

A future app may help you avoid getting the flu by informing you of your local risk on a given day.
Applied mathematician Sara del Valle works at the U.S.'s foremost nuclear weapons lab: Los Alamos. Once colloquially called Atomic City, it's a hidden place 45 minutes into the mountains northwest of Santa Fe. Here, engineers developed the first atomic bomb.
Like AccuWeather, an app for disease prediction could help people alter their behavior to live better lives.
Today, Los Alamos still a small science town, though no longer a secret, nor in the business of building new bombs. Instead, it's tasked with, among other things, keeping the stockpile of nuclear weapons safe and stable: not exploding when they're not supposed to (yes, please) and exploding if someone presses that red button (please, no).
Del Valle, though, doesn't work on any of that. Los Alamos is also interested in other kinds of booms—like the explosion of a contagious disease that could take down a city. Predicting (and, ideally, preventing) such epidemics is del Valle's passion. She hopes to develop an app that's like AccuWeather for germs: It would tell you your chance of getting the flu, or dengue or Zika, in your city on a given day. And like AccuWeather, it could help people alter their behavior to live better lives, whether that means staying home on a snowy morning or washing their hands on a sickness-heavy commute.

Sara del Valle of Los Alamos is working to predict and prevent epidemics using data and machine learning.
Since the beginning of del Valle's career, she's been driven by one thing: using data and predictions to help people behave practically around pathogens. As a kid, she'd always been good at math, but when she found out she could use it to capture the tentacular spread of disease, and not just manipulate abstractions, she was hooked.
When she made her way to Los Alamos, she started looking at what people were doing during outbreaks. Using social media like Twitter, Google search data, and Wikipedia, the team started to sift for trends. Were people talking about hygiene, like hand-washing? Or about being sick? Were they Googling information about mosquitoes? Searching Wikipedia for symptoms? And how did those things correlate with the spread of disease?
It was a new, faster way to think about how pathogens propagate in the real world. Usually, there's a 10- to 14-day lag in the U.S. between when doctors tap numbers into spreadsheets and when that information becomes public. By then, the world has moved on, and so has the disease—to other villages, other victims.
"We found there was a correlation between actual flu incidents in a community and the number of searches online and the number of tweets online," says del Valle. That was when she first let herself dream about a real-time forecast, not a 10-days-later backcast. Del Valle's group—computer scientists, mathematicians, statisticians, economists, public health professionals, epidemiologists, satellite analysis experts—has continued to work on the problem ever since their first Twitter parsing, in 2011.
They've had their share of outbreaks to track. Looking back at the 2009 swine flu pandemic, they saw people buying face masks and paying attention to the cleanliness of their hands. "People were talking about whether or not they needed to cancel their vacation," she says, and also whether pork products—which have nothing to do with swine flu—were safe to buy.
At the latest meeting with all the prediction groups, del Valle's flu models took first and second place.
They watched internet conversations during the measles outbreak in California. "There's a lot of online discussion about anti-vax sentiment, and people trying to convince people to vaccinate children and vice versa," she says.
Today, they work on predicting the spread of Zika, Chikungunya, and dengue fever, as well as the plain old flu. And according to the CDC, that latter effort is going well.
Since 2015, the CDC has run the Epidemic Prediction Initiative, a competition in which teams like de Valle's submit weekly predictions of how raging the flu will be in particular locations, along with other ailments occasionally. Michael Johannson is co-founder and leader of the program, which began with the Dengue Forecasting Project. Its goal, he says, was to predict when dengue cases would blow up, when previously an area just had a low-level baseline of sick people. "You'll get this massive epidemic where all of a sudden, instead of 3,000 to 4,000 cases, you have 20,000 cases," he says. "They kind of come out of nowhere."
But the "kind of" is key: The outbreaks surely come out of somewhere and, if scientists applied research and data the right way, they could forecast the upswing and perhaps dodge a bomb before it hit big-time. Questions about how big, when, and where are also key to the flu.
A big part of these projects is the CDC giving the right researchers access to the right information, and the structure to both forecast useful public-health outcomes and to compare how well the models are doing. The extra information has been great for the Los Alamos effort. "We don't have to call departments and beg for data," says del Valle.
When data isn't available, "proxies"—things like symptom searches, tweets about empty offices, satellite images showing a green, wet, mosquito-friendly landscape—are helpful: You don't have to rely on anyone's health department.
At the latest meeting with all the prediction groups, del Valle's flu models took first and second place. But del Valle wants more than weekly numbers on a government website; she wants that weather-app-inspired fortune-teller, incorporating the many diseases you could get today, standing right where you are. "That's our dream," she says.

This plot shows the the correlations between the online data stream, from Wikipedia, and various infectious diseases in different countries. The results of del Valle's predictive models are shown in brown, while the actual number of cases or illness rates are shown in blue.
(Courtesy del Valle)
The goal isn't to turn you into a germophobic agoraphobe. It's to make you more aware when you do go out. "If you know it's going to rain today, you're more likely to bring an umbrella," del Valle says. "When you go on vacation, you always look at the weather and make sure you bring the appropriate clothing. If you do the same thing for diseases, you think, 'There's Zika spreading in Sao Paulo, so maybe I should bring even more mosquito repellent and bring more long sleeves and pants.'"
They're not there yet (don't hold your breath, but do stop touching your mouth). She estimates it's at least a decade away, but advances in machine learning could accelerate that hypothetical timeline. "We're doing baby steps," says del Valle, starting with the flu in the U.S., dengue in Brazil, and other efforts in Colombia, Ecuador, and Canada. "Going from there to forecasting all diseases around the globe is a long way," she says.
But even AccuWeather started small: One man began predicting weather for a utility company, then helping ski resorts optimize their snowmaking. His influence snowballed, and now private forecasting apps, including AccuWeather's, populate phones across the planet. The company's progression hasn't been without controversy—privacy incursions, inaccuracy of long-term forecasts, fights with the government—but it has continued, for better and for worse.
Disease apps, perhaps spun out of a small, unlikely team at a nuclear-weapons lab, could grow and breed in a similar way. And both the controversies and public-health benefits that may someday spin out of them lie in the future, impossible to predict with certainty.

The U.S. population is becoming more diverse, but clinical trials don't reflect that, experts say. Some are focusing on recruiting minorities to participate in research.
While racial and ethnic minority groups represent almost half of the U.S. population, the lack of diversity in clinical trials poses serious challenges. Limited awareness and access impede equitable representation, which is necessary to prove the safety and effectiveness of medical interventions across different groups.
A Yale University study on clinical trial diversity published last year in BMJ Medicine found that while 81 percent of trials testing the new cancer drugs approved by the U.S. Food and Drug Administration between 2012 and 2017 included women, only 23 percent included older adults and 5 percent fairly included racial and ethnic minorities. “It’s both a public health and social justice issue,” said Jennifer E. Miller, an associate professor of medicine at Yale School of Medicine. “We need to know how medicines and vaccines work for all clinically distinct groups, not just healthy young White males.” A recent JAMA Oncology editorial stresses out the need for legislation that would require diversity action plans for certain types of trials.
Ensuring meaningful representation of racial and ethnic minorities in clinical trials for regulated medical products is fundamental to public health.--FDA Commissioner Robert M. Califf.
But change is on the horizon. Last April, the FDA issued a new draft guidance encouraging industry to find ways to revamp recruitment into clinical trials. The announcement, which expanded on previous efforts, called for including more participants from underrepresented racial and ethnic segments of the population.
“The U.S. population has become increasingly diverse, and ensuring meaningful representation of racial and ethnic minorities in clinical trials for regulated medical products is fundamental to public health,” FDA commissioner Robert M. Califf, a physician, said in a statement. “Going forward, achieving greater diversity will be a key focus throughout the FDA to facilitate the development of better treatments and better ways to fight diseases that often disproportionately impact diverse communities. This guidance also further demonstrates how we support the Administration’s Cancer Moonshot goal of addressing inequities in cancer care, helping to ensure that every community in America has access to cutting-edge cancer diagnostics, therapeutics and clinical trials.”
Lola Fashoyin-Aje, associate director for Science and Policy to Address Disparities in the Oncology Center of Excellence at the FDA, said that the agency “has long held the view that clinical trial participants should reflect the clinical and demographic characteristics of the patients who will ultimately receive the drug once approved.” However, “numerous studies over many decades” have measured the extent of underrepresentation. One FDA analysis found that the proportion of White patients enrolled in U.S. clinical trials (88 percent) is much higher than their numbers in country's population. Meanwhile, the enrollment of African American and Native Hawaiian/American Indian and Alaskan Native patients is below their national numbers.
The FDA’s guidance is accelerating researchers’ efforts to be more inclusive of diverse groups in clinical trials, said Joyce Sackey, a clinical professor of medicine and associate dean at Stanford School of Medicine. Underrepresentation is “a huge issue,” she noted. Sackey is focusing on this in her role as the inaugural chief equity, diversity and inclusion officer at Stanford Medicine, which encompasses the medical school and two hospitals.
Until the early 1990s, Sackey pointed out, clinical trials were based on research that mainly included men, as investigators were concerned that women could become pregnant, which would affect the results. This has led to some unfortunate consequences, such as indications and dosages for drugs that cause more side effects in women due to biological differences. “We’ve made some progress in including women, but we have a long way to go in including people of different ethnic and racial groups,” she said.

A new mural outside Guadalupe Centers Middle School in Kansas City, Missouri, advocates for increasing diversity in clinical trials. Kim Jones, 51-year-old African American breast cancer survivor, is second on the left.
Artwork by Vania Soto. Photo by Megan Peters.
Among racial and ethnic minorities, distrust of clinical trials is deeply rooted in a history of medical racism. A prime example is the Tuskegee Study, a syphilis research experiment that started in 1932 and spanned 40 years, involving hundreds of Black men with low incomes without their informed consent. They were lured with inducements of free meals, health care and burial stipends to participate in the study undertaken by the U.S. Public Health Service and the Tuskegee Institute in Alabama.
By 1947, scientists had figured out that they could provide penicillin to help patients with syphilis, but leaders of the Tuskegee research failed to offer penicillin to their participants throughout the rest of the study, which lasted until 1972.
Opeyemi Olabisi, an assistant professor of medicine at Duke University Medical Center, aims to increase the participation of African Americans in clinical research. As a nephrologist and researcher, he is the principal investigator of a clinical trial focusing on the high rate of kidney disease fueled by two genetic variants of the apolipoprotein L1 (APOL1) gene in people of recent African ancestry. Individuals of this background are four times more likely to develop kidney failure than European Americans, with these two variants accounting for much of the excess risk, Olabisi noted.
The trial is part of an initiative, CARE and JUSTICE for APOL1-Mediated Kidney Disease, through which Olabisi hopes to diversify study participants. “We seek ways to engage African Americans by meeting folks in the community, providing accessible information and addressing structural hindrances that prevent them from participating in clinical trials,” Olabisi said. The researchers go to churches and community organizations to enroll people who do not visit academic medical centers, which typically lead clinical trials. Since last fall, the initiative has screened more than 250 African Americans in North Carolina for the genetic variants, he said.
Other key efforts are underway. “Breaking down barriers, including addressing access, awareness, discrimination and racism, and workforce diversity, are pivotal to increasing clinical trial participation in racial and ethnic minority groups,” said Joshua J. Joseph, assistant professor of medicine at the Ohio State University Wexner Medical Center. Along with the university’s colleges of medicine and nursing, researchers at the medical center partnered with the African American Male Wellness Agency, Genentech and Pfizer to host webinars soliciting solutions from almost 450 community members, civic representatives, health care providers, government organizations and biotechnology professionals in 25 states and five countries.
Their findings, published in February in the journal PLOS One, suggested that including incentives or compensation as part of the research budget at the institutional level may help resolve some issues that hinder racial and ethnic minorities from participating in clinical trials. Compared to other groups, more Blacks and Hispanics have jobs in service, production and transportation, the authors note. It can be difficult to get paid leave in these sectors, so employees often can’t join clinical trials during regular business hours. If more leaders of trials offer money for participating, that could make a difference.
Obstacles include geographic access, language and other communications issues, limited awareness of research options, cost and lack of trust.
Christopher Corsico, senior vice president of development at GSK, formerly GlaxoSmithKline, said the pharmaceutical company conducted a 17-year retrospective study on U.S. clinical trial diversity. “We are using epidemiology and patients most impacted by a particular disease as the foundation for all our enrollment guidance, including study diversity plans,” Corsico said. “We are also sharing our results and ideas across the pharmaceutical industry.”
Judy Sewards, vice president and head of clinical trial experience at Pfizer’s headquarters in New York, said the company has committed to achieving racially and ethnically diverse participation at or above U.S. census or disease prevalence levels (as appropriate) in all trials. “Today, barriers to clinical trial participation persist,” Sewards said. She noted that these obstacles include geographic access, language and other communications issues, limited awareness of research options, cost and lack of trust. “Addressing these challenges takes a village. All stakeholders must come together and work collaboratively to increase diversity in clinical trials.”
It takes a village indeed. Hope Krebill, executive director of the Masonic Cancer Alliance, the outreach network of the University of Kansas Cancer Center in Kansas City, which commissioned the mural, understood that well. So her team actively worked with their metaphorical “village.” “We partnered with the community to understand their concerns, knowledge and attitudes toward clinical trials and research,” said Krebill. “With that information, we created a clinical trials video and a social media campaign, and finally, the mural to encourage people to consider clinical trials as an option for care.”
Besides its encouraging imagery, the mural will also be informational. It will include a QR code that viewers can scan to find relevant clinical trials in their location, said Vania Soto, a Mexican artist who completed the rendition in late February. “I’m so honored to paint people that are survivors and are living proof that clinical trials worked for them,” she said.
Jones, the cancer survivor depicted in the mural, hopes the image will prompt people to feel more open to partaking in clinical trials. “Hopefully, it will encourage people to inquire about what they can do — how they can participate,” she said.

Drones are just one of several new technologies that are rising to the challenge of more frequent wildfires.
Robots have been a game-changer. Inspired by Paris, the Los Angeles Fire Department (LAFD) was the first in the U.S. to deploy a firefighting robot in 2021, the Thermite Robotics System 3 – RS3, for short.
RS3 is a 3,500-pound turbine on a crawler—the size of a Smart car—with a 36.8 horsepower engine that can go for 20 hours without refueling. It can plow through hazardous terrain, move cars from its path, and pull an 8,000-pound object from a fire.
All that while spurting 2,500 gallons of water per minute with a rear exhaust fan clearing the smoke. At a recent trade show, RS3 was billed as equivalent to 10 firefighters. The Los Angeles Times referred to it as “a droid on steroids.”

Robots such as the Thermite RS3 can plow through hazardous terrain and pull an 8,000-pound object from a fire.
Los Angeles Fire Department
The advantage of the robot is obvious. Operated remotely from a distance, it greatly reduces an emergency responder’s exposure to danger, says Wade White, assistant chief of the LAFD. The robot can be sent into airplane fires, nuclear reactors, hazardous areas with carcinogens (think East Palestine, Ohio), or buildings where a roof collapse is imminent.
Advances for firefighters are taking many other forms as well. Fibers have been developed that make the firefighter’s coat lighter and more protective from carcinogens. New wearable devices track firefighters’ biometrics in real time so commanders can monitor their heat stress and exertion levels. A sensor patch is in development which takes readings every four seconds to detect dangerous gases such as methane and carbon dioxide. A sonic fire extinguisher is being explored that uses low frequency soundwaves to remove oxygen from air molecules without unhealthy chemical compounds.
The demand for this technology is only increasing, especially with the recent rise in wildfires. In 2021, fires were responsible for 3,800 deaths and 14,700 injuries of civilians in this country. Last year, 68,988 wildfires burned down 7.6 million acres. Whether the next generation of firefighting can address these new challenges could depend on special cameras, robots of the aerial variety, AI and smart systems.
Fighting fire with cameras
Another key innovation for firefighters is a thermal imaging camera (TIC) that improves visibility through smoke. “At a fire, you might not see your hand in front of your face,” says White. “Using the TIC screen, you can find the door to get out safely or see a victim in the corner.” Since these cameras were introduced in the 1990s, the price has come down enough (from $10,000 or more to about $700) that every LAFD firefighter on duty has been carrying one since 2019, says White.
TICs are about the size of a cell phone. The camera can sense movement and body heat so it is ideal as a search tool for people trapped in buildings. If a firefighter has not moved in 30 seconds, the motion detector picks that up, too, and broadcasts a distress signal and directional information to others.
To enable firefighters to operate the camera hands-free, the newest TICs can attach inside a helmet. The firefighter sees the images inside their mask.
TICs also can be mounted on drones to get a bird’s-eye, 360 degree view of a disaster or scout for hot spots through the smoke. In addition, the camera can take photos to aid arson investigations or help determine the cause of a fire.
More help From above
Firefighters prefer the term “unmanned aerial systems” (UAS) to drones to differentiate them from military use.
A UAS carrying a camera can provide aerial scene monitoring and topography maps to help fire captains deploy resources more efficiently. At night, floodlights from the drone can illuminate the landscape for firefighters. They can drop off payloads of blankets, parachutes, life preservers or radio devices for stranded people to communicate, too. And like the robot, the UAS reduces risks for ground crews and helicopter pilots by limiting their contact with toxic fumes, hazardous chemicals, and explosive materials.
“The nice thing about drones is that they perform multiple missions at once,” says Sean Triplett, team lead of fire and aviation management, tools and technology at the Forest Service.
Experts predict we’ll see swarms of drones dropping water and fire retardant on burning buildings and forests in the near future.
The UAS is especially helpful during wildfires because it can track fires, get ahead of wind currents and warn firefighters of wind shifts in real time. The U.S. Forest Service also uses long endurance, solar-powered drones that can fly for up to 30 days at a time to detect early signs of wildfire. Wildfires are no longer seasonal in California – they are a year-long threat, notes Thanh Nguyen, fire captain at the Orange County Fire Authority.
In March, Nguyen’s crew deployed a drone to scope out a huge landslide following torrential rains in San Clemente, CA. Emergency responders used photos and videos from the drone to survey the evacuated area, enabling them to stay clear of ground on the hillside that was still sliding.
Improvements in drone batteries are enabling them to fly for longer with heavier payloads. Experts predict we’ll see swarms of drones dropping water and fire retardant on burning buildings and forests in the near future.
AI to the rescue
The biggest peril for a firefighter is often what they don’t see coming. Flashovers are a leading cause of firefighter deaths, for example. They occur when flammable materials in an enclosed area ignite almost instantaneously. Or dangerous backdrafts can happen when a firefighter opens a window or door; the air rushing in can ignite a fire without warning.
The Fire Fighting Technology Group at the National Institute of Standards and Technology (NIST) is developing tools and systems to predict these potentially lethal events with computer models and artificial intelligence.
Partnering with other institutions, NIST researchers developed the Flashover Prediction Neural Network (FlashNet) after looking at common house layouts and running sets of scenarios through a machine-learning model. In the lab, FlashNet was able to predict a flashover 30 seconds before it happened with 92.1% success. When ready for release, the technology will be bundled with sensors that are already installed in buildings, says Anthony Putorti, leader of the NIST group.
The NIST team also examined data from hundreds of backdrafts as a basis for a machine-learning model to predict them. In testing chambers the model predicted them correctly 70.8% of the time; accuracy increased to 82.4% when measures of backdrafts were taken in more positions at different heights in the chambers. Developers are working on how to integrate the AI into a small handheld device that can probe the air of a room through cracks around a door or through a created opening, Putorti says. This way, the air can be analyzed with the device to alert firefighters of any significant backdraft risk.
Early wildfire detection technologies based on AI are in the works, too. The Forest Service predicts the acreage burned each year during wildfires will more than triple in the next 80 years. By gathering information on historic fires, weather patterns, and topography, says White, AI can help firefighters manage wildfires before they grow out of control and create effective evacuation plans based on population data and fire patterns.
The future is connectivity
We are in our infancy with “smart firefighting,” says Casey Grant, executive director emeritus of the Fire Protection Research Foundation. Grant foresees a new era of cyber-physical systems for firefighters—a massive integration of wireless networks, advanced sensors, 3D simulations, and cloud services. To enhance teamwork, the system will connect all branches of emergency responders—fire, emergency medical services, law enforcement.
FirstNet (First Responder Network Authority) now provides a nationwide high-speed broadband network with 5G capabilities for first responders through a terrestrial cell network. Battling wildfires, however, the Forest Service needed an alternative because they don’t always have access to a power source. In 2022, they contracted with Aerostar for a high altitude balloon (60,000 feet up) that can extend cell phone power and LTE. “It puts a bubble of connectivity over the fire to hook in the internet,” Triplett explains.
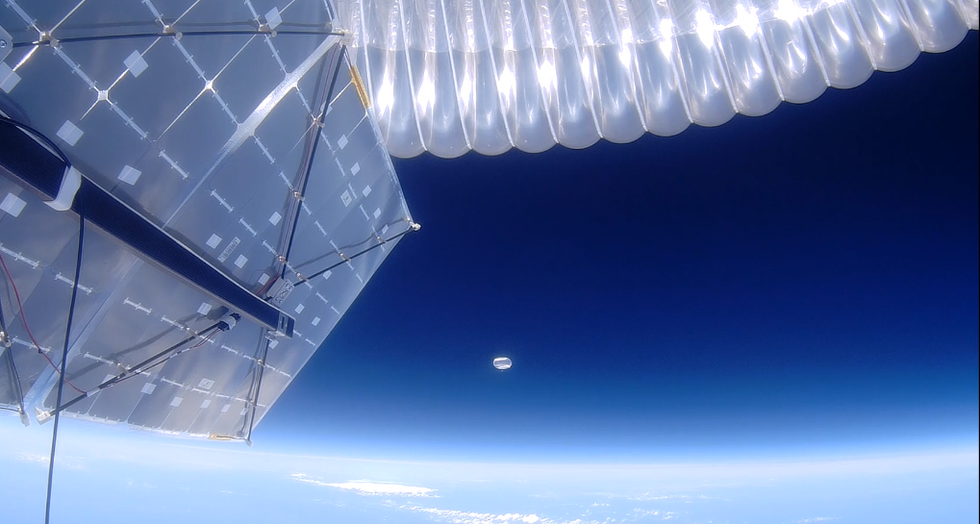
A high altitude balloon, 60,000 feet high, can extend cell phone power and LTE, putting a "bubble" of internet connectivity over fires.
Courtesy of USDA Forest Service
Advances in harvesting, processing and delivering data will improve safety and decision-making for firefighters, Grant sums up. Smart systems may eventually calculate fire flow paths and make recommendations about the best ways to navigate specific fire conditions. NIST’s plan to combine FlashNet with sensors is one example.
The biggest challenge is developing firefighting technology that can work across multiple channels—federal, state, local and tribal systems as well as for fire, police and other emergency services— in any location, says Triplett. “When there’s a wildfire, there are no political boundaries,” he says. “All hands are on deck.”