

Anita Freeman, left, hugs her sister Elizabeth Martin at a bakery in Huntington Beach, California, in 2009 — a year before Elizabeth's cancer diagnosis. (Courtesy Anita Freeman)
For five weeks, Anita Freeman watched her sister writhe in pain. The colon cancer diagnosed four years earlier became metastatic.
"I still wouldn't wish that ending on my worst enemy."
At this tormenting juncture, her 66-year-old sister, Elizabeth Martin, wanted to die comfortably in her sleep. But doctors wouldn't help fulfill that final wish.
"It haunts me," Freeman, 74, who lives in Long Beach, California, says in recalling the prolonged agony. Her sister "was breaking out of the house and running in her pajamas down the sidewalk, screaming, 'Help me. Help me.' She just went into a total panic."
Finally, a post-acute care center offered pentobarbital, a sedative that induced a state of unconsciousness, but only after an empathetic palliative care doctor called and insisted on ending the inhumane suffering. "We even had to fight the owners of the facility to get them to agree to the recommendations," Freeman says, describing it as "the only option we had at that time; I still wouldn't wish that ending on my worst enemy."
Her sister died a week later, in 2014. That was two years before California's medical aid-in-dying law took effect, making doctors less reliant on palliative sedation to peacefully end unbearable suffering for terminally ill patients. Now, Freeman volunteers for Compassion & Choices, a national grassroots organization based in Portland, Oregon, that advocates for expanding end-of-life options.
Palliative sedation involves medicating a terminally ill patient into lowered awareness or unconsciousness in order to relieve otherwise intractable suffering at the end of life. It is not intended to cause death, which occurs due to the patient's underlying disease.
In contrast, euthanasia involves directly and deliberately ending a patient's life. Euthanasia is legal only in Canada and some European countries and requires a health care professional to administer the medication. In the United States, laws in seven states and Washington, D.C. give terminally ill patients the option to obtain prescription medication they can take to die peacefully in their sleep, but they must be able to self-adminster it.
Recently, palliative sedation has been gaining more acceptance among medical professionals as an occasional means to relieve suffering, even if it may advance the time of death, as some clinicians believe. However, studies have found no evidence of this claim. Many doctors and bioethicists emphasize that intent is what distinguishes palliative sedation from euthanasia. Others disagree. It's common for controversy to swirl around when and how to apply this practice.

Elizabeth Martin with her sister Anita Freeman in happier times, before metastatic cancer caused her tremendous suffering at the end of her life.
(Courtesy Anita Freeman)
"Intent is everything in ethics. The rigor and protocols we have around palliative sedation therapy also speaks to it being an intervention directed to ease refractory distress," says Martha Twaddle, medical director of palliative medicine and supportive care at Northwestern University's Lake Forest Hospital in Lake Forest, Illinois.
Palliative sedation should be considered only when pain, shortness of breath, and other unbearable symptoms don't respond to conventional treatments. Left to his or her own devices, a patient in this predicament could become restless, Twaddle says, noting that "agitated delirium is a horrible symptom for a family to witness."
At other times, "we don't want to be too quick to sedate," particularly in cases of purely "existential distress"—when a patient experiences anticipatory grief around "saying goodbye" to loved ones, she explains. "We want to be sure we're applying the right therapy for the problem."
Encouraging patients to reconcile with their kin may help them find inner peace. Nonmedical interventions worth exploring include quieting the environment and adjusting lighting to simulate day and night, Twaddle says.
Music-thanatology also can have a calming effect. It is live, prescriptive music, mainly employing the harp or voice, tailored to the patient's physiological needs by tuning into vital signs such as heart rate, respiration, and temperature, according to the Music-Thanatology Association International.
"When we integrated this therapeutic modality in 2003, our need for using palliative sedation therapy dropped 75 percent and has remained low ever since," Twaddle observes. "We have this as part of our care for treating refractory symptoms."
"If palliative sedation is being employed properly with the right patient, it should not hasten death."
Ethical concerns surrounding euthanasia often revolve around the term "terminal sedation," which "can entail a physician deciding that the patient is a lost cause—incurable medically and in substantial pain that cannot adequately be relieved," says John Kilner, professor and director of the bioethics programs at Trinity International University in Deerfield, Illinois.
By halting sedation at reasonable intervals, the care team can determine whether significant untreatable pain persists. Periodic discontinuation serves as "evidence that the physician is still working to restore the patient rather than merely to usher the patient painlessly into death," Kilner explains. "Indeed, sometimes after a period of unconsciousness, with the body relieved of unceasing pain, the body can recover enough to make the pain treatable."
The medications for palliative sedation "are tried and true sedatives that we've had for a long time, for many years, so they're predictable," says Joe Rotella, chief medical officer at the American Academy of Hospice and Palliative Medicine.
Some patients prefer to keep their eyes open and remain conscious to answer by name, while others tell their doctors in advance that they want to be more heavily sedated while receiving medications to manage pain and other symptoms. "We adjust the dosage until the patient is sleeping at a desired level of sedation," Rotella says.
Sedation is an intrinsic side effect of most medications prescribed to control severe symptoms in terminally ill patients. In general, most people die in a sleepy state, except for instances of sudden, dramatic death resulting from a major heart attack or stroke, says Ryan R. Nash, a palliative medicine physician and director of The Ohio State University Center for Bioethics in Columbus.
"Using those medications to treat pain or shortness of breath is not palliative sedation," Nash says. In addition, providing supplemental nutrition and hydration in situations where death is imminent—with a prognosis limited to hours or days—generally doesn't help prolong life. "If palliative sedation is being employed properly with the right patient," he adds, "it should not hasten death."
Nonetheless, hospice nurses sometimes feel morally distressed over carrying out palliative sedation. Implementing protocols at health systems would help guide them and alleviate some of their concerns, says Gregg VandeKieft, medical director for palliative care at Providence St. Joseph Health's Southwest Washington Region in Olympia, Washington. "It creates guardrails by sort of standardizing and normalizing things," he says.
"Our goal is to restore our patient. It's never to take their life."
The concept of proportionality weighs heavily in the process of palliative sedation. But sometimes substantial doses are necessary. For instance, an opioid-tolerant patient recently needed an unusually large amount of medication to control symptoms. She was in a state of illness-induced confusion and pain, says David E. Smith, a palliative medicine physician at Baptist Health Supportive Care in Little Rock, Arkansas.
Still, "we are parsimonious in what we do. We only use as much therapeutic force as necessary to achieve our goals," Smith says. "Our goal is to restore our patient. It's never to take their life."

The test tubes contain tiny DNA/enzyme-based circuits, which comprise TRUMPET, a new type of electronic device, smaller than a cell.
While a computer gives these inputs in binary code or "bits," such as a 0 or 1, biocomputing uses DNA strands as inputs, whether double or single-stranded, and often uses fluorescent RNA as an output.
Adamala’s research focuses on developing such biocomputing systems using DNA, RNA, proteins, and lipids. Using these molecules in the biocomputing systems allows the latter to be biocompatible with the human body, resulting in a natural healing process. In a recent Nature Communications study, Adamala and her team created a new biocomputing platform called TRUMPET (Transcriptional RNA Universal Multi-Purpose GatE PlaTform) which acts like a DNA-powered computer chip. “These biological systems can heal if you design them correctly,” adds Adamala. “So you can imagine a computer that will eventually heal itself.”
The basics of biocomputing
Biocomputing and regular computing have many similarities. Like regular computing, biocomputing works by running information through a series of gates, usually logic gates. A logic gate works as a fork in the road for an electronic circuit. The input will travel one way or another, giving two different outputs. An example logic gate is the AND gate, which has two inputs (A and B) and two different results. If both A and B are 1, the AND gate output will be 1. If only A is 1 and B is 0, the output will be 0 and vice versa. If both A and B are 0, the result will be 0. While a computer gives these inputs in binary code or "bits," such as a 0 or 1, biocomputing uses DNA strands as inputs, whether double or single-stranded, and often uses fluorescent RNA as an output. In this case, the DNA enters the logic gate as a single or double strand.
If the DNA is double-stranded, the system “digests” the DNA or destroys it, which results in non-fluorescence or “0” output. Conversely, if the DNA is single-stranded, it won’t be digested and instead will be copied by several enzymes in the biocomputing system, resulting in fluorescent RNA or a “1” output. And the output for this type of binary system can be expanded beyond fluorescence or not. For example, a “1” output might be the production of the enzyme insulin, while a “0” may be that no insulin is produced. “This kind of synergy between biology and computation is the essence of biocomputing,” says Stephanie Forrest, a professor and the director of the Biodesign Center for Biocomputing, Security and Society at Arizona State University.
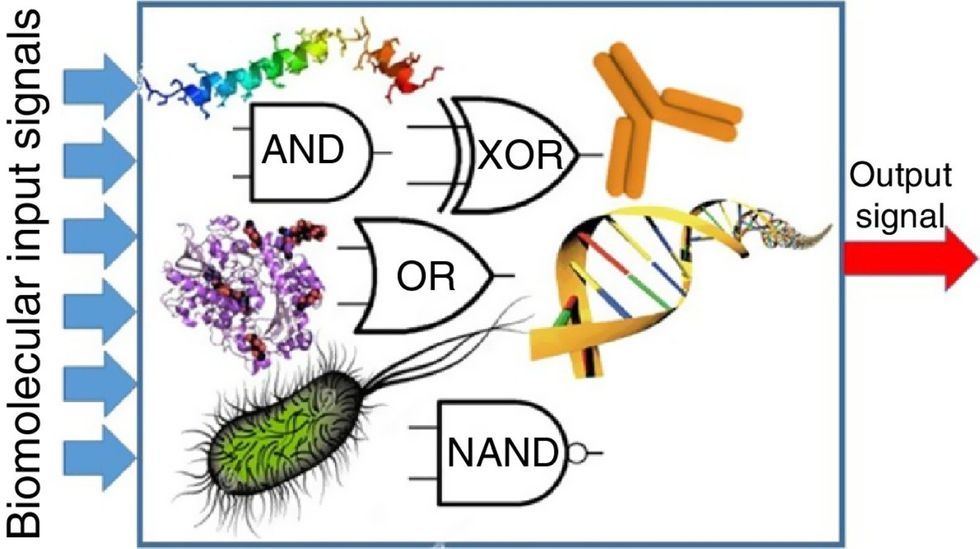
Biocomputing circles are made of DNA, RNA, proteins and even bacteria.
Evgeny Katz
The TRUMPET’s promise
Depending on whether the biocomputing system is placed directly inside a cell within the human body, or run in a test-tube, different environmental factors play a role. When an output is produced inside a cell, the cell's natural processes can amplify this output (for example, a specific protein or DNA strand), creating a solid signal. However, these cells can also be very leaky. “You want the cells to do the thing you ask them to do before they finish whatever their businesses, which is to grow, replicate, metabolize,” Adamala explains. “However, often the gate may be triggered without the right inputs, creating a false positive signal. So that's why natural logic gates are often leaky." While biocomputing outside a cell in a test tube can allow for tighter control over the logic gates, the outputs or signals cannot be amplified by a cell and are less potent.
TRUMPET, which is smaller than a cell, taps into both cellular and non-cellular biocomputing benefits. “At its core, it is a nonliving logic gate system,” Adamala states, “It's a DNA-based logic gate system. But because we use enzymes, and the readout is enzymatic [where an enzyme replicates the fluorescent RNA], we end up with signal amplification." This readout means that the output from the TRUMPET system, a fluorescent RNA strand, can be replicated by nearby enzymes in the platform, making the light signal stronger. "So it combines the best of both worlds,” Adamala adds.
These organic-based systems could detect cancer cells or low insulin levels inside a patient’s body.
The TRUMPET biocomputing process is relatively straightforward. “If the DNA [input] shows up as single-stranded, it will not be digested [by the logic gate], and you get this nice fluorescent output as the RNA is made from the single-stranded DNA, and that's a 1,” Adamala explains. "And if the DNA input is double-stranded, it gets digested by the enzymes in the logic gate, and there is no RNA created from the DNA, so there is no fluorescence, and the output is 0." On the story's leading image above, if the tube is "lit" with a purple color, that is a binary 1 signal for computing. If it's "off" it is a 0.
While still in research, TRUMPET and other biocomputing systems promise significant benefits to personalized healthcare and medicine. These organic-based systems could detect cancer cells or low insulin levels inside a patient’s body. The study’s lead author and graduate student Judee Sharon is already beginning to research TRUMPET's ability for earlier cancer diagnoses. Because the inputs for TRUMPET are single or double-stranded DNA, any mutated or cancerous DNA could theoretically be detected from the platform through the biocomputing process. Theoretically, devices like TRUMPET could be used to detect cancer and other diseases earlier.
Adamala sees TRUMPET not only as a detection system but also as a potential cancer drug delivery system. “Ideally, you would like the drug only to turn on when it senses the presence of a cancer cell. And that's how we use the logic gates, which work in response to inputs like cancerous DNA. Then the output can be the production of a small molecule or the release of a small molecule that can then go and kill what needs killing, in this case, a cancer cell. So we would like to develop applications that use this technology to control the logic gate response of a drug’s delivery to a cell.”
Although platforms like TRUMPET are making progress, a lot more work must be done before they can be used commercially. “The process of translating mechanisms and architecture from biology to computing and vice versa is still an art rather than a science,” says Forrest. “It requires deep computer science and biology knowledge,” she adds. “Some people have compared interdisciplinary science to fusion restaurants—not all combinations are successful, but when they are, the results are remarkable.”

Crickets are low on fat, high on protein, and can be farmed sustainably. They are also crunchy.
Listen on Apple | Listen on Spotify | Listen on Stitcher | Listen on Amazon | Listen on Google
Further reading:
More info on Bicky Nguyen
https://yseali.fulbright.edu.vn/en/faculty/bicky-n...
The environmental footprint of beef production
https://www.earthsave.org/environment.htm
https://www.watercalculator.org/news/articles/beef-king-big-water-footprints/
https://www.frontiersin.org/articles/10.3389/fsufs.2019.00005/full
https://ourworldindata.org/carbon-footprint-food-methane
Insect farming as a source of sustainable protein
https://www.insectgourmet.com/insect-farming-growing-bugs-for-protein/
https://www.sciencedirect.com/topics/agricultural-and-biological-sciences/insect-farming
Cricket flour is taking the world by storm
https://www.cricketflours.com/
https://talk-commerce.com/blog/what-brands-use-cricket-flour-and-why/
