

In the U.S., hospitals generate an estimated 6,000 tons of waste per day. A few clinics are leading the way in transitioning to clean energy sources.
This is part 2 of a three part series on a new generation of doctors leading the charge to make the health care industry more sustainable - for the benefit of their patients and the planet. Read part 1 here and part 3 here.
After graduating from her studies as an engineer, Nora Stroetzel ticked off the top item on her bucket list and traveled the world for a year. She loved remote places like the Indonesian rain forest she reached only by hiking for several days on foot, mountain villages in the Himalayas, and diving at reefs that were only accessible by local fishing boats.
“But no matter how far from civilization I ventured, one thing was already there: plastic,” Stroetzel says. “Plastic that would stay there for centuries, on 12,000 foot peaks and on beaches several hundred miles from the nearest city.” She saw “wild orangutans that could be lured by rustling plastic and hermit crabs that used plastic lids as dwellings instead of shells.”
While traveling she started volunteering for beach cleanups and helped build a recycling station in Indonesia. But the pivotal moment for her came after she returned to her hometown Kiel in Germany. “At the dentist, they gave me a plastic cup to rinse my mouth. I used it for maybe ten seconds before it was tossed out,” Stroetzel says. “That made me really angry.”
She decided to research alternatives for plastic in the medical sector and learned that cups could be reused and easily disinfected. All dentists routinely disinfect their tools anyway and, Stroetzel reasoned, it wouldn’t be too hard to extend that practice to cups.
It's a good example for how often plastic is used unnecessarily in medical practice, she says. The health care sector is the fifth biggest source of pollution and trash in industrialized countries. In the U.S., hospitals generate an estimated 6,000 tons of waste per day, including an average of 400 grams of plastic per patient per day, and this sector produces 8.5 percent of greenhouse gas emissions nationwide.
“Sustainable alternatives exist,” Stroetzel says, “but you have to painstakingly look for them; they are often not offered by the big manufacturers, and all of this takes way too much time [that] medical staff simply does not have during their hectic days.”
When Stroetzel spoke with medical staff in Germany, she found they were often frustrated by all of this waste, especially as they took care to avoid single-use plastic at home. Doctors in other countries share this frustration. In a recent poll, nine out of ten doctors in Germany said they’re aware of the urgency to find sustainable solutions in the health industry but don’t know how to achieve this goal.
After a year of researching more sustainable alternatives, Stroetzel founded a social enterprise startup called POP, short for Practice Without Plastic, together with IT expert Nicolai Niethe, to offer well-researched solutions. “Sustainable alternatives exist,” she says, “but you have to painstakingly look for them; they are often not offered by the big manufacturers, and all of this takes way too much time [that] medical staff simply does not have during their hectic days.”
In addition to reusable dentist cups, other good options for the heath care sector include washable N95 face masks and gloves made from nitrile, which waste less water and energy in their production. But Stroetzel admits that truly making a medical facility more sustainable is a complex task. “This includes negotiating with manufacturers who often package medical materials in double and triple layers of extra plastic.”
While initiatives such as Stroetzel’s provide much needed information, other experts reason that a wholesale rethinking of healthcare is needed. Voluntary action won’t be enough, and government should set the right example. Kari Nadeau, a Stanford physician who has spent 30 years researching the effects of environmental pollution on the immune system, and Kenneth Kizer, the former undersecretary for health in the U.S. Department of Veterans Affairs, wrote in JAMA last year that the medical industry and federal agencies that provide health care should be required to measure and make public their carbon footprints. “Government health systems do not disclose these data (and very rarely do private health care organizations), unlike more than 90% of the Standard & Poor’s top 500 companies and many nongovernment entities," they explained. "This could constitute a substantial step toward better equipping health professionals to confront climate change and other planetary health problems.”
Compared to the U.K., the U.S. healthcare industry lags behind in terms of measuring and managing its carbon footprint, and hospitals are the second highest energy user of any sector in the U.S.
Kizer and Nadeau look to the U.K. National Health Service (NHS), which created a Sustainable Development Unit in 2008 and began that year to conduct assessments of the NHS’s carbon footprint. The NHS also identified its biggest culprits: Of the 2019 footprint, with emissions totaling 25 megatons of carbon dioxide equivalent, 62 percent came from the supply chain, 24 percent from the direct delivery of care, 10 percent from staff commute and patient and visitor travel, and 4 percent from private health and care services commissioned by the NHS. From 1990 to 2019, the NHS has reduced its emission of carbon dioxide equivalents by 26 percent, mostly due to the switch to renewable energy for heat and power. Meanwhile, the NHS has encouraged health clinics in the U.K. to install wind generators or photovoltaics that convert light to electricity -- relatively quick ways to decarbonize buildings in the health sector.
Compared to the U.K., the U.S. healthcare industry lags behind in terms of measuring and managing its carbon footprint, and hospitals are the second highest energy user of any sector in the U.S. “We are already seeing patients with symptoms from climate change, such as worsened respiratory symptoms from increased wildfires and poor air quality in California,” write Thomas B. Newman, a pediatrist at the University of California, San Francisco, and UCSF clinical research coordinator Daisy Valdivieso. “Because of the enormous health threat posed by climate change, health professionals should mobilize support for climate mitigation and adaptation efforts.” They believe “the most direct place to start is to approach the low-lying fruit: reducing healthcare waste and overuse.”
In addition to resulting in waste, the plastic in hospitals ultimately harms patients, who may be even more vulnerable to the effects due to their health conditions. Microplastics have been detected in most humans, and on average, a human ingests five grams of microplastic per week. Newman and Valdivieso refer to the American Board of Internal Medicine's Choosing Wisely program as one of many initiatives that identify and publicize options for “safely doing less” as a strategy to reduce unnecessary healthcare practices, and in turn, reduce cost, resource use, and ultimately reduce medical harm.
A few U.S. clinics are pioneers in transitioning to clean energy sources. In Wisconsin, the nonprofit Gundersen Health network became the first hospital to cut its reliance on petroleum by switching to locally produced green energy in 2015, and it saved $1.2 million per year in the process. Kaiser Permanente eliminated its 800,000 ton carbon footprint through energy efficiency and purchasing carbon offsets, reaching a balance between carbon emissions and removing carbon from the atmosphere in 2020, the first U.S. health system to do so.
Cleveland Clinic has pledged to join Kaiser in becoming carbon neutral by 2027. Realizing that 80 percent of its 2008 carbon emissions came from electricity consumption, the Clinic started switching to renewable energy and installing solar panels, and it has invested in researching recyclable products and packaging. The Clinic’s sustainability report outlines several strategies for producing less waste, such as reusing cases for sterilizing instruments, cutting back on materials that can’t be recycled, and putting pressure on vendors to reduce product packaging.
The Charité Berlin, Europe’s biggest university hospital, has also announced its goal to become carbon neutral. Its sustainability managers have begun to identify the biggest carbon culprits in its operations. “We’ve already reduced CO2 emissions by 21 percent since 2016,” says Simon Batt-Nauerz, the director of infrastructure and sustainability.
The hospital still emits 100,000 tons of CO2 every year, as much as a city with 10,000 residents, but it’s making progress through ride share and bicycle programs for its staff of 20,000 employees, who can get their bikes repaired for free in one of the Charité-operated bike workshops. Another program targets doctors’ and nurses’ scrubs, which cause more than 200 tons of CO2 during manufacturing and cleaning. The staff is currently testing lighter, more sustainable scrubs made from recycled cellulose that is grown regionally and requires 80 percent less land use and 30 percent less water.

The Charité hospital in Berlin still emits 100,000 tons of CO2 every year, but it’s making progress through ride share and bicycle programs for its staff of 20,000 employees.
Wiebke Peitz | Specific to Charité
Anesthesiologist Susanne Koch spearheads sustainability efforts in anesthesiology at the Charité. She says that up to a third of hospital waste comes from surgery rooms. To reduce medical waste, she recommends what she calls the 5 Rs: Reduce, Reuse, Recycle, Rethink, Research. “In medicine, people don’t question the use of plastic because of safety concerns,” she says. “Nobody wants to be sued because something is reused. However, it is possible to reduce plastic and other materials safely.”
For instance, she says, typical surgery kits are single-use and contain more supplies than are actually needed, and the entire kit is routinely thrown out after the surgery. “Up to 20 percent of materials in a surgery room aren’t used but will be discarded,” Koch says. One solution could be smaller kits, she explains, and another would be to recycle the plastic. Another example is breathing tubes. “When they became scarce during the pandemic, studies showed that they can be used seven days instead of 24 hours without increased bacteria load when we change the filters regularly,” Koch says, and wonders, “What else can we reuse?”
In the Netherlands, TU Delft researchers Tim Horeman and Bart van Straten designed a method to melt down the blue polypropylene wrapping paper that keeps medical instruments sterile, so that the material can be turned it into new medical devices. Currently, more than a million kilos of the blue paper are used in Dutch hospitals every year. A growing number of Dutch hospitals are adopting this approach.
Another common practice that’s ripe for improvement is the use of a certain plastic, called PVC, in hospital equipment such as blood bags, tubes and masks. Because of its toxic components, PVC is almost never recycled in the U.S., but University of Michigan researchers Danielle Fagnani and Anne McNeil have discovered a chemical process that can break it down into material that could be incorporated back into production. This could be a step toward a circular economy “that accounts for resource inputs and emissions throughout a product’s life cycle, including extraction of raw materials, manufacturing, transport, use and reuse, and disposal,” as medical experts have proposed. “It’s a failure of humanity to have created these amazing materials which have improved our lives in many ways, but at the same time to be so shortsighted that we didn’t think about what to do with the waste,” McNeil said in a press release.
Susanne Koch puts it more succinctly: “What’s the point if we save patients while killing the planet?”

In 2013, the Human Brain Project set out to build a realistic computer model of the brain over ten years. Now, experts are reflecting on HBP's achievements with an eye toward the future.
Scholars have found that the project did help advance neuroscience more than some detractors initially expected, specifically in the area of brain simulations and virtual models. Using an interdisciplinary approach of combining technology, such as AI and digital simulations, with neuroscience, the HBP worked to gain a deeper understanding of the human brain’s complicated structure and functions, which in some cases led to novel treatments for brain disorders. Lastly, through online platforms, the HBP spearheaded a previously unmatched level of global neuroscience collaborations.
Simulating a human brain stirs up controversy
Right from the start, the project was plagued with controversy and condemnation. One of its prominent critics was Yves Fregnac, a professor in cognitive science at the Polytechnic Institute of Paris and research director at the French National Centre for Scientific Research. Fregnac argued in numerous articles that the HBP was overfunded based on proposals with unrealistic goals. “This new way of over-selling scientific targets, deeply aligned with what modern society expects from mega-sciences in the broad sense (big investment, big return), has been observed on several occasions in different scientific sub-fields,” he wrote in one of his articles, “before invading the field of brain sciences and neuromarketing.”
"A human brain model can simulate an experiment a million times for many different conditions, but the actual human experiment can be performed only once or a few times," said Viktor Jirsa, a professor at Aix-Marseille University.
Responding to such critiques, the HBP worked to restructure the effort in its early days with new leadership, organization, and goals that were more flexible and attainable. “The HBP got a more versatile, pluralistic approach,” said Viktor Jirsa, a professor at Aix-Marseille University and one of the HBP lead scientists. He believes that these changes fixed at least some of HBP’s issues. “The project has been on a very productive and scientifically fruitful course since then.”
After restructuring, the HBP became a European hub on brain research, with hundreds of scientists joining its growing network. The HBP created projects focused on various brain topics, from consciousness to neurodegenerative diseases. HBP scientists worked on complex subjects, such as mapping out the brain, combining neuroscience and robotics, and experimenting with neuromorphic computing, a computational technique inspired by the human brain structure and function—to name just a few.
Simulations advance knowledge and treatment options
In 2013, it seemed that bringing neuroscience into a digital age would be farfetched, but research within the HBP has made this achievable. The virtual maps and simulations various HBP teams create through brain imaging data make it easier for neuroscientists to understand brain developments and functions. The teams publish these models on the HBP’s EBRAINS online platform—one of the first to offer access to such data to neuroscientists worldwide via an open-source online site. “This digital infrastructure is backed by high-performance computers, with large datasets and various computational tools,” said Lucy Xiaolu Wang, an assistant professor in the Resource Economics Department at the University of Massachusetts Amherst, who studies the economics of the HBP. That means it can be used in place of many different types of human experimentation.
Jirsa’s team is one of many within the project that works on virtual brain models and brain simulations. Compiling patient data, Jirsa and his team can create digital simulations of different brain activities—and repeat these experiments many times, which isn’t often possible in surgeries on real brains. “A human brain model can simulate an experiment a million times for many different conditions,” Jirsa explained, “but the actual human experiment can be performed only once or a few times.” Using simulations also saves scientists and doctors time and money when looking at ways to diagnose and treat patients with brain disorders.

Compiling patient data, scientists can create digital simulations of different brain activities—and repeat these experiments many times.
The Human Brain Project
Simulations can help scientists get a full picture that otherwise is unattainable. “Another benefit is data completion,” added Jirsa, “in which incomplete data can be complemented by the model. In clinical settings, we can often measure only certain brain areas, but when linked to the brain model, we can enlarge the range of accessible brain regions and make better diagnostic predictions.”
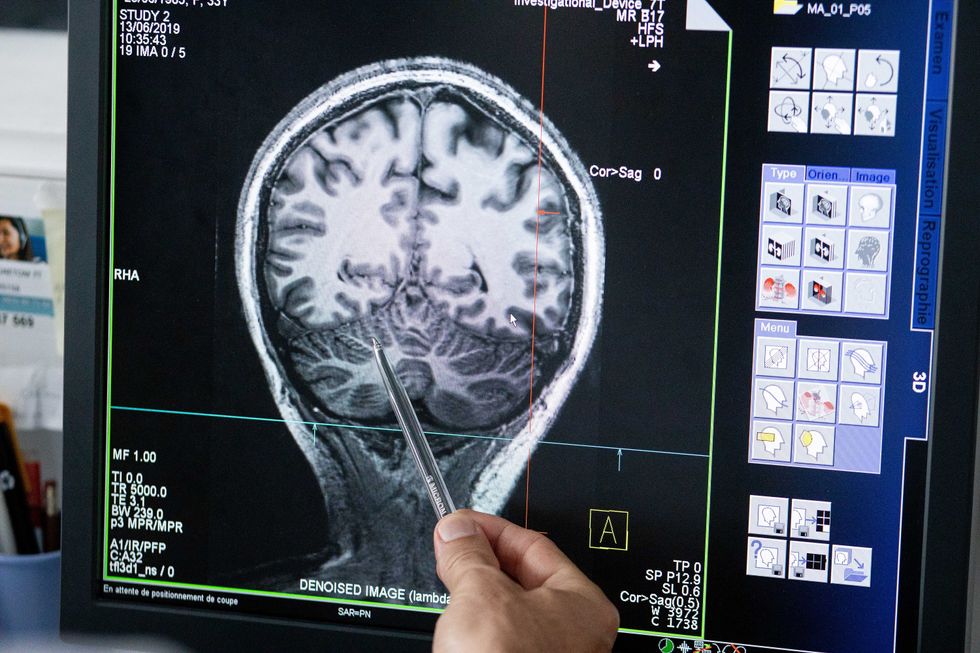
With time, Jirsa’s team was able to move into patient-specific simulations. “We advanced from generic brain models to the ability to use a specific patient’s brain data, from measurements like MRI and others, to create individualized predictive models and simulations,” Jirsa explained. He and his team are working on this personalization technique to treat patients with epilepsy. According to the World Health Organization, about 50 million people worldwide suffer from epilepsy, a disorder that causes recurring seizures. While some epilepsy causes are known others remain an enigma, and many are hard to treat. For some patients whose epilepsy doesn’t respond to medications, removing part of the brain where seizures occur may be the only option. Understanding where in the patients’ brains seizures arise can give scientists a better idea of how to treat them and whether to use surgery versus medications.
“We apply such personalized models…to precisely identify where in a patient’s brain seizures emerge,” Jirsa explained. “This guides individual surgery decisions for patients for which surgery is the only treatment option.” He credits the HBP for the opportunity to develop this novel approach. “The personalization of our epilepsy models was only made possible by the Human Brain Project, in which all the necessary tools have been developed. Without the HBP, the technology would not be in clinical trials today.”
Personalized simulations can significantly advance treatments, predict the outcome of specific medical procedures and optimize them before actually treating patients. Jirsa is watching this happen firsthand in his ongoing research. “Our technology for creating personalized brain models is now used in a large clinical trial for epilepsy, funded by the French state, where we collaborate with clinicians in hospitals,” he explained. “We have also founded a spinoff company called VB Tech (Virtual Brain Technologies) to commercialize our personalized brain model technology and make it available to all patients.”
The Human Brain Project created a level of interconnectedness within the neuroscience research community that never existed before—a network not unlike the brain’s own.
Other experts believe it’s too soon to tell whether brain simulations could change epilepsy treatments. “The life cycle of developing treatments applicable to patients often runs over a decade,” Wang stated. “It is still too early to draw a clear link between HBP’s various project areas with patient care.” However, she admits that some studies built on the HBP-collected knowledge are already showing promise. “Researchers have used neuroscientific atlases and computational tools to develop activity-specific stimulation programs that enabled paraplegic patients to move again in a small-size clinical trial,” Wang said. Another intriguing study looked at simulations of Alzheimer’s in the brain to understand how it evolves over time.
Some challenges remain hard to overcome even with computer simulations. “The major challenge has always been the parameter explosion, which means that many different model parameters can lead to the same result,” Jirsa explained. An example of this parameter explosion could be two different types of neurodegenerative conditions, such as Parkinson’s and Huntington’s diseases. Both afflict the same area of the brain, the basal ganglia, which can affect movement, but are caused by two different underlying mechanisms. “We face the same situation in the living brain, in which a large range of diverse mechanisms can produce the same behavior,” Jirsa said. The simulations still have to overcome the same challenge.
Understanding where in the patients’ brains seizures arise can give scientists a better idea of how to treat them and whether to use surgery versus medications.
The Human Brain Project
A network not unlike the brain’s own
Though the HBP will be closing this year, its legacy continues in various studies, spin-off companies, and its online platform, EBRAINS. “The HBP is one of the earliest brain initiatives in the world, and the 10-year long-term goal has united many researchers to collaborate on brain sciences with advanced computational tools,” Wang said. “Beyond the many research articles and projects collaborated on during the HBP, the online neuroscience research infrastructure EBRAINS will be left as a legacy even after the project ends.”
Those who worked within the HBP see the end of this project as the next step in neuroscience research. “Neuroscience has come closer to very meaningful applications through the systematic link with new digital technologies and collaborative work,” Jirsa stated. “In that way, the project really had a pioneering role.” It also created a level of interconnectedness within the neuroscience research community that never existed before—a network not unlike the brain’s own. “Interconnectedness is an important advance and prerequisite for progress,” Jirsa said. “The neuroscience community has in the past been rather fragmented and this has dramatically changed in recent years thanks to the Human Brain Project.”
According to its website, by 2023 HBP’s network counted over 500 scientists from over 123 institutions and 16 different countries, creating one of the largest multi-national research groups in the world. Even though the project hasn’t produced the in-silico brain as Markram envisioned it, the HBP created a communal mind with immense potential. “It has challenged us to think beyond the boundaries of our own laboratories,” Jirsa said, “and enabled us to go much further together than we could have ever conceived going by ourselves.”
