

The Cocoanut Grove fire in Boston in 1942 tragically claimed 490 lives, but was the catalyst for several important medical advances.
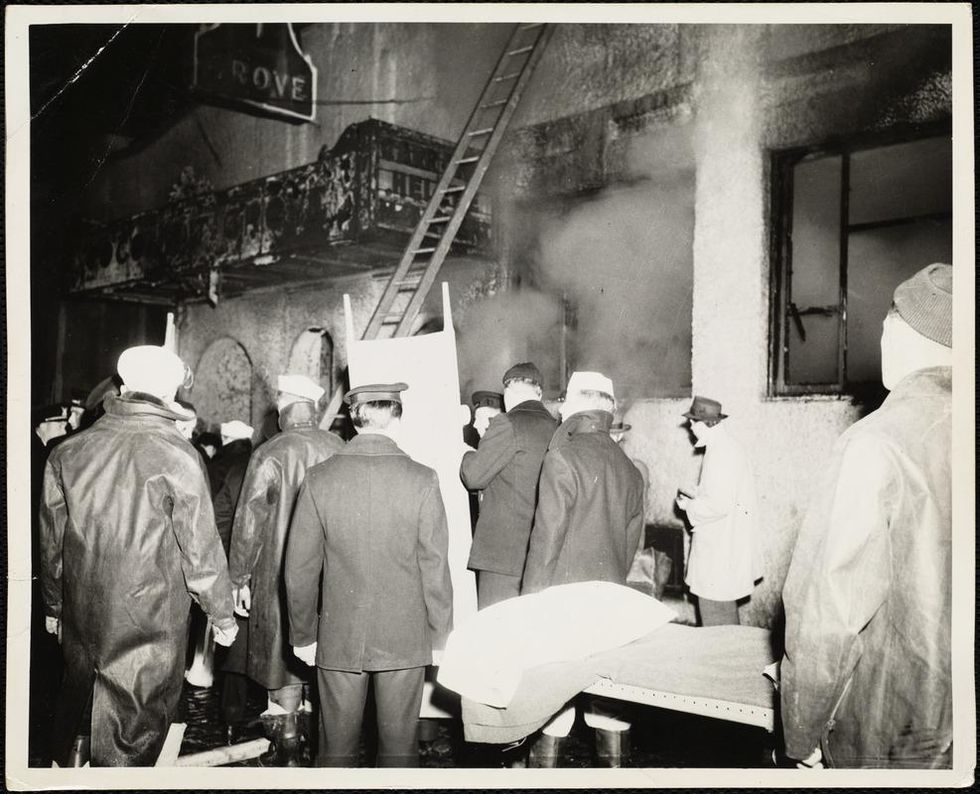
The scene of the fire.
Boston Public Library
Tragic Losses Prompted Revolutionary Leaps
But there is a silver lining: this horrific disaster prompted dramatic changes in safety regulations to prevent another catastrophe of this magnitude and led to the development of medical techniques that eventually saved millions of lives. It transformed burn care treatment and the use of plasma on burn victims, but most importantly, it introduced to the public a new wonder drug that revolutionized medicine, midwifed the birth of the modern pharmaceutical industry, and nearly doubled life expectancy, from 48 years at the turn of the 20th century to 78 years in the post-World War II years.
The devastating grief of the survivors also led to the first published study of post-traumatic stress disorder by pioneering psychiatrist Alexandra Adler, daughter of famed Viennese psychoanalyst Alfred Adler, who was a student of Freud. Dr. Adler studied the anxiety and depression that followed this catastrophe, according to the New York Times, and "later applied her findings to the treatment World War II veterans."
Dr. Ken Marshall is intimately familiar with the lingering psychological trauma of enduring such a disaster. His mother, an Irish immigrant and a nurse in the surgical wards at Boston City Hospital, was on duty that cold Thanksgiving weekend night, and didn't come home for four days. "For years afterward, she'd wake up screaming in the middle of the night," recalls Dr. Marshall, who was four years old at the time. "Seeing all those bodies lined up in neat rows across the City Hospital's parking lot, still in their evening clothes. It was always on her mind and memories of the horrors plagued her for the rest of her life."
The sheer magnitude of casualties prompted overwhelmed physicians to try experimental new procedures that were later successfully used to treat thousands of battlefield casualties. Instead of cutting off blisters and using dyes and tannic acid to treat burned tissues, which can harden the skin, they applied gauze coated with petroleum jelly. Doctors also refined the formula for using plasma--the fluid portion of blood and a medical technology that was just four years old--to replenish bodily liquids that evaporated because of the loss of the protective covering of skin.
"Every war has given us a new medical advance. And penicillin was the great scientific advance of World War II."
"The initial insult with burns is a loss of fluids and patients can die of shock," says Dr. Ken Marshall. "The scientific progress that was made by the two institutions revolutionized fluid management and topical management of burn care forever."
Still, they could not halt the staph infections that kill most burn victims—which prompted the first civilian use of a miracle elixir that was being secretly developed in government-sponsored labs and that ultimately ushered in a new age in therapeutics. Military officials quickly realized this disaster could provide an excellent natural laboratory to test the effectiveness of this drug and see if it could be used to treat the acute traumas of combat in this unfortunate civilian approximation of battlefield conditions. At the time, the very existence of this wondrous medicine—penicillin—was a closely guarded military secret.
From Forgotten Lab Experiment to Wonder Drug
In 1928, Alexander Fleming discovered the curative powers of penicillin, which promised to eradicate infectious pathogens that killed millions every year. But the road to mass producing enough of the highly unstable mold was littered with seemingly unsurmountable obstacles and it remained a forgotten laboratory curiosity for over a decade. But Fleming never gave up and penicillin's eventual rescue from obscurity was a landmark in scientific history.
In 1940, a group at Oxford University, funded in part by the Rockefeller Foundation, isolated enough penicillin to test it on twenty-five mice, which had been infected with lethal doses of streptococci. Its therapeutic effects were miraculous—the untreated mice died within hours, while the treated ones played merrily in their cages, undisturbed. Subsequent tests on a handful of patients, who were brought back from the brink of death, confirmed that penicillin was indeed a wonder drug. But Britain was then being ravaged by the German Luftwaffe during the Blitz, and there were simply no resources to devote to penicillin during the Nazi onslaught.
In June of 1941, two of the Oxford researchers, Howard Florey and Ernst Chain, embarked on a clandestine mission to enlist American aid. Samples of the temperamental mold were stored in their coats. By October, the Roosevelt Administration had recruited four companies—Merck, Squibb, Pfizer and Lederle—to team up in a massive, top-secret development program. Merck, which had more experience with fermentation procedures, swiftly pulled away from the pack and every milligram they produced was zealously hoarded.
After the nightclub fire, the government ordered Merck to dispatch to Boston whatever supplies of penicillin that they could spare and to refine any crude penicillin broth brewing in Merck's fermentation vats. After working in round-the-clock relays over the course of three days, on the evening of December 1st, 1942, a refrigerated truck containing thirty-two liters of injectable penicillin left Merck's Rahway, New Jersey plant. It was accompanied by a convoy of police escorts through four states before arriving in the pre-dawn hours at Massachusetts General Hospital. Dozens of people were rescued from near-certain death in the first public demonstration of the powers of the antibiotic, and the existence of penicillin could no longer be kept secret from inquisitive reporters and an exultant public. The next day, the Boston Globe called it "priceless" and Time magazine dubbed it a "wonder drug."
Within fourteen months, penicillin production escalated exponentially, churning out enough to save the lives of thousands of soldiers, including many from the Normandy invasion. And in October 1945, just weeks after the Japanese surrender ended World War II, Alexander Fleming, Howard Florey and Ernst Chain were awarded the Nobel Prize in medicine. But penicillin didn't just save lives—it helped build some of the most innovative medical and scientific companies in history, including Merck, Pfizer, Glaxo and Sandoz.
"Every war has given us a new medical advance," concludes Marshall. "And penicillin was the great scientific advance of World War II."


Recent immigration restrictions have left many foreign researchers' projects and careers in limbo—and some in jeopardy.
"I spent about $4,000 on lawyer fees and another $1,200 to pay for the motions I filed," she recalls. "I had to borrow money from my parents and my cousin because without my salary I just didn't have the $7,000 at hand." But the already narrow window of opportunity slammed completely shut when the Trump administration suspended issuing new visas for foreign researchers in June. All Mohan's attempts were denied. In August, she had to leave the country. "Given the recent work visa ban by the administration, all my options in the U.S. are closed," she wrote a bitter note on Twitter. "I have to uproot my entire life in NY for the past 6 years and leave." She eventually found a temporary position in Calcutta, where she can continue research.
Mohan is hardly alone in her visa saga. Many foreign scholars on H- and J-type visas and other permits that let them remain employed in America had been struggling to keep their rights to continue research, which in certain cases is crucial to battling the pandemic. Some had to leave the country, some filed every possible extension to buy time, and others are stuck in their home countries, unable to return. The already cumbersome process of applying for visas and extensions became crippled during the lockdowns. But in June, when President Trump extended and expanded immigration restrictions to cut the number of immigrant workers entering the U.S., the new limits left researchers' projects and careers in limbo—and some in jeopardy.
"We have been a beneficiary of this flow of human capacity and resource investment for many generations—and this is now threatened."
Rakesh Ramachandran, whose computational biology work contributed to one of the first coronavirus studies to map out its protein structures—is stranded in India. In early March, he had travelled there to attend a conference and visit the American consulate to stamp his H1 visa for a renewal, already granted. The pandemic shut down both the conference and the consulates, and Ramachandran hasn't been able to come back since. The consulates finally opened in September, but so far the online portal has no available appointment slots. "I'm told to keep trying," Ramachandran says.
The visa restrictions affected researchers worldwide, regardless of disciplines or countries. A Ph.D. student in neuroscience, Morgane Leroux had to do her experiments with mice at Gladstone Institutes in America and analyze the data back home at Sorbonne University in France. She had finished her first round of experiments when the lockdowns forced her to return to Paris, and she hasn't been able to come back to resume her work since. "I can't continue the experiments, which is really frustrating," she says, especially because she doesn't know what it means for her Ph.D. "I may have to entirely change my subject," she says, which she doesn't want to do—it would be a waste of time and money.
But besides wreaking havoc in scholars' personal lives and careers, the visa restrictions had—and will continue to have—tremendous deleterious effects on America's research and its global scientific competitiveness. "It's incredibly short-sighted and self-destructing to restrict the immigration of scientists into the U.S.," says Benjamin G. Neel, who directs the Laura and Isaac Perlmutter Cancer Center at New York University. "If they can't come here, they will go elsewhere," he says, causing a brain drain.

Neel in his lab with postdocs
(Courtesy of Neel)
Neel felt the outcomes of the shortsighted policies firsthand. In the past few months, his lab lost two postdoctoral researchers who had made major strides in understanding the biology of several particularly stubborn, treatment-resistant malignancies. One postdoc studied the underlying mechanisms responsible for 90 percent of pancreatic cancers and half of the colon ones. The other one devised a new system of modeling ovarian cancer in mice to test new therapeutic drug combinations for the deadliest tumor types—but had to return home to China.
"By working around the clock, she was able to get her paper accepted, but she hasn't been able to train us to use this new system, which can set us back six months," Neel says.
Her discoveries also helped the lab secure about $900,000 in grants for new research. Losing people like this is "literally killing the goose that lays the golden eggs," Neel adds. "If you want to make America poor again, this is the way to do it."
Cassidy R. Sugimoto at Indiana University Bloomington, who studies how scientific knowledge is produced and disseminated, says that scientists are the most productive when they are free to move, exchange ideas, and work at labs with the best equipment. Restricting that freedom reduces their achievement.
"Several empirical studied demonstrated the benefits to the U.S. by attracting and retaining foreign scientists. The disproportional number of our Nobel Prize winners were not only foreign-born but also foreign-educated," she says. Scientific advancement bolsters the country's economic prowess, too, so turning scholars away is bad for the economy long-term. "We have been a beneficiary of this flow of human capacity and resource investment for many generations—and this is now threatened," Sugimoto adds—because scientists will look elsewhere. "We are seeing them shifting to other countries that are more hospitable, both ideologically and in terms of health security. Many visiting scholars, postdocs, and graduate students who would otherwise come to the United States are now moving to Canada."
It's not only the Ph.D. students and postdocs who are affected. In some cases, even well-established professors who have already made their marks in the field and direct their own labs at prestigious research institutions may have to pack up and leave the country in the next few months. One scientist who directs a prominent neuroscience lab is betting on his visa renewal and a green card application, but if that's denied, the entire lab may be in jeopardy, as many grants hinge on his ability to stay employed in America.
"It's devastating to even think that it can happen," he says—after years of efforts invested. "I can't even comprehend how it would feel. It would be terrifying and really sad." (He asked to withhold his name for fear that it may adversely affect his applications.) Another scientist who originally shared her story for this article, later changed her mind and withdrew, worrying that speaking out may hurt the entire project, a high-profile COVID-19 effort. It's not how things should work in a democratic country, scientists admit, but that's the reality.
Still, some foreign scholars are speaking up. Mehmet Doğan, a physicist at University of California Berkeley who has been fighting a visa extension battle all year, says it's important to push back in an organized fashion with petitions and engage legislators. "This administration was very creative in finding subtle and not so subtle ways to make our lives more difficult," Doğan says. He adds that the newest rules, proposed by the Department of Homeland Security on September 24, could further limit the time scholars can stay, forcing them into continuous extension battles. That's why the upcoming election might be a turning point for foreign academics. "This election will decide if many of us will see the U.S. as the place to stay and work or whether we look at other countries," Doğan says, echoing the worries of Neel, Sugimoto, and others in academia.

Dogan on Zoom talking to his fellow union members of the Academic Researchers United, a union of almost 5,000 Academic Researchers.
(Credit: Ceyda Durmaz Dogan)
If this year has shown us anything, it is that viruses and pandemics know no borders as they sweep across the globe. Likewise, science can't be restrained by borders either. "Science is an international endeavor," says Neel—and right now humankind now needs unified scientific research more than ever, unhindered by immigration hurdles and visa wars. Humanity's wellbeing in America and beyond depends on it.
[Editor's Note: To read other articles in this special magazine issue, visit the beautifully designed e-reader version.]