FDA completely upside down and make sure this happens without any kind of regulatory obstacle.
I've been struggling away all these years trying to bring little bits of money in the door, and the reason I have is because of the skepticism as to regards whether this could actually work, combined with the pro-aging trance, which is a product of the skepticism – people not wanting to get their hopes up, so finding excuses about aging being a blessing in disguise, so they don't have to think about it. All of that will literally disintegrate pretty much overnight when we have the right kind of sufficiently impressive progress in the lab. Therefore, the availability of money will also [open up]. It's already cracking: we're already seeing the beginnings of the actual rejuvenation biotechnology industry that I've been talking about with a twinkle in my eye for some years.
"For humans, a 50-50 chance would be twenty years at this point, and there's a 10 percent chance that we won't get there for a hundred years."
Why do you think the culture is starting to shift?
There's no one thing yet. There will be that tipping point I mentioned, perhaps five years from now when we get a real breakthrough, decisive results in mice that make it simply impossible to carry on being fatalistic about all this. Prior to that, what we're already seeing is the impact of sheer old-school repeat advertising—me going out there, banging away and saying the same fucking thing again and again, and nobody saying anything that persuasively knocks me down. … And it's also the fact that we are making incremental amounts of progress, not just ourselves, but the scientific community generally. It has become incrementally more plausible that what I say might be true.
I'm sure you hate getting the timeline question, but if we're five years away from this breakthrough in mice, it's hard to resist asking—how far is that in terms of a human cure?
When I give any kind of timeframes, the only real care I have to take is to emphasize the variance. In this case I think we have got a 50-50 chance of getting to that tipping point in mice within five years from now, certainly it could be 10 or 15 years if we get unlucky. Similarly, for humans, a 50-50 chance would be twenty years at this point, and there's a 10 percent chance that we won't get there for a hundred years.
"I don't get people coming to me saying, well I don't think medicine for the elderly should be done because if it worked it would be a bad thing. People like to ignore this contradiction."
What would you tell skeptical people are the biggest benefits of a very long-lived population?
Any question about the longevity of people is the wrong question. Because the longevity that people fixate about so much will only ever occur as a side effect of health. However long ago you were born or however recently, if you're sick, you're likely to die fairly soon unless we can stop you being sick. Whereas if you're healthy, you're not. So if we do as well as we think we can do in terms of keeping people healthy and youthful however long ago they were born, then the side effect in terms of longevity and life expectancy is likely to be very large. But it's still a side effect, so the way that people actually ought to be—in fact have a requirement to be—thinking, is about whether they want people to be healthy.
Now I don't get people coming to me saying, well I don't think medicine for the elderly should be done because if it worked it would be a bad thing. People like to ignore this contradiction, they like to sweep it under the carpet and say, oh yeah, aging is totally a good thing.
People will never actually admit to the fact that what they are fundamentally saying is medicine for the elderly, if it actually works, would be bad, but still that is what they are saying.
Shifting gears a bit, I'm curious to find out which other radical visionaries in science and tech today you most admire?
Fair question. One is Mike West. I have the great privilege that I now work for him part-time with Age X. I have looked up to him very much for the past ten years, because what he did over the past 20 years starting with Geron is unimaginable today. He was working in an environment where I would not have dreamt of the possibility of getting any private money, any actual investment, in something that far out, that far ahead of its time, and he did it, again and again. It's insane what he managed to do.
What about someone like Elon Musk?
Sure, he's another one. He is totally impervious to the caution and criticism and conservatism that pervades humanity, and he's getting on making these bloody self-driving cars, space tourism, and so on, making them happen. He's thinking just the way I'm thinking really.
"You can just choose how frequently and how thoroughly you repair the damage. And you can make a different choice next time."
You famously said ten years ago that you think the first person to live to 1000 is already alive. Do you think that's still the case?
Definitely, yeah. I can't see how it could not be. Again, it's a probabilistic thing. I said there's at least a 10 percent chance that we won't get to what I call Longevity Escape Velocity for 100 years and if that's true, then the statement about 1000 years being alive already is not going to be the case. But for sure, I believe that the beneficiaries of what we may as well call SENS 1.0, the point where we get to LEV, those people are exceptionally unlikely ever to suffer from any kind of ill health correlated with their age. Because we will never fall below Longevity Escape Velocity once we attain it.
Could someone who was just born today expect—
I would say people in middle age now have a fair chance. Remember – a 50/50 chance of getting to LEV within 20 years, and when you get there, you don't just stay at biologically 70 or 80, you are rejuvenated back to biologically 30 or 40 and you stay there, so your risk of death each year is not related to how long ago you were born, it's the same as a young adult. Today, that's less than 1 in 1000 per year, and that number is going to go down as we get self-driving cars and all that, so actually 1000 is a very conservative number.
So you would be able to choose what age you wanted to go back to?
Oh sure, of course, it's just like a car. What you're doing is you're repairing damage, and the damage is still being created by the body's metabolism, so you can just choose how frequently and how thoroughly you repair the damage. And you can make a different choice next time.
What would be your perfect age?
I have no idea. That's something I don't have an opinion about, because I could change it whenever I like.

Declining numbers of insects, coupled with climate change, can have devastating effects for people in more ways than one. But clever use of technologies like AI could keep them buzzing.
And because many insects serve as food for other species—bats, birds and freshwater fish—they’re an integral part of the ecosystem’s food chain. “If you like to eat good food, you should thank an insect,” says Scott Hoffman Black, an ecologist and executive director of the Xerces Society for Invertebrate Conservation in Portland, Oregon. “And if you like birds in your trees and fish in your streams, you should be concerned with insect conservation.”
Deforestation, urbanization, and agricultural spread have eaten away at large swaths of insect habitat. The increasingly poorly controlled use of insecticides, which harms unintended species, and the proliferation of invasive insect species that disrupt native ecosystems compound the problem.
“There is not a single reason why insects are in decline,” says Jessica L. Ware, associate curator in the Division of Invertebrate Zoology at the American Museum of Natural History in New York, and president of the Entomological Society of America. “There are over one million described insect species, occupying different niches and responding to environmental stressors in different ways.”

Jessica Ware, an entomologist at the American Museum of Natural History, is using DNA methods to monitor insects.
Credit:D.Finnin/AMNH
In addition to habitat loss fueling the decline in insect populations, the other “major drivers” Ware identified are invasive species, climate change, pollution, and fluctuating levels of nitrogen, which play a major role in the lifecycle of plants, some of which serve as insect habitants and others as their food. “The causes of world insect population declines are, unfortunately, very easy to link to human activities,” Lehmann says.
Climate change will undoubtedly make the problem worse. “As temperatures start to rise, it can essentially make it too hot for some insects to survive,” says Emily McDermott, an assistant professor in the Department of Entomology and Plant Pathology at the University of Arkansas. “Conversely in other areas, it could potentially also allow other insects to expand their ranges.”
Without Pollinators Humans Will Starve
We may not think much of our planet’s getting warmer by only one degree Celsius, but it can spell catastrophe for many insects, plants, and animals, because it’s often accompanied by less rainfall. “Changes in precipitation patterns will have cascading consequences across the tree of life,” says David Wagner, a professor of ecology and evolutionary biology at the University of Connecticut. Insects, in particular, are “very vulnerable” because “they’re small and susceptible to drying.”
For instance, droughts have put the monarch butterfly at risk of being unable to find nectar to “recharge its engine” as it migrates from Canada and New England to Mexico for winter, where it enters a hibernation state until it journeys back in the spring. “The monarch is an iconic and a much-loved insect,” whose migration “is imperiled by climate change,” Wagner says.
Warming and drying trends in the Western United States are perhaps having an even more severe impact on insects than in the eastern region. As a result, “we are seeing fewer individual butterflies per year,” says Matt Forister, a professor of insect ecology at the University of Nevada, Reno.
There are hundreds of butterfly species in the United States and thousands in the world. They are pollinators and can serve as good indicators of other species’ health. “Although butterflies are only one group among many important pollinators, in general we assume that what’s bad for butterflies is probably bad for other insects,” says Forister, whose research focuses on butterflies. Climate change and habitat destruction are wreaking havoc on butterflies as well as plants, leading to a further indirect effect on caterpillars and butterflies.
Different insect species have different levels of sensitivity to environmental changes. For example, one-half of the bumblebee species in the United States are showing declines, whereas the other half are not, says Christina Grozinger, a professor of entomology at the Pennsylvania State University. Some species of bumble bees are even increasing in their range, seemingly resilient to environmental changes. But other pollinators are dwindling to the point that farmers have to buy from the rearing facilities, which is the case for the California almond industry. “This is a massive cost to the farmer, which could be provided for free, in case the local habitats supported these pollinators,” Lehmann says.
For bees and other insects, climate change can harm the plants they depend on for survival or have a negative impact on the insects directly. Overly rainy and hot conditions may limit flowering in plants or reduce the ability of a pollinator to forage and feed, which then decreases their reproductive success, resulting in dwindling populations, Grozinger explains.
“Nutritional deprivation can also make pollinators more sensitive to viruses and parasites and therefore cause disease spread,” she says. “There are many ways that climate change can reduce our pollinator populations and make it more difficult to grow the many fruit, vegetable and nut crops that depend on pollinators.”
Disease-Causing Insects Can Bring More Outbreaks
While some much-needed insects are declining, certain disease-causing species may be spreading and proliferating, which is another reason for human concern. Many mosquito types spread malaria, Zika virus, West Nile virus, and a brain infection called equine encephalitis, along with other diseases as well as heartworms in dogs, says Michael Sabourin, president of the Vermont Entomological Society. An animal health specialist for the state, Sabourin conducts vector surveys that identify ticks and mosquitoes.
Scientists refer to disease-carrying insects as vector species and, while there’s a limited number of them, many of these infections can be deadly. Fleas were a well-known vector for the bubonic plague, while kissing bugs are a vector for Chagas disease, a potentially life-threatening parasitic illness in humans, dogs, and other mammals, Sabourin says.
As the planet heats up, some of the creepy crawlers are able to survive milder winters or move up north. Warmer temperatures and a shorter snow season have spawned an increasing abundance of ticks in Maine, including the blacklegged tick (Ixodes scapularis), known to transmit Lyme disease, says Sean Birkel, an assistant professor in the Climate Change Institute and Cooperative Extension at the University of Maine.
Coupled with more frequent and heavier precipitation, rising temperatures bring a longer warm season that can also lead to a longer period of mosquito activity. “While other factors may be at play, climate change affects important underlying conditions that can, in turn, facilitate the spread of vector-borne disease,” Birkel says.
For example, if mosquitoes are finding fewer of their preferred food sources, they may bite humans more. Both male and female mosquitoes feed on sugar as part of their normal behavior, but if they aren’t eating their fill, they may become more bloodthirsty. One recent paper found that sugar-deprived Anopheles gambiae females go for larger blood meals to stay in good health and lay eggs. “More blood meals equals more chances to pick up and transmit a pathogen,” McDermott says, He adds that climate change could reduce the number of available plants to feed on. And while most mosquitoes are “generalist sugar-feeders” meaning that they will likely find alternatives, losing their favorite plants can make them hungrier for blood.
Similar to the effect of losing plants, mosquitoes may get turned onto people if they lose their favorite animal species. For example, some studies found that Culex pipiens mosquitoes that transmit the West Nile virus feed primarily on birds in summer. But that changes in the fall, at least in some places. Because there are fewer birds around, C. pipiens switch to mammals, including humans. And if some disease-carrying insect species proliferate or increase their ranges, that increases chances for human infection, says McDermott. “A larger concern is that climate change could increase vector population sizes, making it more likely that people or animals would be bitten by an infected insect.”
Science Can Help Bring Back the Buzz
To help friendly insects thrive and keep the foes in check, scientists need better ways of trapping, counting, and monitoring insects. It’s not an easy job, but artificial intelligence and molecular methods can help. Ware’s lab uses various environmental DNA methods to monitor freshwater habitats. Molecular technologies hold much promise. The so-called DNA barcodes, in which species are identified using a short string of their genes, can now be used to identify birds, bees, moths and other creatures, and should be used on a larger scale, says Wagner, the University of Connecticut professor. “One day, something akin to Star Trek’s tricorder will soon be on sale down at the local science store.”
Scientists are also deploying artificial intelligence, or AI, to identify insects in agricultural systems and north latitudes where there are fewer bugs, Wagner says. For instance, some automated traps already use the wingbeat frequencies of mosquitoes to distinguish the harmless ones from the disease-carriers. But new technology and software are needed to further expand detection based on vision, sound, and odors.
“Because of their ubiquity, enormity of numbers, and seemingly boundless diversity, we desperately need to develop molecular and AI technologies that will allow us to automate sampling and identification,” says Wagner. “That would accelerate our ability to track insect populations, alert us to the presence of new disease vectors, exotic pest introductions, and unexpected declines.”

Certain gases used for anesthesia are 3,000 times more damaging for the climate than CO2. Some anesthesiologists are pointing to other solutions.
On the whole, the medical sector is responsible for a disproportionally large percentage of greenhouse gas emissions, with the U.S. as the biggest culprit. According to a key paper published in 2020 in Health Affairs, the health industry “is among the most carbon-intensive service sectors in the industrialized world,” accounting for between 4.4 percent and 4.6 percent of greenhouse gas emissions. “It’s not just anesthesia but health care that has a problem,” says Jodi Sherman, anesthesiology professor and Medical Director of the Program on Healthcare Environmental Sustainability at Yale University as well as co-director of the Lancet Planetary Health Commission on Sustainable Healthcare. In the U.S., health care greenhouse gas emissions make up about 8.5 percent of domestic greenhouse gas emissions. They rose 6 percent from 2010 to 2018, to nearly 1,700 kilograms per person, more than in any other nation.
Of course, patients worry primarily about safety, not sustainability. Yet, Koch emphasizes that “as doctors, we have the responsibility to do no harm, and this includes making sure that we use resources as sustainably as possible.” Studies show that 2018 greenhouse gas and toxic air pollutant emissions resulted in the loss of 388,000 disability-adjusted life years in the U.S. alone. “Disease burden from health care pollution is of the same order of magnitude as deaths from preventable medical errors, and should be taken just as seriously,” Sherman cautions.
When Koch, the anesthesiologist, started discussing sustainable options with colleagues, the topic was immediately met with plenty of interest. Her experience is consistent with the latest representative poll of the nonprofit Foundation Health in Germany. Nine out of ten doctors were interested in urgently finding sustainable solutions for medical services but lacked knowhow and resources. For teaching purposes, Sherman and her team have developed the Yale Gassing Greener app that allows anesthesiologists to compare how much pollution they can avoid through choosing different anesthesia methods. Sherman also published professional guidelines intended to help her colleagues better understand how various methods affect carbon emissions.
Significant traces of inhalation gases have been found in Antarctica and the Himalayas, far from the vast majority of surgery rooms.
A solution espoused by both Sherman and Koch is comparatively simple: They stopped using desflurane, which is by far the most damaging of all inhalation gases to the climate. Its greenhouse effect is 2,590 times stronger than carbon dioxide. The Yale New Haven Hospital already stopped using desflurane in 2013, becoming the first known healthcare organization to eliminate a drug based on environmental grounds. Sherman points out that this resulted in saving more than $1.2 million in costs and 1,600 tons of CO2 equivalents, about the same as the exhaust from 360 passenger vehicles per year.
At the Charité, Koch claims that switching to other anesthesiology choices, such as propofol, has eliminated 90 percent of the climate gas emissions in the anesthesiology department since 2016. Young anesthesiologists are still taught to use desflurane as the standard because desflurane is absorbed less into the patients’ bodies, and they wake up faster. However, Koch who has worked as an anesthesiologist since 2006, says that with a little bit of experience, you can learn when to stop giving the propofol so it's timed just as well with a person’s wake-up process. In addition, “patients are less likely to feel nauseous after being given propofol,” Koch says. Intravenous drugs might require more skill, she adds, "but there is nothing unique to the drug desflurane that cannot be accomplished with other medications.”
Desflurane isn’t the only gas to be concerned about. Nitrous oxide is the second most damaging because it’s extremely long-lived in the environment, and it depletes the ozone layer. Climate-conscious anesthesiologists are phasing out this gas, too, or have implemented measures to decrease leaks.
Internationally, 192 governments agreed in the Kyoto protocol of 2005 to reduce halogenated hydrocarbons – resulting from inhalation gases, including desflurane and nitrous oxide – because of their immense climate-warming potential, and in 2016, they pledged to eliminate them by 2035. However, the use of inhalation anesthetics continues to increase worldwide, not least because more people access healthcare in developing countries, and because people in industrialized countries live longer and therefore need more surgeries. Significant traces of inhalation gases have been found in Antarctica and the Himalayas, far from the vast majority of surgery rooms.
Certain companies are now pushing new technology to capture inhalation gases before they are released into the atmosphere, but both Sherman and Koch believe marketing claims of 99 percent efficiency amount to greenwashing. After investigating the technology first-hand and visiting the company that is producing such filters in Germany, Koch concluded that such technology only reduces emissions by 25 percent. And Sherman believes such initiatives are akin to the fallacy of recycling plastic. In addition to questioning their efficiency, Sherman fears such technology “gives the illusion there is a magical solution that means I don’t need to change my behavior, reduce my waste and choose less harmful options.”
Financial interests are at play, too. “Desflurane is the most expensive inhalation gas, and some think, the most expensive must be the best,” Koch says. Both Koch and Sherman lament that efforts to increase sustainability in the medical sector are entirely voluntary in their countries and led by a few dedicated individual professionals while industry-wide standards and transparency are needed, a notion expressed in the American Hospital Association’s Sustainability Roadmap.

Susanne Koch, an anesthesiologist in Berlin, wants her colleagues to stop using a gas called desflurane, which is by far the most damaging of all inhalation gases to the climate.
Adobe Stock
Other countries have done more. The European Union recommends reducing inhalation gases and even contemplated a ban of desflurane, except in medical emergencies. In 2008, the National Health Service (NHS) created a Sustainable Development Unit, which measures CO2 emissions in the U.K. health sector. NHS is the first national health service that pledged to reach net zero carbon by 2040. The carbon footprint of the NHS fell by 26 percent from 1990 to 2019, mostly due to reduced use of certain inhalers and the switch to renewable energy for heat and power. “The evidence that the climate emergency is a health emergency is overwhelming,” said Nick Watts, the NHS Chief Sustainability Officer, in a press release, “with health professionals already needing to manage its symptoms.”
Sherman is a leading voice in demanding action in the U.S. To her, comprehensive solutions start with the mandatory, transparent measurement of emissions in the health sector to tackle the biggest sources of pollution. While the Biden administration highlighted its efforts to reduce these kinds of emissions during the United Nations Climate Conference (COP27) in November 2022 and U.S. delegates announced that more than 100 health care organizations signed the voluntary Health Sector Climate Pledge, with the aim to reduce emissions by 50 percent in the next eight years, Sherman is convinced that voluntary pledges are not enough. “Voluntary measures are insufficient,” she testified in congress. “The vast majority of U.S. health care organizations remain uncommitted to timely action. Those that are committed lack policies and knowledge to support necessary changes; even worse, existing policies drive inappropriate consumption of resources and pollution.”
Both Sherman and Koch look at the larger picture. “Health care organizations have an obligation to their communities to protect public health,” Sherman says. “We must lead by example. That includes setting ambitious, science-based carbon reduction targets to achieve net zero emissions before 2050. We must quantify current emissions and their sources, particularly throughout the health care supply chains.”